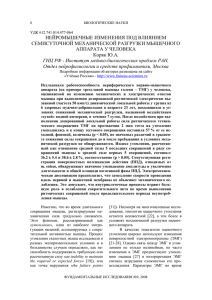
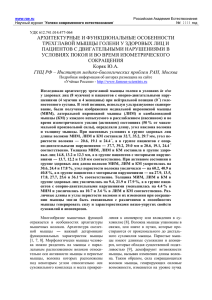
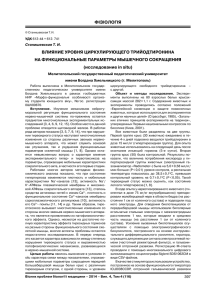
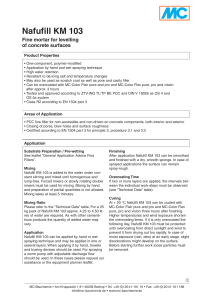
Cosmetic Commentary Journal of Cosmetic Dermatology, 15, 566--574 Specific aspects of a combined approach to male face correction: botulinum toxin A and volumetric fillers Max-Adam Scherer, MD* Clinic of High Aesthetic Medicine, Moscow, Russia Summary Cosmetologists in the last decade face a permanently increasing number of male patients. The necessity of a gender-adjusted approach in treatment of this patient category is obvious. An adequate correction requires consideration of the anatomic and physiologic features of male faces together with a whole set of interrelated aspects of psychologic perception of the male face esthetics, socially formed understanding of masculine features and appropriate emotional expressions, also of the motivations and expectations of men coming to a cosmetologist. The author explains in detail the elaborated out of own vast experience methods of complex male face correction using the above-mentioned gender-specific approach to create a naturally looking and harmonic facial expression and appearance. The presented botulinum therapy specifics concern the injection point location and toxin doses for every point. As a result, a rather distinct smoothening of the skin profile without detriment to the facial expressiveness and gender-related features is achieved. The importance and methods of an extremely delicate approach to volumetric plasty with stabilized hyaluronic acid-based fillers in men for avoiding hypercorrection and retaining the gender-specific features are discussed. Keywords: male face correction, gender-specific approach, botulinum toxin A, hyaluronic acid filler, natural look Introduction Cosmetologists in the last decade face a permanently increasing number of male patients. This places the topic of a gender-specific esthetic correction on the agenda. The concept of a gender-specific approach encompasses consideration of the differences in anatomic, physiologic, and esthetic features of male and female faces, socially formed perception of masculinity and femininity *Plastic surgeon, cosmetic dermatologist, rejuvenation injection methods specialist in private practice. Correspondence: Max-Adam Scherer, Clinic of High Aesthetic Medicine, Bolshoy Karetnyy lane 24/2, Moscow 127051, Russia. E-mail: dr.max.adam.scherer@gmail.com Accepted for publication May 11, 2016 566 attributes, differences in motivations of men and women, their behavior and emotional expression. From a psychological point of view, the appearance of a male person directly represents his gender role, identity and corresponds to social status, although congenital anthropometric and anatomic–physiological parameters such as facial skeletal proportions, skin texture, intensity of sebum production, and other remain in the background. Often even age-related changes are being ignored as such. For males, “to look younger” implies an intention to accentuate their successfulness and importance in the presence of younger men, unconsciously percepted as competitors, and to demonstrate wealthiness and sex appeal when communicating with women. The majority of men strive for a trustworthy look to impress surrounding people, especially business © 2016 Wiley Periodicals, Inc. Specific aspects of combined male face correction partners, in a positive way. That is why slightly noticeable wrinkles on the forehead and between eyebrows give the male appearance an air of proficiency and are percepted as signs of concentration and attentiveness. If women want to completely “erase” the signs of aging from their faces, men, on the contrary, need a “very slight” rejuvenation, that is, to eliminate precisely those features, which can be percepted as signs of sickness, weariness, and indifference. The goal of a cosmetologist is to limit facial expressiveness, to reduce wrinkles which make the face look older and unkempt, to restore the important for gender imaging volumetric parameters, nevertheless avoiding an ideal “childish” smoothness. Psychologists point out that childish features enhance the attractiveness of a female face, but by no means of a male appearance.1 General considerations Most often, men come to a cosmetologist to eliminate expressive static or/and dynamic wrinkles. Injections of botulinum toxin type A (BTA) allow to solve the problem effectively with a fast and relatively long-lasting effect; therefore, the treatment has become perhaps the most popular with this patient category. My experience shows that a gender-specific approach comprises an adjustment of the toxin dosage and an alteration of dose distribution among the injection points, also different placement of the points to guide the propagation/diffusion of BTA. These alterations are determined namely by the anatomic–topographical and physiological distinctions of a male face, for example, men often have very conspicuous superciliary arches, and this gives the face a stern, rough look. If such a gender-specific feature is present, BTA should not be injected into the frontalis muscle in big (“masculine”) doses to avoid transformation of roughness into surliness. The use of minimally sufficient BTA doses for male face correction complies with the trends of modern esthetic botulinum therapy. Nowadays, absence of facial expressiveness is regarded as not desirable, and the goal of correction is to achieve regression of expressive wrinkles along with retaining a sufficient, harmonic, and natural facial expressiveness.2 Moreover, quite young men aged 30–40 with the clinical picture of a “grumpy” or “tired” face seek our help with increasing frequency. They express a wish to get rid of wrinkles – not only static, but also dynamic – on the forehead and in the interbrow area. In this case, a cosmetologist faces particularly the necessity to limit the activity of facial expressive muscles. One more © 2016 Wiley Periodicals, Inc. . M-A Scherer aspect – a visit to the cosmetologist must “remain inconspicuous”, otherwise a noticeable correction of esthetic problems/signs of aging may be perceived by others as a failure and cause disapproval. Before considering technical aspects, I would like to emphasize the importance of a comprehensive approach to the problems with wrinkles on the forehead, in the periorbital area and between eyebrows in men, including a correction/fixation of the brow position and shape to avoid both eyebrow ptosis and a “female-type” rise. I reduce BTA with a slightly less solvent volume: 2 mL of saline (instead of 2.5 mL) for a standard BTA amount of 500 U. Such a dilution grade allows to precisely forecast and limit the solution propagation and toxin diffusion areas. This helps to achieve good injection results especially in men because of a slightly higher BTA concentration. Volumetric face plasty with fillers mostly based on stabilized hyaluronic acid is another equally popular procedure (Fig. 1). I widely use in my practice preparations of cross-linked stabilized hyaluronic acid (HA) which allow for a natural, harmonic, and predictable outcome of the volumetric correction that lasts for the period of 12–18 months. Volumetric filler injections are indicated not only for mature-aged men. Quite young patients presenting the clinical picture of a “tired look” with hypotrophy in the temporal, malar, and suborbital areas, deep nasolabial folds are also treated with this method. Genderspecific aspects of the face can also be accentuated through volumetric filler injections in the mandibular angle and mental areas. It must be pointed out that in volumetric plasty, the filler must be introduced exactly into a definite adipose Figure 1 The main zones of volumetric filler injections in men. 567 Specific aspects of combined male face correction . M-A Scherer compartment showing constitutional or age-related atrophy. Successful correction is based on knowledge of topographic anatomy of the fat regions that provide structural support for the overlying soft tissues,3 and a clear comprehension of the appropriate HA gel dosing, taking into account specific volumetric features of the preparation selected for the procedure. A modeling is performed within the target adipose compartment or in the subcutaneous adipose tissue to ensure an even distribution of the preparation and a natural look. I point out that the volumetric preparations of cross-linked stabilized HA should not be introduced interdermally; it must be injected only in the subcutaneous or deep adipose tissue. Let us discuss with more detail the correction of key areas. The forehead and the interbrow area correction Botulinum therapy The morphologic features of a male forehead are the following: It is more receding, wider, and often higher than a female forehead. Frontal protuberances are usually smoothed, and the superciliary arches are conspicuous. Facial expressive motility in a male forehead is rather high, and horizontal wrinkles appear early: begin to show or are already formed at the age of 20–25. Often such wrinkles are related to habitual glowering. The frontalis muscle in men is not only more pronouncedly active, but also stronger than in women. An increase in the standard BTA dose seems therefore to make sense. But this would impair the achievement of a natural result: A smooth “childish” forehead creates an air of serenity – not typical for men and undesired by them. Moreover, the approach with bigger doses increases the risk of iatrogenic brow ptosis. Another important point is that horizontal wrinkles on the forehead are seldom corrected alone, because their formation and, further, elimination are associated with the activity of muscles in the interbrow area – the most motile and emotionally expressive zone in men. In course of botulinum therapy, it is necessary to maintain a harmonic activity correlation of the levator – frontalis muscle – and the depressors – muscles of the interbrow area (the brow crimpling muscle – corrugator; the brow-lowering muscle and the procerus muscle) and to avoid unplanned compensatory muscle activation.4 This is achieved through rational placement of the injection points and reasonable choice of 568 Figure 2 The zone of the upper face third: drawing of the dynamic topographic net. The layout shows botulinum toxin type A doses for each rectangle, and also the distribution of doses for injection points in the interbrow area. BTA dosages. The activity and strength of expressive muscles, their anatomic–topographical features should be evaluated prior to introduction of the preparation. It is facilitated by use of a dynamic topographic net system that I have elaborated (Fig. 2). Step one in correction of forehead wrinkles is to locate the borders of the epicranial tendinous aponeurosis. To visualize the muscle volume, strength, and activity and to locate the aponeurosis borders, a series of tests is accomplished. In particular, the patient is requested to rise the brows high (to show surprise) several times. This shows the position of a point important for the correction of this area – let us call it “the aponeurosis point” (AP). This point indicates the lowest location of the aponeurosis: Demonstration of surprise forms no wrinkles in the central part of the forehead above this point. When building the dynamic net, the patient is first of all requested to show surprise and the universal AP is marked (the “x” mark in Fig. 2). When the patient frowns and squints, the points of maximum brow head motility, of maximal brow curvature, and points of the brow tail are well visualized. Three lines are drawn vertically upwards out of the points marked on the brows – on the right and on the left side correspondingly. Two horizontal lines are drawn: one through the AP and the other on the halfway between the AP and the line connecting the brow heads. (Important: any flat image somewhat distorts the proportions of a 3-D object, so be sure to place the lower horizontal line in the middle between the AP and the brow heads in Fig. 2) The sections of the resulting net correspond to zones of different expressive activity. © 2016 Wiley Periodicals, Inc. Specific aspects of combined male face correction BTA is introduced in the center of each section (rectangle) of the dynamic topographic net. It is a handy reference benchmark for the therapist, while it allows to make injections at the same level, to distribute the toxin dose systematically and to exactly document the injection layout of each procedure. When injecting BTA in the forehead, the needle is introduced at an angle of 90° to the skin down to the periosteum and subsequently slightly drawn back into the frontalis muscle. There is another technique, perhaps more simple: the needle is introduced directly into the muscle at an angle of 45°. It is possible to make subcutaneous BTA injections to achieve a “soft” relaxative effect. The BTA doses per injection point are 2.5– 5 U (Fig. 2) depending on the degree of facial expressive activity. So, three ribbon zones of toxin introduction can be distinguished according to the presented dynamic net: level A – from the brow line to the lower horizontal line; level B – between the lower and upper horizontal lines; level C – above the aponeurosis central fixation point (this is the level where the frontalis muscle fibers transit to the aponeurosis). Level B is the main region for correcting horizontal forehead wrinkles in men, and in women as well. This zone is the highest activity area of the frontalis muscle, and the introduction of BTA does not lead to a change in brow position. On level C, BTA is also injected in all sections except the central one (we consider this level in case of a high forehead and/or low position of the aponeurosis central attachment point). BTA dose per injection point is 2.5 U. Important: in case of a low forehead or deep wrinkles with apparent tissue excess, the injections are made only on level C. The choice of injection points on level A should be more considerate. No injections are made in the zone between two medial vertical lines for prevention of brow head ptosis. In men, BTA may be injected in the paracentral rectangles, 2–2.5 U per injection point. The injections are made more superficially. Working on this level allows to retain the horizontal outline and low positioning of the brows in men. Formation of the interbrow area wrinkles and creases is secondary to hypertonus/hyperactivity of the corrugator, procerus, and the brow-lowering muscle. A partial relaxation of the corrugator and the browlowering muscle should be achieved to make vertical wrinkles less distinct. Here, a standard BTA dose for the glabella zone correction of 20–40 U is used. The first injection point corresponds to the corrugator head (bone fixation zone), the projection of which is the © 2016 Wiley Periodicals, Inc. . M-A Scherer point of maximum brow head motility while frowning. The injection is deep, intramuscular, the BTA dose is 7.5–15 U into each point on the right and on the left side, and in case of injections in young patients, the dosage may be reduced to 5 U. The use of mentioned toxin dosages allows to maintain full facial expressiveness in the interbrow area. For men, this is essential. When correcting horizontal wrinkles in the interbrow area, BTA is introduced into the procerus muscle, in the point situated in the middle of the vertical (centrofacial) segment between two horizontal lines drawn from one brow head to the other and – with eyes looking straightforward – from one pupil center to the other. The muscle location and activity can be defined more exactly through facial expressiveness tests (the patient is asked to wrinkle the nose and frown). The injections are intramuscular, 3–4 mm deep; the BTA dose is 10–15 U. Correction of the brow position The goals set in correction of brow position and outline in men and women differ drastically. When working with a female face, the attention is focused on formation of a brow curvature or on lifting of the brow lateral part – if not the entire brow. In male face correction, it is more often necessary to preserve the brow position and less often to lift the brows evenly provided that their linear horizontal outline (a genderspecific feature) is maintained. Nevertheless, I hear a request “to open the eyes” by slightly lifting the brow rather frequently; it comes more often from young and middle-aged patients who usually work in places with a mixed personnel. In older patients, such a correction is performed in case of a somewhat overhanging upper eyelid. Botulinum therapy The injection layout is elaborated with the use of the dynamic net and the points located in the brow area (Fig. 2). As a rule, in women, BTA is introduced on brow level into projection points of the upper orbital part of the orbicular muscle of the eye. A brow curvature is formed and the brow tail levation takes place due to relaxation of this muscle and prevalence of the levator activity of the lateral part of the frontalis muscle. In men, BTA is introduced directly into the brow, into the upper orbital part of the orbicular muscle of the eye as well (Fig. 3). An additional point is used for injections, and it is located in the middle of a segment 569 Specific aspects of combined male face correction . M-A Scherer Figure 3 The botulinum toxin type A injection layout for correction of an excessively low brow position (brow lift). between the point of maximal brow head motility and the point of brow curvature corresponding to the brow-lowering muscle projection. BTA introduction into 4 points in the brow area allows to relax the corrugator, the brow-lowering muscle, and the upper orbital part of the orbicular muscle of the eye. Due to even traction of the frontalis muscle, the brow is slightly lifted without change of the linear shape, that is, preserving the gender-specific feature. A BTA dose of 2.5–5 U is introduced into the brow tail point, 2.5– 5 U – into the relative brow curvature point, 2.5–5 U into the intermediate point, and a dose of 5 U into the point of the brow head (this point is also used in correction of interbrow area wrinkles in Fig. 2). For enhancement of the levator function of the lower part of the frontalis muscle, BTA is introduced into points located symmetrically in the upper depressor part of it on level C on the left and on the right (two points on each side), 2.5 U per point (Fig. 3). In this case, the compensatory muscle activity mechanism comes into action.2,4 Volumetric plasty for brow lifting Correction of the brow position can be performed with fillers in patients with a low-active frontalis muscle and faintly accentuated superciliary arches. Therefore, BTA injections are made into the discussed above 4 points on the brow and into the procerus muscle, and after 2 weeks, the filler is injected. A slight levation of the brows is achieved, and motility in the forehead is maintained. This method is simple enough. The cross-linked stabilized HA preparation is introduced through a 25G cannula 50 mm long. The cannula entry point is 570 Figure 4 Brow lifting with volumetric filler injections. situated a bit laterally from the extreme point of the brow tail. The cannula is introduced down to the periosteum and is moved medially upward toward the frontal protuberances, and 0.3–0.5 mL of filler is introduced in each of their projection points (Fig. 4). Consequently, an active upward modeling of the preparation is being performed. Creation of a certain convexity of the frontalis muscle leads to a brow line rise by several millimeters. Correction of the temporal area Volumetric plasty Depression of the temporal area soft tissues is an esthetic defect as such and can cause lowering of the brow tail. Adipose tissue atrophy of the temporal area often comes along with an involution of the adipose tissue in the brow area (retroorbicularis oculi fat, ROOF). That is the reason why temporal area volumetric plasty encompasses, as a rule, correction of the lateral brow end area as well (Fig. 5). In correction of the temporal area, it is necessary to avoid injury to the superficially located vessels and nerves.5 The interfascial layers are considered in this context to be the most safe filler injection level.6 The technical procedure that I suggest allows to inject the filler exactly into this level: the soft tissues of the temporal area are grasped between two fingers and are lifted over the muscle, and the needle or cannula is introduced into the base of the formed crease. The total filler amount should not be more than 0.3–0.5 mL for one side. This preparation volume provides for a sufficient and harmonic outcome. Immediately after the injections, an active modeling is made to distribute the introduced material evenly. When performing fan-type © 2016 Wiley Periodicals, Inc. Specific aspects of combined male face correction (a) . M-A Scherer of the temporal area, and ≥0.05 mL of the preparation is injected retrogressively along every vector. Sometimes a venous pattern may appear, but this undesired effect resolves completely in 10–14 days after full integration of the preparation. Wrinkle correction in the lateral eye corner area Botulinum therapy (b) Figure 5 Volumetric correction of the temporal area: (a) the bolus technique; (b) linear injections with a cannula. Figure 6 Location of botulinum toxin type A injection points in correction of the lateral eye corner zone and elimination of compensatory medial eye corner wrinkles. injections with a cannula, the entry point is situated on the zygomatic arch, upward from the line drawn from the pupil of the eye to the ear lobe. The cannula is advanced through the temporal fossa to the border © 2016 Wiley Periodicals, Inc. In men, esthetic problems of the periorbital area form early and are significantly expressed due to the prevalence of hypertensive or hyperkinetic muscle activity type. Age-related changes of the area around eyes are undoubtedly related to a change in brow position: brows and eyes form an integrated esthetic entity. In correction of the periorbital area, it is necessary to consider skin tonus of the lower and upper eyelid, presence of expressed skin excess and edema as well. These are relative contraindications for esthetic correction. Correction of the lateral eye corner area in men is not meant to relax the muscles of this area completely. A deep relaxation of the lateral part of the orbicular muscle of the eye creates the impression of an open and trustful gaze, which befits women very well, but is out of question for men – the gender-specific “aggressiveness” is lost. The goal of esthetic correction is to smoothen the wrinkles in the central and lower parts of the lateral eye corner; nevertheless, preservation of small wrinkles in the upper part of this area is possible. Therefore, it is necessary to relax only the lower lateral part of the orbicular muscle of the eye, leaving the upper lateral part active. To do so, the injection points are located lower than the intercanthal line, and the injections are made intra- or subcutaneously. In such a correction, the skin rugosity is eliminated but single rhytids remain. So, the ability to convey positive emotions through natural, hearty facial expressions (for example, a sincere Duchenne smile7) is preserved. The injection points are selected as follows (Fig. 6): Several lines are drawn from the pupil midpoint with the patient looking straightforward – the first line to the brow tail; the second is a horizontal line drawn through pupil centers of both eyes; the third line is drawn to the ear lobe; and the fourth is drawn vertically through the pupil midpoint (the midpupil line). These lines form projection sections of the orbicular muscle of the eye with the orbicular bone edge as the inner border. A total of 5 U of BTA is introduced into the central part of each section, except the upper 571 Specific aspects of combined male face correction . M-A Scherer lateral one (hatched in Fig. 6). This technique is recommended for fan-type location of wrinkles. An adjustment is possible in every particular case. Injections in the lower eyelid area should be performed with caution: BTA introduction in high doses may lead to a prolapse of the infraorbital fat and hernia aggravation – that happens more often exactly in men and may also lead to ectropion formation. The importance of wrinkle correction in the eye inner corner area should be noted. These rhytids may be of a compensatory origin. For prevention of their development, 1–2.5 U of BTA is introduced intracutaneously into the point where the midpupil line crosses the lower orbital edge (marked with “*” in Fig. 6). The preparation is injected intradermally with papula formation to avoid eyelid eversion. The dose is reduced to 1–1.25 U if the patient earlier underwent a lower eyelid blepharoplasty. (a) (b) Correction of the zygomatic area Volumetric plasty The buccomalar area is the center of face harmony and balance. Volume of the deep (suborbicularis oculi fat, SOOF) and superficial adipose tissue layers (the intraorbital fat/malar mound/and the middle cheek fat) in the zygomatic arch area is of big importance for the esthetics of the face middle third, ensuring the malar and, partially, cheek form, curvature, and rotundity. The inferior suborbital adipose tissue (SOOF) – statically attached, nongliding, and nonmovable through motility of facial expressive muscles – does not sag with age, but is susceptible to involution; therefore, the volume recovery of this compartment is an important step of esthetic correction.8 When working with male patients, it is important, as mentioned above, to rule out hypercorrection which may cause face feminization.9 Therefore, it is regarded essentially important to use small volumes of a cross-linked stabilized HA filler. The filler is introduced with a needle in a microbolus technique: A total of 5 consecutive injections of 0.1–0.2 mL each (total volume not more than 0.5–1 mL on each side) are made on the zygomatic arch line (Fig. 7). Preparation location depth is above the periosteum. It is possible to carry out zygomatic area correction with a cannula 25G 25 mm long: Retrogressive injections are carried out in a fan technique, and the cannula access is provided in a point located on the so-called McGregor’s patch (a fibrous tissue clump in the center of the zygomatic arch). The midpupil line limits the vectors medially, and it allows to avoid injuring the neurovascular bundle emerging 572 Figure 7 Volumetric filler injections into the malar zone: (a) the microbolus technique; (b) fan technique using a cannula. from the infraorbital foramen.6 Total volume for one side is 0.5–1 mL, and for one vector 0.1–0.2 mL. A thorough modeling is carried out after injection. Conclusion The increasing number of male patients in practice of esthetic medicine specialists has become an incentive for comprehensive analysis of this trend. In the opinion of psychologists, motivation of male patients to undergo an esthetic correction comes not only from awareness of face aging, but also from a number of social aspects. For men, the necessity of rejuvenation is inseparable from accentuating gender-specific features, male sexuality, personal wealthiness, social status, role in the community. The final expectance regarding esthetic correction is to look rejuvenated, irradiating health and energy, successful, keeping up with time (Fig. 8). But it is important not only to maintain but even accentuate to some extent the masculine features of the appearance. Along with common issues, wishes of patients may differ according to age, social status, occupation, and professional environment. Some men © 2016 Wiley Periodicals, Inc. Specific aspects of combined male face correction (a) (b) (e) (h) (c) (f) . M-A Scherer (d) (g) (i) (j) Figure 8 Metamorphosis of male patients at various stages of esthetic correction. Patient L., age 36: (a) presented with complaints about wrinkles in the forehead and a tired, haggard look. A combined correction was carried out. In the first step, 75 U botulinum toxin type A was introduced in the upper face third and the lateral orbit area. In 2 weeks, volumetric correction of the malar area and the nasolabial folds (cross-linked stabilized hyaluronic acid, 2 mL) was performed. (b) The outcome. (c) and (d) correction layout. Patient D., age 30: (e) presented with complaints about a tired look, also looking older than his age. Botulinum therapy (in the interbrow area) and volumetric correction with 3 mL of cross-linked stabilized hyaluronic acid preparation were carried out. (f) The correction outcome. (g) correction layout. Patient A., age 32: (h) presented with complaints about a “tired face”. Botulinum therapy (in the interbrow area) and multizone volumetric correction with 3 mL of cross-linked stabilized hyaluronic acid preparation were carried out. (i) The correction layout. (j) The outcome. are proud of their “scowl”, and some, to the contrary, come with a request to lift the brows a little and “open” the eyes. Whatever procedure is carried out, the key point for success will be moderateness of the outcome. An outside observer must notice no particular changes, only improvement of the appearance as a whole, a harmonization of the face. In botulinum therapy, universal injection algorithms should not always be the only reference. The specific features of male skin, muscles, and facial bones require a special approach to esthetic drawbacks correction. The continuous changes of face esthetics perception in the society transform the correction goals as well. My accumulated clinic experience shows that in botulinum © 2016 Wiley Periodicals, Inc. therapy of the upper and middle third of male faces, it is appropriate to use the same BTA dosages as recommended for women – without increasing them by 50 or even 100%. The therapy specifics concern the injection points location and toxin doses for every point. As a result, a rather distinct smoothening of the skin profile without detriment to the facial expressiveness and gender-specific features is achieved. To my opinion, optimal results of volumetric filler injection procedures are achieved with the use of – however paradoxical it may seem – fairly “delicate” fillers, which create a discreet volume, nevertheless with a possibility of modeling in the tissues. Although a slight volumetric hypercorrection of the middle face 573 Specific aspects of combined male face correction . M-A Scherer third is acceptable in females (an extra rotundity and tenderness of the face), in males it may deprive the appearance of a masculine air. Men perceive such things as extremely negative (a “doll-like” face). Use of a cross-linked stabilized HA preparation allows to carry out volumetric correction in men with a maximally natural-looking and stable outcome. Acknowledgements The author is thankful to Dr. Razumovskaya E.A. for consulting and kind help with preparation of this article. Conflict of interest The author reports no conflicts of interest regarding this article. References 1 Naini FB. Facial Aesthetics: Concepts and Clinical Diagnosis. Chichester, UK: Wiley-Blackwell Pub; 2011: pp. 3–16, 45-52. 2 Michaud T, Gassia V, Belhaouari L. Facial dynamics and emotional expressions in facial aging treatments. J Cosmet Dermatol 2015; 14: 9–21. 574 3 Pessa JE, Rohrich RJ. Facial Topography. (Clinical Anatomy of the Face). St. Louis, Missouri; Quality Medical Pub., Inc.; 2012: p. 62. 4 Sattler G, Kane M. Illustrated Guide to Aesthetic Botulinumtoxin Injections: Basics, Localization, Uses. (Aesthetic Methods for Skin Rejuvenation) Quintessence Pub. Co., 2013 5 Juh asz MLW, Marmur ES. Temporal fossa defects: techniques for injecting hyaluronic acid filler and complications after hyaluronic acid filler injection. J Cosmet Dermatol 2015; 14: 254–9. 6 Seckel BR. Facial danger zones. Avoiding nerve injury in facial plastic surgery. USA; QMP; 1994. 7 Duchenne GB (Boulogne) G-B 1867. Mecanisme de la physionomie humaine ou analyse electro-physiologique de l’expression des passions. [Mechanism of the human facial features or electrophysiological analysis of expressed emotions] Paris: Librairie J.-B. Bailliere et Fils. Can be viewed at: http://vlp.mpiwg-berlin.mpg.de/library/data/ lit38953 €sthetischen Augmenta8 Sattler G, Sommer B. Bildatlas der a tionsverfahren mit Fillern: Dosierung, Lokalization, Anwen€ dung. (Asthetische Verfahren zur Hautverj€ ungung, Band 2) KVM – Der Medizinverlag, 2010 9 Swift A. The mathematics of facial beauty: a cheek enhancement guide for the aesthetic injector. In: D Jones, ed. Injectable Fillers: Principles and Practice. Chichester, UK: Wiley-Blackwell Pub. Ltd.; 2010: pp. 140–57. © 2016 Wiley Periodicals, Inc.