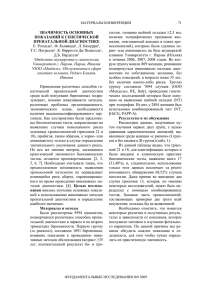
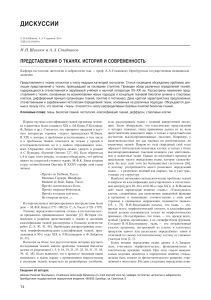
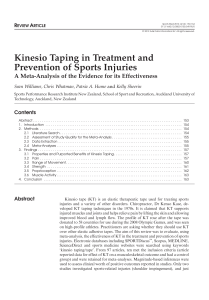
Cervical Cancer Module Coordinator: Dr Valerie Hinch v.hinch@ulster.ac.uk Cervical Cancer and HPV Aims and Learning Outcomes: after studying this session you should confidently be able to: 1. 2. 3. 4. Understand the normal cytology of the cervix Outline stages of cytology abnormality - Dyskaryosis Outline stages of Histology abnormality - Cervical Intraepithelial Neoplasia (CIN) Describe the role of Human Papilloma Virus in cervical cancer Glossary Abnormal: A change in the appearance of epithelial cells (dysplasia) or the appearance of the nucleus (dyskaryosis) Benign: A tumour that is not cancer. It does not spread to other parts of the body but sometimes it is removed anyway if it grows too big. Not malignant. Biopsy: Procedure carried out to extract a sample of tissue so it can be examined. Borderline: This means that cell changes have been found in the cells from the cervix but they will most likely go back to normal on their own. Brush (LBC): Broom like device used to collect cells from the cervix when taking a Liquid Based Cytology sample. Call/Recall: The process used to invite people for a screening test Cervical cancer/carcinoma: Cancer of the neck (cervix) of the uterus. The tumour has spread into surrounding tissue and may involve adjacent organs (invasion). It may be detected in a precancerous stage of development by a cervical screening test. Cervical Intraepithelial Neoplasia (CIN): Cellular changes in the cervix (neck of the womb) preceding the invasive stages of cervical cancer. The CIN grading system distinguishes three stages, CIN1, CIN2 and CIN3. The three grades of CIN relate to the thickness of the tissue covering the cervix that is affected. CIN 1 means one third of the thickness of the tissue covering the cervix has abnormal cells. CIN 3 means the full thickness of the tissue covering the cervix has abnormal cells. All these results mean that they are pre-cancerous. Cervix: Neck of the Uterus (Womb) Colposcopist: Clinician of gynaecological medicine specialising in the use of a colposcope and treatment. Cytology/Cytopathology: The study of cells under a microscope. Dyskaryosis: The appearance of abnormal cells whose nuclei show the features characteristic of the earliest stage of malignancy. Mild Dyskaryosis Indicates mild or slight cell changes in the cervix Moderate Dyskaryosis Indicates moderate cell changes in the cervix Severe Dyskaryosis Indicates severe cell changes in the cervix Fail Safe System: Procedures built into the computer system to ensure any woman with a not normal result is followed up. Human Papilloma Virus: There are over 100 different types of this virus and they cause different epithelial conditions e.g. HPV 1,2, + 4 cause hand and feet warts; HPV 6 + 11 cause genital warts and HPV 16 +18 cause CIN, indicated as major risk factor for developing cervical cancer. Inadequate screening test : A cervical screening test which cannot be properly assessed microscopically due to poor quality or too few cells/materials This could result in a repeat test. (An inadequate test is also known as an ‘unsatisfactory’ test). Invasive cancer: Cancer that has spread from its site of origin. Liquid Based Cytology (LBC) : A technique for taking and preparing slides to be read. A brush is used to gather up the cells and instead of smearing the cervical cell sample over the slide, it is placed in a preservative liquid for transportation to a laboratory. Negative (Normal): A smear result where all cells viewed were normal – no changes in structure of cells or nucleus were observed. Referral : The process whereby a patient is transferred from one professional to another, usually for specialist advice and/or treatment. Repeat smear: Usually taken three-six months after a positive or abnormal result to check if cells have fixed themselves or are still not normal Referral : The process whereby a patient is transferred from one professional to another, usually for specialist advice and/or treatment. Repeat smear: Usually taken three-six months after a positive or abnormal result to check if cells have fixed themselves or are still not normal Definition • Cytology (from the Greek word ‘kytos’ means ‘hollow’: Scientific study of the structure and function of cells Non-gynaecology (non cervical) - discuss in next week’s lecture Gynaecology (cervical cytology) • Cytopathology: A branch of laboratory medicine concerned with examination of cells in health and disease • Cytopathologist: Clinician whom analysing and diagnoses cytology cells • Cervical Cytology: Study of cervical cells Histology vs Cytology • Both valuable diagnostic tools. • Important to take full advantage of the additional techniques that can be applied to cytology smears and histopathology tissue sections to gain maximum clinical information. • Histology diagnosis may be required for confirmation of Cytology diagnosis. Histology Cytology Invasive Minimally-invasive Tissues Cells Formalin fixation Wet/dry fixation Paraffin embedded blocks Slide smear preparation Overnight processing Same day processing Diagnosis by Pathologist Diagnosis by BMS Costly Minimum cost The Female Genital Tract Surrounding lymph nodes Transformation zone – also known as the squamous/ columnar junction • Here you have a schematic diagram of normal female genital tract illustrating the transformation zone (squamous/columnar junction) – note the surrounding lymph nodes and the Histology representation Squamous Columnar cells cells Let’s take a journey of a gynaecology (cervical sample) through the laboratory,…..it all begins with cervical screening,.. Why Cervical Screening? Why Cervical Screening? - To prevent cervical cancer • • • • • • Approximately 3,200 new cervical cancer cases in the UK every year (>8 every day). Cervical cancer is the 14th most common cancer Cervical cancer accounts for 2% of all new cancer cases in females in the UK Cervical cancer accounts for less than 1% of all new cancer cases in females and males combined in the UK Incidence rates for cervical cancer in the UK are highest in females aged 30 to 34 (2015-2017). Since the early 1990s, cervical cancer incidence rates have decreased by a quarter (25%) in the UK (2015-2017). (UK, as at 2017) ,…mortality rates (UK 2016-2018) • Approximately 850 cervical cancer deaths in the UK every year, (> 2 every day) • The 19th most common cause of cancer deaths, with approximately 860 deaths in 2018. • Accounts for 1% of all cancer deaths in females in the UK (2018). • Mortality rates are highest in females aged 90+ (2016-2018). • Each year more than a quarter of all cervical cancer deaths (29%) are aged 75 and over (2016-2018). • Since the early 1970s, mortality rates have decreased by three-quarters (75%) • Over the last decade, mortality rates have decreased by around a sixth (18%) 2020 - Number of NEW CANCER CASES • • • • Two main forms of cervical cancer: Squamous Cell Carcinoma ~ 85% Glandular Cell Carcinoma - Adenocarcinoma ~10-15% A study by the International Agency for Research on Cancer has reported an increase in adenocarcinoma and a downward trend in Squamous Cell Carcinoma in many countries worldwide • Note the % in comparison to various types of cancers • Perhaps the screening programme is contributing to the small % of cervical cancers? How does a cervical cell become cancerous? Characteristics common to many cancers: 1. Abnormal signal transduction resulting in uncontrolled cell proliferation 2. Loss of apoptosis (programmed cell death) 3. Tissue invasion and Metastasis, allowing spread of the cancer 4. Angiogenesis, leading to enhanced blood supply of tumour Cancer progression • Most cancers arise as in cervical cells in the epithelial cells (these are the cells that arise on the surface of tissues and organs), • When they begin to proliferate and become out of control, they are said to become hyperplastic and hyperplasia occurs. Symptoms and Risk Factors associated with cervical cancer • • • Cervical cancer characteristically has a long pre-cancerous phase, the changes take place primarily in the transformation zone Symptoms: Abnormal vaginal bleeding Post coital bleeding Vaginal discharge Risk Factors: Early age of intercourse Smoking Number of sexual partners HPV Cervical Screening • • • • • • • • Screening is NOT a test for cancer. It is a national recommendation and local policy that females under 25 are not routinely invited for cervical screening It is however recommended that all females aged between 25 and 64 years, who have ever been sexually active, have regular screening tests Females aged 25-49 are invited every three years Females aged 50-64 are invited every five years England, Wales and Scotland use HPV primary screening Northern Ireland use cell morphology screening following by HPV detection if required. Screening aims to prevent cervical cancer by detecting early pre-cancerous changes in the cells that line the cervix (squamous/columnar) Test results show abnormal changes in approximately 1 in 10 females Any abnormal changes can then be treated, preventing them from potentially developing into cancer Where does the screening take place? • • • • • • All females who fall within the screening age range are automatically invited to attend for a screening test. Screening is carried out by a trained clinician Samples are sourced from: GPs Health centres Hospital Outpatient’s Department Sexual and reproductive health (family planning) clinic. Cervical cells are sampled A small soft brush is used to gently pick up a sample of cells from your cervix. The sample is rinsed in an alcohol based preservative - ThinPrep Vials e.g. Hologic Ltd (21ml PreservCyt) How are the cervical cells sampled? • Cervical cells are scraped from the squamocolumnar junction (transformation zone) and screened for abnormality Sample rinsed in alcohol-based preservative and sent to laboratory How are the samples processed by the clinician? 1 3 5 RECORD the patient's full name and date of birth on the vial. ... the patient information and medical history on the cytology requisition form. RINSE the Cervix Brush immediately into the PreservCyt Solution vial PLACE the vial and requisition in a specimen bag for transportation to the laboratory. 2 4 OBTAIN an adequate sample from the cervix using a Cervix Brush (broom-like device) TIGHTEN What happens at Cervical Screening: Videohttps://vimeo.com/113916053 Laboratory checks To ensure samples are suitable for processing Laboratory checks are important - important quality control: • • • • • • Samples must be accompanied by a request form No cervix brush should have been left in vial The vial cap should not be over tightened Fluid levels should be sufficient If sample is grossly blood-stained need to treat with Glacial Acetic Acid (GAA), otherwise cell morphology will be masked Expiry date of vial should be checked - If the vial is “Out of Date”, this should be recorded on laboratory error logging system, senior BMS informed, returned to sender Samples with any of the following details should be drawn to the attention of a senior BMS Urgent Private patients Post-menopausal bleeding Details of any ongoing therapy e.g. HRT Molecular Investigations Suspicious Request form checks: Patient and source information must be clearly printed on the request form Cervical specimen requests received without essential criteria may be returned to the sender for amendment Full Name Example of essential information recorded for Date of Birth each patient Gender Patient’s address Health & Care Number Relevant Clinical history Patient’s Location Patient’s Consultant/GP So how is testing performed? • • • • • Thin Prep T5000 Processor (an example) Fully automated instrument for the preparation of liquid-based cytology samples Under negative pressure the sample collects cells which are then transferred on to a glass microscope slide The instrument must be kept clean and free from glass particles and dust Auto-Loader section allows a batch of up to 160 samples to be processed Sample workflow Processors PAP stained smear Thin-Prep vials Sample workflow Imaging system How could we represent cervical cells in a practical? Swab our buccal cavity. Just like cervical cells, the cells which line the inside of your cheeks are flat sheets of squamous epithelial cells Immature non-keratinized (i.e. they still contain their nuclei unlike mature keratinized cells) Histology view Squamous cells Columnar cells Why use PAP stain? Easy to visualise colours from the entire spectrum: red, orange, yellow, green, blue, and violet (multichromatic) Superficial cells are orange to pink Intermediate and parabasal cells are turquoise green/blue Staining results in transparent cells Cell nuclei are crisp blue to black Chromatin patterns are visible Histology view Cytology view Papanicolaou (PAP) stain • • • • • • • • • Automated Papanicolaou (PAP) stain Multichromatic staining histological technique developed by George Papanikolaou (father of cytopathology) Most employed for gynaecological specimens Also employed for some non-gynaecological specimens This procedure is considered accurate if the prepared, stained specimen displays a representative subset of the cellularity present The differential staining pattern permits prolonged periods of microscopy with minimal eye-strain The detection of pre-/malignant cells is based upon visual observation, and does not yield quantitative information When presenting its composition several dyes, it can reveal different types of cells. These characteristics are what make it optimal for cytological type studies. Papanicolaou (PAP) stain continued,… • • • • • • • A nuclear stain, haematoxylin, is used to stain cell nuclei OG-6 counterstain stains keratin EA (Eosin Azure) counterstain, (Eosin Y ) stains the superficial epithelial squamous cells, nucleoli, cilia, and red blood cells Light Green SF yellowish stains the cytoplasm of other cells, including non-keratinized squamous cells The stained specimen should display hues from the entire spectrum: red, orange, yellow, green, blue, and violet The chromatin patterns are well visible, the cells from borderline lesions are easier to interpret. The staining results in transparent cells, so even thicker specimens with overlapping cells can be interpreted On a well prepared specimen, the cell nuclei are crisp blue to black Cells with high content of keratin are yellow. Superficial cells are orange to pink, and intermediate and parabasal cells are turquoise green to blue. Metaplastic cells often stain both green and pink at once Results of PAP stain Dye Structure Colour Haematoxylin Nucleus Blue/Black Light Green (Eosin A50) Immature (Non-keratinized. intermediate, parabasal, basal, columnar cells Blue/Green Eosin Y (Eosin A50) Cytoplasm of superficial cells Red/Pink/Orange Orange G Mature (keratinized), superficial cells Orange A stained PAP smears would then be ready for the Consultant Pathologist/BMS to screen and diagnose,…. Cytology microscopy Microscopy Clinicians: Primary screening All BMS have a daily workload of slides to screen, ‘spotting’ any areas of concern Rapid Review All negative and inadequate smears are reviewed Checking Staff fully re-screen all cases referred commenting on the quality of the sample and spotting areas Final medical screening Consultant Pathologist produces final report Cytology results Results may be as follows: Infections: Fungal hyphae Trichomonas Actinomyces Herpes virus Human Papilloma Virus (HPV) Precancerous changes: Negative Borderline changes Mild dyskaryosis (low grade) Moderate dyskaryosis (high grade) Severe dyskaryosis (high grade) Invasive (high grade) Glandular neoplasia Infections Candida Albicans Approximately 20% of women normally have Candida in the vagina without having any symptoms. PAP show hyphae and spores. Trichomonas Sexually transmitted infection (STI) caused by Trichomonas vaginalis (TV).. Cervix becomes very inflamed with sores. PAP show small perinuclear halo nuclei Actinomyces Seen in the vast majority of patients, usually seen in patients using an IUCD (including the Mirena coil). PAP show tangled clump clusters of organisms Herpes Genital herpes increases the risk of cervical cancer . It causes sores or blisters to form in or around the genitals/ HPV Infection – main cause of cancer (this will be discussed later) • White area indicates infection • PAP illustrates nuclear enlargement, multinucleation, anisocytosis, perinuclear cytoplasmic vacuolization • Koilocyte is a squamous epithelial cell occur as a result of HPV Koilocyte Cytology Morphology Normal Morphology • • Normal cells are characterised by their morphological uniformity Nuclear size is proportional to the relative cytopasmic area (cytonuclear index) Nucleus (N) Cytoplasm (C) N:C ratio Cell size & shape Nuclear morphology - reflects the state of proliferation, round or ovoid in shape, smooth nuclear contour, evenly distributed, finely granular homogeneous chromatin Cytoplasm - generally provides an indication of origin, functional state & degree of differentiation Small compact nucleus Occupying less than 1/3 of cell Low N/C ratio Abnormal cells • • • • An abnormal cervical screening test result means that you have changes in the cells covering the neck of your womb (cervix). These changes are not cancer. The cells often return to normal by themselves, however if not treated, these changes could develop into cancer in the future. Depends on characteristics of nucleus and cytoplasm Screening result may report as being: low grade (borderline cell changes) low grade (mild cell changes) CIN1- Histology term high grade (moderate cell changes) CIN2 - Histology term high grade (severe cell changes) CIN3 - Histology term Abnormal nuclear morphology Nucleus: Increase in N/C ratio Variation in cell size, shape and staining (anisokaryosisor anisonucleosis Intense nuclear staining (Hyperchromasia) Change in chromatin pattern Irregular, coarse chromatin clumping Condensation of chromatin at nuclear border Angularity of nuclear border Irregular nuclear outline with grooving, indentation or crenation Thickened nuclear envelope –karyotheca Increased nuclear DNA content Abnormal nucleoli morphology Nucleoli: Normal nuclei contain small, discrete nucleoli composed of RNA and associated proteins Both multinucleolation & macronucleolation observed in proliferative states-both neoplastic& non-neoplastic Degenerative chromatin may appear as: A dense, contacted mass Dense fragments Undergo dissolution Abnormal cytoplasm morphology Cytoplasm: Variation in size & shape of similar cells –Anisocytosis Abnormal cells may have: Larger nuclear volume, thus Smaller cytoplasmic volume Nuclear : Cytoplasmic ratio affected Ultrastructural composition of the cytoplasm exerts a major influence on staining reactions Mitochondria, golgi bodies, lipids, carbohydrates & hormones etc Cytology has the following stages of abnormality: Cytology terms Pre-cancerous changes are described as Dyskaryosis Borderline, Mild, Moderate, Severe Dyskaryosis (Dysplasia) Histology terms Cervical Intraepithelial Neoplasia (CIN) The changes are divided into 3 phases: CIN1, CIN2, CIN3 Mild Dyskaryosis Mild Dyskaryosis Normal cells • • Dyskarytotic nucleus in a differentiated cell Less than 1/2 the cell in the nucleus Squamous cells Basement membrane CIN1 Moderate Dyskaryosis Moderate Dyskaryosis Normal cells • • Less differentiation of cytoplasm Dyskaryotic Nucleus occupies 1/2 - 1/3 cell Squamous cells Basement membrane CIN2 Severe Dyskaryosis Severe Dyskaryosis Normal cells • Dyskaryotic nucleus occupies 3/3 of the cell Normal Squamous cells Basement membrane CIN3 Nuclear abnormality with Koilocytosis Nuclear abnormalities due to HPV infection Nucleus-irregularly enlarged Nuclear hyperchromatic Nuclear multinucleation Cells perinuclear halo Perinuclear halo Condensation of cytoplasm Multinucleation Condensation of cytoplasm Summary of Cervical Intraepithelial Neoplasia (CIN) Summary Histology: Normal to CIN3 Squamous cells Basement membrane Normal CIN 1 CIN 2 CIN 3 Treatment - abnormal cells • LLETZ - (large loop excision of the transformation zone). It’s also known as loop electrosurgical excision (LEEP) or loop diathermy. This is the most common treatment for abnormal cervical cells. The colposcopist uses a thin wire loop to remove the transformation zone of the cervix. The wire has an electrical current running through it, which cuts the tissue and seals the wound at the same time. • Cone - biopsy where a cone shaped wedge of tissue from the cervix is removed. • Cold coagulation - this uses a hot probe to burn away abnormal cells. • Cryotherapy - The colposcopist uses a cold probe to freeze away the abnormal cells. • Laser ablation - A laser beam is a very strong, hot beam of light. It burns away the abnormal area. If cancer arises Summary: Normal - Invasive carcinoma Cervical Squamous Carcinoma Normal Cervix Cervical Squamous Carcinoma Invasive carcinoma Nucleoli irregular in shape and size, vary in number Irregular clearing in chromatin (windowing) Cytoplasmic keratinisation Cancer Stages Cervical Cancer - Stage 1 Stage 1A1 means the cancer has grown less than 3 mm into the tissues of the cervix. Stage 1A2 means the cancer has grown between 3 and 5 mm into the cervical tissues. Stage 1B2 the cancer is at least 2cm but not bigger than 4cm in size. Stage 1B1 the cancer is deeper than 5mm but no more than 2cm in size. Stage 1B3 the cancer is at least 4cm but is still only in the cervix. Cervical Cancer - Stage 2 Stage 2A1 means the cancer is 4 cm or less. Stage 2A2 means the cancer is more than 4 cm. Stage 2B the cancer has spread up into the tissues around the cervix. Cervical Cancer - Stage 3 Stage 3A is when the cancer has spread to the lower third of the vagina but not the pelvic wall. Stage 3B means the tumour has grown Stage 3C1 means cancer is in the through to the pelvic wall or is blocking nearby pelvic lymph nodes. Stage 3C2 means cancer is in the para-aortic lymph 1 or both of the tubes that drain the nodes (in the abdomen). kidneys (the ureters). Cervical Cancer - Stage 4 Stage 4A is when the cancer has spread to nearby organs such as the bladder or back passage (rectum). Stage 4B is when the cancer has spread to organs further away, such as the lungs. Your doctor might call this secondary or metastatic cancer. Cervical Cancer Treatment • The stage of cancer helps the clinician decide which treatment is required. • Treatment depends on the type of cancer (the primary source) • Where the cancer is located • Other health conditions • Surgery • Combined chemotherapy and radiotherapy (chemoradiotherapy) Cervical Cancer survival rates Survival statistics for people diagnosed between 2013 and 2017. These statistics are non-age-standardized. Stage 1 Around 95 out of 100 people (around 95%) will survive their cancer for 5 years or more after diagnosis. Stage 2 Almost 70 out of 100 people (almost 70%) will survive their cancer for 5 years or more after diagnosis. Stage 3 More than 40 out of 100 people (more than 40%) will survive their cancer for 5 years or more after diagnosis. Stage 4 Around 15 out of 100 people (around 15%) will survive their cancer for 5 years or more after being diagnosed. Human Papilloma Virus (HPV) and Cervical Cancer HPV In humans viruses contribute to ~ 15% of all malignancies Viruses are the second most important risk factor for developing cancer in humans after cigarette smoking! 80% of viruses-associated cancers include Carcinoma of the cervix Since the advent of recombinant DNA technology and the cloning of human papillomaviruses (HPV), the association between HPV, CIN and cancer has been confirmed Compelling evidence both epidemiological and molecular tests demonstrate that persistent HPV infection is a pivotal step in the development of cervical cancer HPV Small DNA viruses 55nm in diameter A non-enveloped icosahedral outer coat Surrounding a circular genome of double stranded DNA The genome of ~ 8000bp Divided into Early genes: E1, E2, E4, E5, E6 & E7 Late genes: L1 & L2 Over 30 HPV types infect the cervical mucosa HPV genes Early genes are responsible for: DNA replication Transcriptional regulation and transformation The early gene products E6 and E7 encode the major transforming proteins: Capable of inducing cell proliferation and immortalisation By binding to the tumour-suppressor gene products p53 & pRB P16-associated with cervical cancer (IHC) Late genes control: Formation of the capsid coat HPV Infection Initiated when the virus gains access to the basal epithelial cells Stages include: infection of metaplastic epithelium at the cervical transformation zone viral persistence progression of persistently infected epithelium to cervical precancer invasion through the basement membrane of the epithelium Minor trauma (during sexual intercourse) allows access to the target cells: Near or at the cervical transformation zone The viral life cycle is linked to keratinocyte differentiation Viral replication leads to: Koilocytosis (indication of HPV), nuclear enlargement, multinucleation, dyskaryosis and CIN HPV sub-types Approximately 200 types of HPV are acknowledged to exist 15 are classified as high-risk types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73, and 82 3 as probable high-risk: 26, 53, and 66 12 as low-risk: 6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81, and CP6108 HPV 16 and 18 associated with 70% cases of cervical cancer HPV 6 and 11 associated with 90% of benign lesions such as genital warts Together with type 31, they are the prime risk factors for cervical cancer HPV Mode of Transmission Detection of HPV Morphological Electron Microscopy Immunohistochemistry (p16, Ki-67, P53) In Situ Hybridisation (ISH) Non-Morphological PCR Hybrid Capture Popular Testing Methods 1. Roche: Cobas 4800 (most popular) 2. Hologic Aptima 3. Abbott Real-Time Detection HPV16, HPV18 and 12 ‘other HR-HPV’ genotypes but doesn’t have the specificity to provide their genotypes. -70% of cervical cancers are due to HPV 16 & 18 HPV16, HPV18 & HPV 45 (3rd most common HPV genotype) -12% of cervical adenocarcinomas caused by HPV45 thus this method of testing could help to identify more women at risk of cervical cancer 14 HR-HPV genotypes including HPV 16 & 18 Similar to Roche: Cobas 4800, HPV 16 and HPV 18 are specifically identified HPV Vaccines What are HPV vaccines? Vaccines which produce antibodies to protect against infection with HPV Three vaccines approved by the Food and Drug Administration (FDA) Gardasil, Gardasil 9 and Cervarix All three prevent infection with HPV 16 and 18 Gardasil also prevents infection with HPV 6 and 11 Gardasil 9 prevents infection with HPV 16, 18, 6, 11 plus 31,33,45,52 and 58 Administered to children aged 11-12 years old in two doses six months after the other Trials have proved that these vaccines have found to provide almost 100% protection against HPV16 and 18 associated HPV infections Vaccine - with/without Abnormal cervical result - what next? Borderline change (low-grade dyskaryosis) Laboratory will perform a reflex high-risk human papillomavirus (HR-HPV) test on the cytology sample If the HPV test is positive the female will be referred for colposcopy for an appointment within 6 weeks If HPV test is negative, the female will be returned to routine screening (3 years) High-grade dyskaryosis (moderate or severe) referral to colposcopy for an appointment within 2 weeks Suspected invasive cancer or glandular neoplasia referred to colposcopy for an appointment within 2 weeks Cervical Screening Programme HPV triage and test of cure protocol It has to be noted that HPV causes more than cervical cancer,….. You should now be able to: 1. 2. 3. 4. 5. Understand the normal cytology of the cervix Outline stages of Dyskaryosis Outline stages of Cervical Intraepithelial Neoplasia (CIN) Describe the role of Human Papilloma Virus in cervical cancer Be aware of the various types of treatment. End of Lecture Thank you for listening - any questions?