VetBooks.ir
VetBooks.ir
VetBooks.ir
Advances In
The Canine
Cranial Cruciate
Ligament
VetBooks.ir
VetBooks.ir
Advances In
The Canine
Cranial Cruciate
Ligament
Second Edition
Edited by
Peter Muir BVSc, MVetClinStud, PhD, Diplomate ACVS, ECVS
VetBooks.ir
This edition first published 2018
© 2018 ACVS Foundation
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
Edition History
1st Edition © 2010 ACVS Foundation; 2nd Edition © 2018 ACVS Foundation
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or
by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by law. Advice on how to
obtain permission to reuse material from this title is available at http://www.wiley.com/go/permissions.
The right of Peter Muir to be identified as the author of the editorial material in this work has been asserted in accordance
with law.
Registered Office
John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030, USA
Editorial Office
111 River Street, Hoboken, NJ 07030, USA
For details of our global editorial offices, customer services, and more information about Wiley products visit us at
www.wiley.com.
Wiley also publishes its books in a variety of electronic formats and by print-on-demand. Some content that appears in
standard print versions of this book may not be available in other formats.
Limit of Liability/Disclaimer of Warranty
The contents of this work are intended to further general scientific research, understanding, and discussion only and are not
intended and should not be relied upon as recommending or promoting scientific method, diagnosis, or treatment by
physicians for any particular patient. In view of ongoing research, equipment modifications, changes in governmental
regulations, and the constant flow of information relating to the use of medicines, equipment, and devices, the reader is
urged to review and evaluate the information provided in the package insert or instructions for each medicine, equipment, or
device for, among other things, any changes in the instructions or indication of usage and for added warnings and
precautions. While the publisher and authors have used their best efforts in preparing this work, they make no
representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically
disclaim all warranties, including without limitation any implied warranties of merchantability or fitness for a particular
purpose. No warranty may be created or extended by sales representatives, written sales materials or promotional statements
for this work. The fact that an organization, website, or product is referred to in this work as a citation and/or potential
source of further information does not mean that the publisher and authors endorse the information or services the
organization, website, or product may provide or recommendations it may make. This work is sold with the understanding
that the publisher is not engaged in rendering professional services. The advice and strategies contained herein may not be
suitable for your situation. You should consult with a specialist where appropriate. Further, readers should be aware that
websites listed in this work may have changed or disappeared between when this work was written and when it is read.
Neither the publisher nor authors shall be liable for any loss of profit or any other commercial damages, including but not
limited to special, incidental, consequential, or other damages.
Library of Congress Cataloging-in-Publication Data
Names: Muir, Peter, BVSc, editor. | American College of Veterinary Surgeons. Foundation, issuing body.
Title: Advances in the canine cranial cruciate ligament / edited by Peter Muir.
Description: Second edition. | Hoboken, NJ : Wiley ; [United States] : American College of Veterinary Surgeons
Foundation, 2018. | Includes bibliographical references and index. |
Identifiers: LCCN 2017026733 (print) | LCCN 2017027885 (ebook) | ISBN 9781119261735 (pdf) | ISBN 9781119261742
(epub) | ISBN 9781119261711 (cloth)
Subjects: | MESH: Dog Diseases–surgery | Anterior Cruciate Ligament | Dogs–injuries | Orthopaedic
Procedures–veterinary | Rupture–veterinary | Rupture, Spontaneous–veterinary
Classification: LCC SF991 (ebook) | LCC SF991 .A38 2018 (print) | NLM SF 991 | DDC 636.7/0897582059–dc23
LC record available at https://lccn.loc.gov/2017026733
Cover Design: Wiley
Cover Images: Courtesy of Peter Muir
Set in 9.5/11.5pt PalatinoStd by Aptara Inc., New Delhi, India
10 9 8 7 6 5 4 3 2 1
VetBooks.ir
Dedication
This book is dedicated to Susannah Sample, to my family, and to all of my colleagues
who have contributed effort to advancing the understanding of canine cruciate ligament rupture, and the treatment of affected dogs.
VetBooks.ir
VetBooks.ir
Contents
About the Editor
Foreword to the Second Edition
Kenneth A. Johnson
Foreword
R. Randy Basinger, ACVS Foundation
Preface
Peter Muir
xi
xiii
xvii
xix
Contributing Authors
xxi
I Structure and Function
1
Introduction
Peter Muir
1
2 Biomechanics of the Cruciate
Ligaments
Susannah J. Sample
3 Cruciate Ligament Remodeling and
Repair
Connie S. Chamberlain, Erin E.
Crowley, and Ray Vanderby Jr.
4 Meniscal Structure and Function
Antonio Pozzi and James L. Cook
39
xv
Acknowledgements
Peter Muir
1 Morphology and Function of the
Cruciate Ligaments
Hilde de Rooster and Eithne Comerford
5 Biomechanics of the Normal and
Cranial Cruciate Ligament-Deficient
Stifle
Antonio Pozzi and Stanley E. Kim
3
13
21
31
II Etiopathogenesis of Cruciate
Ligament Rupture
Introduction
Peter Muir
45
45
6 Histology of Cruciate
Ligament Rupture
Kei Hayashi
47
7 Genetics of Cruciate
Ligament Rupture
Lauren A. Baker and Peter Muir
57
8 Cruciate Ligament Matrix
Metabolism and Development
of Laxity
Eithne Comerford
9 Morphological Risk Factors for
Cruciate Ligament Rupture
Eithne Comerford
10 Role of Nitric Oxide Production and
Matrix Protease Activity in Cruciate
Ligament Degeneration
David E. Spreng and Simone Forterre
11 Role of Antibodies to Collagen
Type I and II
Hilde de Rooster and Eithne Comerford
65
73
81
89
vii
VetBooks.ir
viii
Contents
12 Synovitis Precedes Stifle Instability
Associated with Cruciate Ligament
Rupture
Jason A. Bleedorn
13 Role of Synovial Immune Responses
in Stifle Synovitis
Peter Muir
III Clinical Features
Introduction
Peter Muir
93
101
107
107
14 Epidemiology of Cruciate Ligament
Rupture
Lauren A. Baker and Peter Muir
109
15 History and Clinical Signs of
Cruciate Ligament Rupture
Peter Muir
115
16 Partial Rupture of the Cranial
Cruciate Ligament
Peter Muir
119
17 Caudal Cruciate Ligament Rupture
Peter Muir
123
18 Stress Imaging of the Stifle
Stanley E. Kim
127
19 Stifle Ultrasonography
Cristi R. Cook
135
20 Computed Tomography (CT)
of the Stifle
Ingrid Gielen and Henri van Bree
141
21 Magnetic Resonance Imaging
of the Stifle
Peter V. Scrivani
155
22 Risk Prediction of Cruciate
Ligament Rupture using Stifle
Diagnostic Imaging
Peter Muir
IV Surgical Treatment
Introduction
Peter Muir
165
169
169
23 Arthroscopy and Arthrotomy
of the Stifle
Brian S. Beale, Donald A. Hulse,
Antonio Pozzi, and Peter Muir
171
24 Joint Lavage
Peter Muir
185
25 Extracapsular Stabilization
Selena Tinga and Stanley E. Kim
189
26 Intra-Articular Repair for Cranial
Cruciate Ligament Rupture in the
Dog
Jeffery J. Biskup and Michael G.
Conzemius
201
27 Tibial Plateau Leveling Osteotomy
Susan L. Schaefer
217
28 Tibial Tuberosity Advancement
Randy J. Boudrieau
227
29 Closing Cranial Wedge Ostectomy
and Triple Tibial Osteotomy
Simon C. Roe
243
30 Treatment of Excessive Tibial
Plateau Angle
Michael P. Kowaleski
253
31 Surgical Management of Cruciate
Ligament Rupture Combined with
Patella Luxation
Anke Langenbach and Denis J.
Marcellin-Little
261
32 Biomechanics of the Cranial
Cruciate Ligament-Deficient Stifle
Treated by Tibial Osteotomies
Antonio Pozzi, Stanley E. Kim, and
Selena Tinga
271
33 Arthroscopic Follow-Up
after Surgical Stabilization
of the Stifle
Brian S. Beale and Donald A. Hulse
34 Cranial Cruciate Ligament
Debridement
David E. Spreng
279
291
VetBooks.ir
Contents
35 Surgical Treatment of Concurrent
Meniscal Injury
Samuel P. Franklin, James L. Cook, and
Antonio Pozzi
36 Meniscal Release
Antonio Pozzi and James L. Cook
37 Progression of Osteoarthritis after
Stifle Stabilization Surgery
Susannah J. Sample
38 Clinical Outcomes after Surgical
Treatment of Cruciate Ligament
Rupture
Mary Sarah Bergh and Steven C.
Budsberg
39 Success and Failure after Stifle
Stabilization Surgery
Michael G. Conzemius and Richard B.
Evans
40 Diagnosis and Management
of Orthopaedic Infection after Stifle
Surgery
Noël M.M. Moens
V Medical Management of
Cruciate Ligament Rupture
Introduction
Peter Muir
41 Medical Therapy for Stifle
Osteoarthritis
Steven C. Budsberg
295
42 Rehabilitation for Dogs with
Cruciate Ligament Rupture
Denis J. Marcellin-Little and Courtney
J. Arnoldy
ix
343
301
VI Future Directions
307
313
Introduction
Peter Muir
43 Clinical Research Design and
Patient-Oriented Outcomes
Dorothy Cimino Brown
44 Total Knee Replacement in the Dog
Matthew J. Allen, William D. Liska,
and Valentina Brioschi
317
323
331
331
333
45 Regenerative Medicine and Cranial
Cruciate Ligament Repair
Gabriel S. Perrone, Martha M. Murray,
and Patrick Vavken
353
353
355
363
371
46 Disease-Modifying Medical and
Cell-Based Therapy
Susannah J. Sample and Peter Muir
379
Index
385
VetBooks.ir
VetBooks.ir
About the Editor
Peter Muir BVSc, MVetClinStud, PhD, Diplomate ACVS, ECVS. Dr Muir obtained his veterinary degree in 1985 from Bristol University
in the United Kingdom. After working in private practice in the UK, he returned to Bristol and obtained a PhD in veterinary science
in 1990. He then moved to The University of
Sydney to undertake training in small animal
surgery, obtaining a Masters degree in 1992.
He completed his surgery training at the University of Wisconsin-Madison and became a
Diplomate of the American College of Veterinary Surgeons in 1995. After periods on faculty at the University of California, Davis and
the Royal Veterinary College, University of
London, he returned to Madison as a faculty member, where he is currently the Melita
Grunow Family Professor of Companion Animal Health. He has authored many peerreviewed publications on stifle osteoarthritis
and cruciate ligament rupture and speaks regularly at international meetings on this work.
xi
VetBooks.ir
VetBooks.ir
Foreword to the Second Edition
The popularity and success of the First Edition of this authoritative collection of work on
canine cranial cruciate ligament rupture has
been an impetus to launch a thoroughly revised
new, Second Edition. This move is easily justifiable considering the immense clinical importance of this disease in small animal clinical
practice, and also the numerous advances that
have been made in knowledge about the problem in the last few years. The appeal of this book
to the busy clinician is that all the latest developments are assembled under one umbrella in
this volume. The editor of this volume, Dr Peter
Muir, has arranged and organized the various
chapters in a coherent manner that takes the
reader from the basics of the disease pathophysiology, through the essence of diagnosis and
treatment options, to a view of the future.
As is generally the case in science, the everincreasing body of knowledge has really served
to expose the apparently growing complexity
of the problem of canine cruciate ligament rupture. To achieve the best possible outcome for
each and every dog presented with this problem, it is no longer acceptable to have just
one standard surgical treatment that we use
in every case. We must be even more meticulous in objectively assessing each patient, and
consider how we manage concurrent problems such as meniscal injury or patellar luxation. Also, advanced imaging is assuming an
increasingly useful role in detecting variability
in skeletal and articular morphology that can
require modification in surgical technique. Furthermore, the development of dynamic imaging has allowed us to learn more about motion
of the cruciate-deficient stifle during ambulation and full weight-bearing, before and after
surgery. These are very exciting developments
that we need to carefully and critically evaluate,
and embrace as appropriate.
Dr Muir and all the contributing authors are
warmly congratulated on the production of this
new edition. However, as I previously foreshadowed in my foreword to the First Edition, I do
suspect that in another few years, we will again
be ready for yet another new edition!
Kenneth A. Johnson
Sydney, Australia
xiii
VetBooks.ir
VetBooks.ir
Foreword
The American College of Veterinary Surgeons
Foundation is excited to present the Second Edition of Advances in the Canine Cranial Cruciate
Ligament in the book series entitled Advances
in Veterinary Surgery. The American College of
Veterinary Surgeons (ACVS) Foundation is an
independently charted philanthropic organization devoted to advancing the charitable, educational and scientific goals of the ACVS. Founded
in 1965, the ACVS sets the standards for the specialty of veterinary surgery. The ACVS, which
is approved by the American Veterinary Medical Association, administers the board certification process for Diplomates in veterinary
surgery and advances veterinary surgery and
education. One of the principle goals of the
ACVS Foundation is to foster the advancement
of the art and science of veterinary surgery. The
Foundation achieves these goals by: supporting
investigations in the diagnosis and treatment of
surgical diseases; increasing educational opportunities for surgeons, surgical residents and veterinary practitioners; improving the surgical
training of residents and veterinary students;
and bettering animal patients’ care, treatment,
and welfare. This collaboration with WileyBlackwell will benefit all who are interested
in veterinary surgery by presenting the latest
evidence-based information on a particular surgical topic.
Advances in the Canine Cranial Cruciate Ligament is edited by Dr Peter Muir, who is well recognized as an expert in this field. He has chosen
a group of strong contributing authors to detail
the areas of structure and function, etiopathogenesis, clinical features, surgical and medical
management, and postoperative care and rehabilitation. We are sure you will find this reference extremely valuable.
The ACVS Foundation is proud to partner
with Wiley-Blackwell in this important series,
and is honored to present this newest book in
the Advances in Veterinary Surgery series.
R. Randy Basinger
Chair, Board of Trustees
ACVS Foundation
xv
VetBooks.ir
VetBooks.ir
Preface
Although cruciate ligament rupture has been
recognized clinically in dogs for more than
50 years, research into this condition has largely
focused on the development of methods for surgical treatment of the unstable stifle, and not
the disease mechanism. Cruciate ligament rupture is one of the most common reasons that
dogs are presented to veterinarians for the treatment of lameness. It has been a long-held clinical belief that the disease mechanism for cruciate ligament rupture in dogs is similar to that
for anterior cruciate ligament rupture in human
beings. Over the past 10 years there has been
increasing recognition that second ruptures are
common in both human beings and dogs. Historically, the dog has been a common animal
model for research into the surgical treatment
of anterior cruciate ligament rupture. Transection of the cranial cruciate ligament in experimental dogs has also been a common ani-
mal model for biomedical research studies of
osteoarthritis.
During the past 15 years, an increasing body
of work investigating the disease mechanism
for cruciate ligament rupture has been published. Cruciate ligament rupture in the dog
is a complex trait, with genetic and environmental factors contributing to disease risk. This
research is challenging established views about
what causes cruciate ligament rupture and how
affected dogs should be managed clinically. My
goals for the Second Edition of this book were
to produce a text that summarizes state of the
art knowledge about cruciate ligament rupture
in the dog, including recent advances in the past
5 years, to provide a useful reference for a broad
audience, and to highlight areas for development of future work in this field.
Peter Muir
xvii
VetBooks.ir
VetBooks.ir
Acknowledgements
I would like to acknowledge the consistent support of Erica Judisch of Wiley Blackwell, and
of Dr Mark Markel, Chair of the ACVS Foundation’s Board of Trustees for the Advances in
Veterinary Surgery book series. I am extremely
grateful to all of the chapter authors who have
consistently been very committed to this project
and have made such amazing and thoughtful contributions to this book. I am also grateful to all of the organizations that have pro-
vided financial support for clinical research into
canine cruciate ligament rupture. Without these
gifts, my work and the work of many others
that is summarized in this book would not have
been possible. Lastly, I would like to thank dog
owners and breeders for their interest in and
enthusiasm for new knowledge regarding this
important orthopaedic condition.
Peter Muir
xix
VetBooks.ir
VetBooks.ir
Contributing Authors
Matthew J. Allen, Vet MB, PhD, MRCVS
Professor of Small Animal Surgery
Director, Surgical Discovery Centre
University of Cambridge
Department of Veterinary Medicine
Madingley Road
Cambridge CB3 0ES
United Kingdom
e-mail: mja1000@cam.ac.uk
Courtney J. Arnoldy, CCRP
Physical Therapist
University of Wisconsin-Madison
School of Veterinary Medicine
UW Veterinary Care Hospital
2015 Linden Drive
Madison, Wisconsin 53706
USA
e-mail: courtney.arnoldy@wisc.edu
Lauren A. Baker, DVM, MS
Post-doctoral Fellow
Comparative Orthopaedic and Genetics
Research Laboratory
University of Wisconsin-Madison
School of Veterinary Medicine
2015 Linden Drive
Madison, Wisconsin 53706
USA
e-mail: iwicki@wisc.edu
Brian S. Beale, DVM, Diplomate ACVS
Gulf Coast Veterinary Specialists
1111 West Loop South #160
Houston, TX 77027
USA
e-mail: dogscoper@aol.com
Mary Sarah Bergh, DVM, MS, Diplomate
ACVS, ACVSMR
Associate Professor, Orthopaedic Surgery
Iowa State University
College of Veterinary Medicine
Department of Veterinary Clinical Sciences
1600 S. 16th Street
Ames, IA 50011-1250
USA
e-mail: msbergh@iastate.edu
Jeffery J. Biskup, DVM, Diplomate ACVS-SA
Assistant Professor
University of Tennessee
College of Veterinary Medicine
Department of Small Animal Clinical Sciences
2407 River Drive
Knoxville, TN 37996
USA
e-mail: jbiskup@utk.edu
Jason A. Bleedorn, DVM, MS, Dipomate ACVS
Clinical Assistant Professor of Small Animal
Orthopaedics
University of Wisconsin-Madison
School of Veterinary Medicine
2015 Linden Drive
Madison, Wisconsin 53706
USA
e-mail: jason.bleedorn@wisc.edu
xxi
VetBooks.ir
xxii
Contributing Authors
Randy J. Boudrieau, DVM, Diplomate ACVS,
ECVS
Professor
Tufts University
Cummings School of Veterinary Medicine
Department of Clinical Sciences
200 Westboro Road
North Grafton, MA 01536
USA
e-mail: randy.boudrieau@tufts.edu
Valentina Brioschi, DVM, GPCert(SAS),
MRCVS
Senior Clinical Training Scholar in Small
Animal Surgery
University of Cambridge
The Queen’s Veterinary School Hospital
Madingley Road
Cambridge CB3 0ES
United Kingdom
Dorothy Cimino Brown, MSCE, DVM,
Diplomate ACVS
Senior Research Advisor
Translational Comparative Medical Research
Elanco Animal Health
2500 Innovation Way
Greenfield, IN 46140
USA
e-mail: dottiedvm@gmail.com
Steven C. Budsberg, DVM, MS, Diplomate
ACVS
Professor
University of Georgia
College of Veterinary Medicine
Department of Small Animal Medicine &
Surgery
Athens, GA 30602
USA
e-mail: budsberg@uga.edu
Connie S. Chamberlain, PhD
Assistant Scientist
University of Wisconsin-Madison
School of Medicine & Public Health
Department of Orthopedics & Rehabilitation
1111 Highland Ave
Madison, WI 53705
USA
e-mail: cschamberlai@wisc.edu
Eithne Comerford, BVSc, PhD, CertVR, DSAO,
MRCVS
Professor
University of Liverpool
Faculty of Veterinary Science
Department of Veterinary Clinical Science
Leahurst
Chester High Road
Neston, CH64 7TE
United Kingdom
e-mail: eithne.comerford@liverpool.ac.uk
Michael G. Conzemius, DVM, PhD, Diplomate
ACVS
Endowned Professor of Surgery
University of Minnesota
College of Veterinary Medicine
Department of Veterinary Clinical Sciences
1365 Gortner Avenue
St Paul, MN 55108
USA
e-mail: conze012@umn.edu
Cristi R. Cook, DVM, MS, Diplomate ACVR
Thompson Laboratory for Regenerative
Orthopaedics
Missouri Orthopaedic Institute
University of Missouri-Columbia
1100 Virginia Avenue
Columbia, MO 65212
USA
e-mail: cookcr@missouri.edu
James L. Cook, DVM, PhD, Diplomate ACVS
William & Kathryn Allen Distinguished
Professor in Orthopaedic Surgery
Director, Comparative Orthopaedic
Laboratory, Orthopaedic Research Division &
Mizzou BioJoint Center
Missouri Orthopaedic Institute
University of Missouri
1100 Virginia Avenue
Columbia, MO 65212
USA
e-mail: cookjl@missouri.edu
Erin E. Crowley, DVM
Surgical Fellow
University of Wisconsin-Madison
School of Medicine & Public Health
Department of Orthopedics & Rehabilitation
VetBooks.ir
Contributing Authors
1111 Highland Ave
Madison, WI 53705
USA
Hilde de Rooster, DVM, MVM, PhD,
Diplomate ECVS
Professor in Soft Tissue Surgery
Ghent University
Faculty of Veterinary Medicine
Department of Small Animals
Salisburylann 133
B-9820 Merelbeke
Belgium
e-mail: hilde.derooster@ugent.be
Richard B. Evans, PhD
Waukesha, WI 53189
USA
e-mail: richard.bc.evans@gmail.com
Simone Forterre, Dr. med. vet, PhD
University of Bern
Vetsuisse Faculty Bern
Department of Clinical Veterinary Medicine
Längassstrasse 128
CH-3012 Bern
Switzerland
Samuel P. Franklin, MS, DVM, PhD, Diplomate
ACVS, ACVSMR
Assistant Professor of Small Animal
Orthopaedic Surgery
University of Georgia
Department of Small Animal Medicine &
Surgery
Veterinary Medical Center
2200 College Station Road
Athens, GA 30602
USA
e-mail: spfrank@uga.edu
Ingrid Gielen, DVM, PhD, MSC
Clinical Professor
Department of Veterinary Medical Imaging &
Small Animal Orthopaedics
Ghent University
Faculty of Veterinary Medicine
Salisburylann 133
9230 Merelbeke
Belgium
xxiii
Kei Hayashi, DVM, PhD, Diplomate ACVS
Associate Professor
Cornell University
College of Veterinary Medicine
Department of Clinical Sciences
School of Veterinary Medicine
Ithaca, NY 14853
USA
e-mail: kh528@cornell.edu
Donald A. Hulse, DVM, Diplomate ACVS
Professor
Texas A&M University
Department of Small Animal Clinical Sciences
College of Veterinary Medicine
College Station, TX 77843
USA
Kenneth A. Johnson, MVSc, PhD, FACVSc,
Diplomate ACVS
Professor
The University of Sydney
Faculty of Veterinary Science
Sydney, NSW 2006
Australia
e-mail: kennethjohnson@usyd.edu.au
Stanley E. Kim, BVSc, MS, Diplomate ACVS
Assistant Professor of Small Animal Surgery
University of Florida
College of Veterinary Medicine
Department of Small Animal Clinical Sciences
2015 SW 16th Ave
Gainsville, FL 32610
USA
e-mail: stankim@ufl.edu
Michael P. Kowaleski, DVM, Diplomate ACVS,
ECVS
Professor
Tufts University
Cummings School of Veterinary Medicine
Department of Clinical Sciences
200 Westboro Road
North Grafton, MA 01536
USA
e-mail: mike.kowaleski@tufts.edu
Anke Langenbach, Dr. med. Vet, Diplomate
ACVS, ACVSMR
Veterinary Surgical Centers
140 Part Street, SE
VetBooks.ir
xxiv
Contributing Authors
Vienna, VA 22180
USA
USA
e-mail: martha.murray@childrens.harvard.edu
William D. Liska, DVM, Diplomate ACVS
Global Veterinary Specialists
3130 Grants Lake Blvd
Sugar Land, TX 77496
USA
Gabriel S. Perrone
Research Technologist
Harvard University
Boston Children’s Hospital
Department of Orthopaedic Surgery
61 Binney Street, Enders 270.2
Boston, MA 02115
USA
e-mail: gabriel.perrone@childrens.harvard.edu
Denis J. Marcellin-Little, DEDV, Diplomate
ACVS, ACVSMR
Professor, Small Animal Orthopedic Surgery
University of California, Davis
School of Veterinary Medicine
Department of Surgical and Radiological
Sciences
One Shields Avenue
Davis, CA 95616
USA
e-mail: djmarcel@ucdavis.edu
Noël M.M. Moens, DVM, MSc, Diplomate
ACVS, ECVS
Associate Professor of Orthopaedic Surgery
University of Guelph
Ontario Veterinary College
Department of Clinical Studies
Guelph, ON N1G 2W1
Canada
e-mail: nmoens@ovc.uoguelph.ca
Peter Muir, BVSc, MVetClinStud, PhD,
Diplomate ACVS, ECVS, MRCVS
Melita Grunow Family Professor of
Companion Animal Health
University of Wisconsin-Madison
School of Veterinary Medicine
Department of Surgical Sciences
2015 Linden Drive
Madison, Wisconsin 53706
USA
e-mail: peter.muir@wisc.edu
Martha M. Murray, MD
Professor in Orthopedic Surgery
Harvard University
Boston Children’s Hospital
Department of Orthopaedic Surgery
Hunnewell 2
300 Longwood Avenue
Boston, MA 02115
Antonio Pozzi, Prof. Dr. med. vet, Diplomate
ACVS, ACVSMR
University of Zurich
Vetsuisse Faculty
Clinic for Small Animal Surgery
Winterthurerstrasse 258c
8057, Zurich
Switzerland
e-mail: apozzi@vetclinics.uzh.ch
Simon C. Roe, BVSc, PhD, Diplomate ACVS
Professor of Orthopaedic Surgery
North Carolina State University
College of Veterinary Medicine
Department of Clinical Sciences
1052 William Moore Drive
Raleigh, NC 27607
USA
e-mail: simon_roe@ncsu.edu
Susannah J. Sample, DVM, MS, PhD,
Diplomate ACVS
Assistant Scientist
University of Wisconsin-Madison
Comparative Orthopaedic and Genetics
Research Laboratory
School of Veterinary Medicine
2015 Linden Drive
Madison, Wisconsin 53706
USA
e-mail: susannah.sample@wisc.edu
Susan L. Schaefer, DVM, MS, Diplomate ACVS
Clinical Associate Professor of Small Animal
Orthopaedics
University of Wisconsin-Madison
School of Veterinary Medicine
Department of Surgical Sciences
VetBooks.ir
Contributing Authors
2015 Linden Drive
Madison, Wisconsin 53706
USA
e-mail: susan.schaefer@wisc.edu
Peter V. Scrivani, DVM, Diplomate ACVR
Associate Professor
Cornell University
College of Veterinary Medicine
Department of Clinical Sciences
Ithaca, NY 14853
USA
e-mail: pvs2@cornell.edu
David E. Spreng, Prof. Dr. Med. vet, Diplomate
ECVS, ACVECC EMBA PHW
University of Bern
Vetsuisse Faculty Bern
Department of Clinical Veterinary Medicine
Längassstrasse 128
CH-3012 Bern
Switzerland
e-mail: david.spreng@vetsuisse.unibe.ch
Selena Tinga, DVM
Resident in Small Animal Surgery
University of Florida
College of Veterinary Medicine
Department of Small Animal Clinical Sciences
2015 SW 16th Ave
Gainsville, FL 32610
USA
Email addresses are listed for corresponding authors
for each chapter. Contact information, including email
addresses, for contributors who are ACVS and ECVS
Diplomates is also available from www.acvs.org and
www.ecvs.org, respectively.
xxv
Henri Van Bree, DVM, PhD, Diplomate ECVDI,
ECVS
Professor
Ghent University
Faculty of Veterinary Medicine
Department of Veterinary Medical Imaging &
Small Animal Orthopaedics
Salisburylann 133
B-9820 Merelbeke
Belgium
e-mail: henri.vanbree@ugent.be
Ray Vanderby Jr., PhD
Professor
University of Wisconsin-Madison
School of Medicine & Public Health
Department of Orthopedics & Rehabilitation
1111 Highland Ave
Madison, WI 53705
USA
e-mail: ray.vanderby@wisc.edu
Patrick Vavken, MD
Lecturer in Orthopedic Surgery
Harvard University
Boston Children’s Hospital
Department of Orthopedic Surgery
Orthopedics, Enders 1016
300 Longwood Avenue
Boston, MA 02115
USA
e-mail: patrick.vavken@childrens.harvard.edu
VetBooks.ir
VetBooks.ir
Section I
Structure and Function
Introduction
The anatomy of canine stifle is complex. Our
understanding of the anatomy of the cranial
and caudal cruciate ligaments has gradually
evolved over time, particularly with regard to
the microvascular anatomy of the ligaments.
Recent work suggesting the existence of a
blood–cruciate ligament barrier, analogous
to the blood–brain barrier, is a particularly
interesting finding, which helps explain the
mechanism that leads to incremental fiber rupture within the ligament matrix of both cruciate
ligaments over time, and eventual rupture of
the cranial cruciate ligament. In addition to
their biomechanical role as joint stabilizers, the
cranial and caudal cruciate ligaments likely
have key functions in joint proprioception.
In the future, advances in knowledge of ligament matrix homeostasis effects on cruciate
ligament mechanical properties and associated
joint laxity should provide insight into the
ligament rupture mechanism. Variation in joint
proprioception and joint laxity may ultimately
explain how fiber rupture is initiated in the
early phase of the disease. An important weakness with current surgical treatments for the
unstable stifle is that repair of the ruptured
cranial cruciate ligament is not performed.
This section provides a detailed discussion of
stifle anatomy, including gross and microscopic
anatomy of the cruciate ligaments.
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
1
VetBooks.ir
VetBooks.ir
1
Morphology and Function
of the Cruciate Ligaments
Hilde de Rooster and Eithne Comerford
Introduction
In contrast to the plethora of veterinary publications on cruciate surgery in dogs, only a
few papers deal with the microanatomy and
neurovascular anatomy of the canine cruciate
ligaments. However, an understanding of the
complex anatomy and function of these ligaments is imperative to elucidate the pathophysiology of cruciate ligament rupture, and to
improve surgical intervention.
Morphology
Macroanatomy
The cranial cruciate ligament (CrCL) attaches to
the axial aspect of the lateral femoral condyle,
very close to the articular margin (Figure 1.1).
It extends diagonally across the joint space and
attaches to the cranial intercondyloid area of
the tibial plateau (Singleton 1957; Zahm 1965;
Arnoczky & Marshall 1977). The proximal
attachment site is bordered cranially by the
cranial meniscotibial ligament of the medial
meniscus and caudally by the cranial menis-
cotibial ligament of the lateral meniscus (Rudy
1974; Heffron & Campbell 1978) (Figure 1.2).
The CrCL is narrowest in its mid-region and
fans out proximally and distally (Alm et al.
1975; Heffron & Campbell 1978). The length
of the CrCL is positively correlated with body
weight; taking the average length of its cranial
and caudal borders, the mean length has been
reported as 13.5–18.7 mm (Vasseur et al. 1985;
Wingfield et al. 2000; Comerford et al. 2005). The
CrCL runs cranially, medially, and distally in
an outward spiral as it passes from the femur to
the tibia (Zahm 1965; Haut & Little 1969). Two
demonstrably separate bundles are apparent
(Figure 1.1) (Arnoczky & Marshall 1977; Heffron & Campbell 1978); these components are
termed craniomedial and caudolateral, based
on their relative attachment sites onto the tibial
plateau. The craniomedial subdivision is the
most spiral and the longest, yet smaller, component, and arises more proximally from the
femur and attaches more cranially on the tibial
footprint area, compared with the caudolateral
subdivision. The fibers of the caudolateral
component arise from the most lateral and
distal part of the attachment area of the lateral
femoral condyle, have a straighter path, and
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
3
Structure and Function
VetBooks.ir
4
2
5
6
3
4
1a
1b
7
(A)
(B)
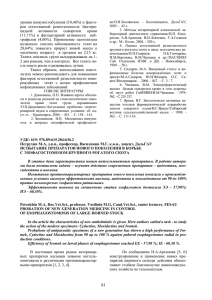
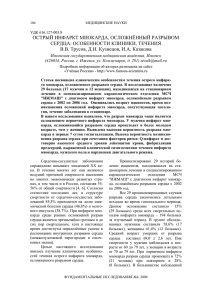
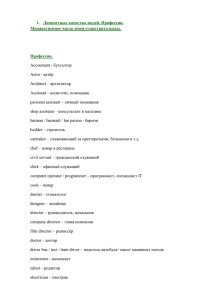
Figure 1.1 Photograph (A) and line drawing (B) of a flexed right stifle joint of a dog. Cranial view after removal of the
infrapatellar fat pad. In panel B: 1a, caudolateral bundle of the cranial cruciate ligament; 1b, craniomedial bundle of the
cranial cruciate ligament; 2, caudal cruciate ligament; 3, medial meniscus; 4, lateral meniscus; 5, tendon of the long
digital extensor; 6, medial femoral condyle; 7, tibial tuberosity.
12
11
4
10
5
1
9
3
2
6
(A)
(B)
7
8
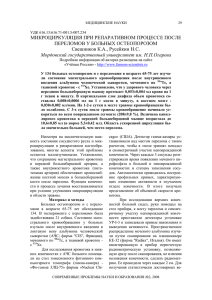
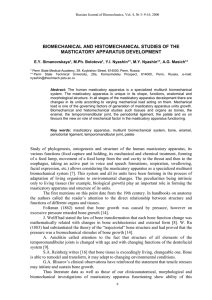
Figure 1.2 Photograph (A) and line drawing (B) of the left pelvic limb of a dog. Dorsal view on the tibial plateau after
removal of the femur. In panel B: 1, cranial cruciate ligament; 2, caudal cruciate ligament; 3, medial meniscus; 4,
intermeniscal ligament; 5, medial collateral ligament; 6, lateral meniscus; 7, meniscofemoral ligament; 8, popliteal
tendon; 9, tendon of the long digital extensor; 10, infrapatellar fat pad; 11, patellar tendon; 12, patella.
VetBooks.ir
Morphology and Function of the Cruciate Ligaments
attach on the most caudal region of the tibial
footprint area (Arnoczky & Marshall 1977;
Heffron & Campbell 1978).
The caudal cruciate ligament (CaCL) is
slightly longer and broader than the CrCL
(Rudy 1974; Arnoczky & Marshall 1977; Harari
1993). Even its collagen fibrils are thicker compared with its cranial counterpart (Brunnberg
1989). The total mid-section diameter is smallest as it fans out from the center, making
the femoral and, to a lesser extent, the tibial attachments larger (Rudy 1974). In the
dog the CaCL also has two components,
although they are less distinct and often
inseparable (Heffron & Campbell 1978; Harari
1993).
Microanatomy
The cruciate ligaments are multifascicular
structures, the base unit of which is collagen,
that contain many wavy fascicular subunits
(Figure 1.3A). Fascicles may be composed of
one up to 10 subfascicles, containing bundles of collagen fibers (Heffron & Campbell
1978; Yahia & Drouin 1989). At the osseous
attachment sites of the CrCL, the collagen
fibers are not arranged entirely parallel to
the longitudinal axis of the ligament and,
especially in younger specimens, columns of
5
chondroid cells do penetrate into the ligament
(Figure 1.3B) (Zahm 1965; Alm & Strömberg
1974). Where both cruciate ligaments are in
contact, the collagen fibers are more densely
packed and oriented tangential to the surface
instead of parallel to the long axis (Vasseur
et al. 1985). Fibers are formed by fibrils that are
composed by organization of repeated collagen
subunits (Alm & Strömberg 1974; Heffron &
Campbell 1978; Vasseur et al. 1985). Their architecture is a combination of helical or planar,
parallel, or twisted networks. The centrally
located collagen fibrils are nearly straight,
whereas those at the periphery are arranged
in a helical wave pattern (Zahm 1965; Alm &
Strömberg 1974; Yahia & Drouin 1989).
Alongside collagen, elastin fibers and bundles of microfibrils (fibrillin 1 and 2) are
abundant in cruciate ligaments, both within
the collagen bundles and in the interfascicular
regions (Figures 1.4AB) (Smith et al. 2011). Those
fibers are predominantly orientated parallel to
the collagen bundles, and this study suggested
a mechanical role for their distribution during
ligament deformation.
As evident in other ligaments, the cruciate ligaments are characterized by relative hypocellularity. Where both cruciate ligaments are in
contact, the epiligament is more cellular than
anywhere else (Smith et al. 2012). In the interfascicular regions, the cells are interspersed
TibialBone
Cartilage
B
CrCL
A
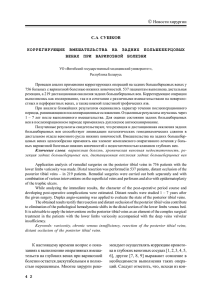
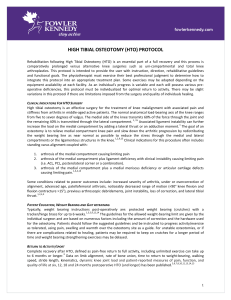
Figure 1.3 Histologic section (H&E stain) of a
normal cranial cruciate ligament (CrCL) of a
4-month-old Riezenschnauzer. (A) Along the
CrCL, dense collagen is aligned parallel to the
long axis of the ligament. The collagen fibers
have a regular accordion-like pattern. (B) At the
attachment site of the CrCL, the collagen is not
arranged entirely parallel to the long axis of the
ligament. Columns of chondroid cells (arrow) do
penetrate into the CrCL (scale bar = 100 μm).
Source: de Rooster et al. 2006. Reproduced with
permission from John Wiley & Sons, Inc.
(A)
(B)
Structure and Function
VetBooks.ir
6
(A)
(B)
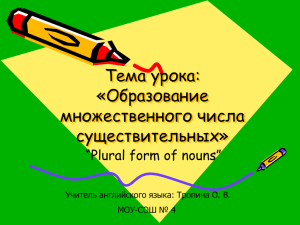
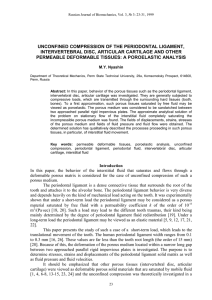
Figure 1.4 (A) Distribution of fibrillin-1 in the canine cruciate ligament complex, longitudinal section cranial cruciate
ligament (CrCL), ×63 confocal laser scanning microscopy (CLSM) image, enzymatic pre-treatment. Fibrillin 1 (orange) is
found pericellularly where nuclei are rounded (nuclei shown in blue). Staining of fibrillin 1 is also seen extending
parallel to collagen in a fiber-like structure (arrows) from an elongated nucleus. Although some co-localization (yellow)
is seen with elastin (green), elastin fibers were generally found to contain little fibrillin 1. Scale bar = 50 μm. (B)
Distribution of fibrillin-2 in the canine cruciate ligament complex, longitudinal section CrCL, ×63 CLSM image from
fascicular region showing fibrillin-2 (red) in long and dense fibers broadly aligned with collagen bundles, with some
branching. Nuclei are stained with DAPI (blue). Scale bar = 50 μm. Source: Smith et al. 2011. Reproduced with
permission from John Wiley & Sons, Inc.
between bundles of collagenous fibers. Most
are interconnected by cytoplasmic projections,
which often branch markedly, forming a threedimensional cellular lattice around those fibers.
Differences in cell morphology were also found
in dog breeds with high and low risks of
cruciate ligament rupture. CrCLs from lowrisk breeds have longer cytoplasmic projections,
while high-risk CrCLs have rounder nuclei and
shorter cytoplasmic projections. These changes
may be indicative of a reduced communication
between cells (Smith et al. 2012).
structures (Vasseur et al. 1985). Compared with
the collateral ligaments, the enveloping synovial membrane is relatively cellular (Heffron &
Campbell 1978). Synovial lining does not occur
on the surfaces of the cruciate ligaments that
are in direct contact with each other (Vasseur
et al. 1985). When examined with scanning electron microscopy, many small holes have been
detected in the synovial membrane covering
the cruciate ligaments, suggesting that the cruciate ligaments are also supplied with nutrients
via the synovial fluid (Kobayashi et al. 2006).
Synovial envelope
Vascular supply
Both the CrCL and the CaCL are covered by
a fairly uniform fold of synovial membrane
which incompletely divides the stifle joint
in the sagittal plane (Arnoczky et al. 1979).
These enveloping epiligamentous membranes
consist mainly of dense connective tissue, small
fibroblasts, and some adipocytes; an intima and
a thin subintimal layer can be distinguished
(Heffron & Campbell 1978). The intima is a
single layer of synoviocytes, and the subintimal
layer is areolar tissue containing small vascular
The major vascular contribution to the center
of the stifle joint occurs from branches of the
middle genicular artery, which arises from the
popliteal artery, penetrates the caudal joint
capsule, and passes craniodistally to the fossa
intercondylaris, running cranially between the
cruciate ligaments (Figures 1.5 and 1.6) (Tirgari
1978). The vascular structures in the proximal
part of the CrCL are more numerous and have
a larger diameter compared with those on the
tibial side (Zahm 1965; Alm & Strömberg 1974).
VetBooks.ir
Morphology and Function of the Cruciate Ligaments
7
1
4
3
3
2
5
1
2
4
Figure 1.6 Photograph of the superficial vascularization
of normal cruciate ligaments after injection of latex in an
ex vivo specimen of an adult dog. The infrapatellar fat
pad and the synovial envelope are the most important
sources of vessels. 1, cranial cruciate ligament; 2, caudal
cruciate ligament; 3, lateral femoral condyle; 4, tibial
plateau. Source: de Rooster et al. 2006. Reproduced with
permission from John Wiley & Sons, Inc.
7
6
Figure 1.5 Line drawing of the major blood supply to
the canine stifle joint. Caudal view. 1, femoral artery; 2,
popliteal artery; 3, descending genicular artery; 4,
proximal medial genicular artery; 5, middle genicular
artery; 6, cranial tibial artery; 7, caudal tibial artery.
Source: de Rooster et al. 2006. Reproduced with
permission from John Wiley & Sons, Inc.
The blood supply to both cruciate ligaments
is predominantly of soft tissue origin; the contribution from the osseous attachments is negligible (Arnoczky et al. 1979; Kobayashi et al.
2006). The infrapatellar fat pad and the wellvascularized synovial membranes, which form
an envelope around the cruciate ligaments, are
the most important sources of vessels (Alm &
Strömberg 1974; Tirgari 1978; Arnoczky et al.
1979, Kobayashi et al. 2006). The synovial vessels arborize into a finely meshed network of
epiligamentous vessels which ensheath the cruciate ligaments throughout their entire length
(Figures 1.7 and 1.8) (Arnoczky et al. 1979;
3
2
1
4
Figure 1.7 Arthroscopic view of the superficial
vascularization of normal cruciate ligaments of an adult
dog. The synovial vessels arborize to form a web-like
network of periligamentous vessels that ensheath the
cruciate ligaments. 1, cranial cruciate ligament; 2, caudal
cruciate ligament; 3, lateral femoral condyle; 4, tibial
plateau. Source: de Rooster et al. 2006. Reproduced with
permission from John Wiley & Sons, Inc.
Structure and Function
VetBooks.ir
8
1
2
CrCL
3
(A)
4
CrCL
SM
1
(B)
Figure 1.8 Histologic section (H&E stain) of a normal
cranial cruciate ligament (CrCL) of an adult dog. (A) The
CrCL is ensheathed by epiligamentous vessels (scale
bar = 100 μm). (B) The well-vascularized synovial
membrane (SM) forms an envelope over the CrCL (scale
bar = 100 μm). 1, epiligamentous vessels; 2, anastomosis
between epiligamentous and endoligamentous vessels; 3,
hypovascular zone; 4, synovial vessels. Source: de
Rooster et al. 2006. Reproduced with permission from
John Wiley & Sons, Inc.
Kobayashi et al. 2006). In general, the vascular arrangement and structural characteristics of
the vasculature inside the CrCL and the CaCL
are similar (Alm & Strömberg 1974; Arnoczky
et al. 1979; Kobayashi et al. 2006). In the inner
part of the cruciate ligaments, around and along
the bundles of collagen fibers, an endoligamentous vascular network courses in the supporting connective tissue (Alm & Strömberg 1974;
Arnoczky et al. 1979; Hayashi et al. 2011). The
larger vessels, usually one artery accompanied
by two veins, mainly course in a longitudinal direction both proximally and distally and
lie parallel to the collagen fascicles (Alm &
Strömberg 1974). Some of them have a tortuous
path in the interfascicular areolar tissue. Only
small capillaries branching from the longitudinal endoligamentous vessels run in a transverse
direction, encircling collagen bundles. The core
of the mid-portion of the CrCL is less well vascularized compared with the remainder of the
ligament (Zahm 1965; Tirgari 1978; Arnoczky
et al. 1979; Vasseur et al. 1985; Hayashi et al.
2011).
Anastomoses exist between extra- and
intraligamentous blood networks (Alm &
Strömberg 1974; Arnoczky et al. 1979;
Kobayashi et al. 2006). Epiligamentous vessels penetrate transversely into the cruciate
ligaments (Figure 1.8). Their branches ramify
and anastomose with the endoligamentous
vessels. There are numerous endosteal vessels
at the ligamentous–osseous junctions; however,
communications with intrinsic endoligamentous vessels are quite poor, especially at the
tibial attachment where most of the endosteal
vessels seem to terminate in subchondral loops
instead of crossing the ligamentous–osseous
junction (Alm & Strömberg 1974; Arnoczky
et al. 1979; Kobayashi et al. 2006).
Innervation
Three major articular nerves arise from the
saphenous nerve, tibial nerve, and common
peroneal nerve to innervate the periarticular
tissues of the canine stifle joint (Figure 1.9)
(O’Connor & Woodbury 1982). The main trunk
of nerve bundles is found at the femoral end of
the cruciate ligaments. Other nerves may contribute afferent fibers to a variable extent to the
cruciate ligaments.
In dogs, the medial articular nerve, which
branches from the saphenous nerve in the
mid-thigh region, provides the largest contribution to stifle joint innervation (O’Connor &
Woodbury 1982). Some of its branches course
through the infrapatellar fat pad to terminate
within the proximal or distal attachments of
the cruciate ligaments or within the meniscal
poles. Other branches of the medial articular
nerve pass cranially through the joint capsule to
VetBooks.ir
Morphology and Function of the Cruciate Ligaments
9
1
1
2
2
4
5
3
3
6
Figure 1.9 Line drawing of the major nerve
supply to the canine stifle joint. (A) Medial view.
(B) Lateral view. 1, saphenous nerve; 2, medial
articular nerve; 3, caudal articular nerve; 4,
common peroneal nerve; 5, tibial nerve; 6,
lateral articular nerve. Source: de Rooster et al.
2006. Reproduced with permission from John
Wiley & Sons, Inc.
(A)
extensively innervate the femoral attachment of
the CaCL. The caudal articular nerve is variably
present in dogs (O’Connor & Woodbury 1982),
its branches arising either directly from the
tibial nerve or from a muscular branch of the
tibial nerve. The caudal articular nerve runs to
the caudal aspect of the joint capsule, where it
may communicate with branches of the medial
articular nerve. The lateral articular nerve
branches from the common peroneal nerve
at the level of the fibular head, deep to the
biceps femoris muscle, and supplies the lateral
aspect of the stifle joint (O’Connor & Woodbury
1982).
Nerves of differing sizes are located in the
richly vascularized synovial tissue covering the
cruciate ligaments (Yahia et al. 1992). From this
peripheral synovium, axons radiate towards
the center of the ligaments (Yahia et al. 1992).
Within the cruciate ligaments, most nerves
course along the epiligamentous and endoligamentous blood vessels in the interfascicular areolar spaces.
Neurohistologic studies have identified various types of sensory nerve endings (receptors
and free nerve endings) in the middle of the
cruciate ligaments, well beneath the synovial
sheath (Yahia et al. 1992). The highest number of
mechanoreceptors was found in the proximal
third of the CrCL, and the lowest in the distal
(B)
third (Arcand et al. 2000). A high percentage of
mechanoreceptors have been found in the tibia
remnants of ruptured human anterior cruciate
ligaments (ACLs), and it has been suggested
that leaving these remnants after ACL reconstruction may be important for postoperative
proprioceptive function (Sha & Zhao 2010).
Functional anatomy
The cruciate ligaments resist forces that would
cause the tibia to translate cranially relative to
the femur and, to a lesser degree, resist forces
that would cause tibial rotation (Arnoczky &
Marshall 1977). The two components of the
CrCL are not isometric, the main difference
being elongation of the craniomedial and shortening of the caudolateral component during
flexion (Arnoczky & Marshall 1977; Heffron &
Campbell 1978). The former is the major
contributor to craniocaudal stability in stifle
flexion, while the latter only contributes when
the craniomedial band is damaged or severely
stretched (Wingfield et al. 2000). With the stifle
in extension, both components are taut, and
limit cranial translation of the tibia relative
to the femur (Arnoczky & Marshall 1977;
Heffron & Campbell 1978).
VetBooks.ir
10
Structure and Function
As the stifle flexes, the cruciate ligaments are
not only wrapped upon each other but also spiral on themselves (Singleton 1957; Arnoczky &
Marshall 1977). The higher strain in the ligaments also limits the amount of normal internal
rotation of the tibia relative to the femur (Zahm
1965; Arnoczky & Marshall 1977; Harari 1993).
In extension, the medial and lateral collateral
ligaments become the primary restraints of rotation, and the cruciate ligaments provide only a
secondary check from the tension in both ligaments (Singleton 1957; Zahm 1965; Vasseur et al.
1985).
Both cruciate ligaments together provide
important secondary restraints against varus
and valgus angulation. The cruciate ligaments
become primary restraints if there is loss of collateral ligament support (Vasseur & Arnoczky
1981).
Overextension is prevented by tension in
the cruciate ligaments, where the CrCL acts as
the primary restraint (Arnoczky & Marshall
1977; Heffron & Campbell 1978). The caudolateral component of the CrCL is the primary
contributor to restraining hyperextension (Heffron & Campbell 1978). The slightly longer
caudal component of the CaCL can only be
considered a secondary restraint (Singleton
1957; Arnoczky & Marshall 1977).
References
Alm A, Ekström H, Strömberg B. Tensile strength of
the anterior cruciate ligament in the dog. Acta Chir
Scand Suppl 1975;445:15–23.
Alm A, Strömberg B. Vascular anatomy of the patellar
and cruciate ligaments. A microangiographic and
histologic investigation in the dog. Acta Chir Scand
Suppl 1974;445:25–35.
Arcand MA, Rhalmi S, Rivard C-H. Quantification of
mechanoreceptors in the canine anterior cruciate
ligament. Int Orthop 2000;24:272–275.
Arnoczky SP, Marshall JL. The cruciate ligaments of
the canine stifle: an anatomical and functional analysis. Am J Vet Res 1977;38:1807–1814.
Arnoczky SP, Rubin RM, Marshall JL. Microvasculature of the cruciate ligaments and its response to
injury. An experimental study in dogs. J Bone Joint
Surg 1979;61A:1221–1229.
Brunnberg L. Klinische Untersuchungen zu Ätiologie
und Pathogenese der Ruptur des Ligamentum cruciatum craniale beim Hund. 2. Mitteilung: Zur
Ätiologie und Diagnose der Ruptur des Ligamentum cruciatum craniale beim Hund. Kleintierprax
1989;34:445–449.
Comerford E, Tarlton J, Innes J, et al. Metabolism and
composition of the canine anterior cruciate ligament relate to difference in knee joint mechanics
and predisposition to ligament rupture. J Orthop
Res 2005;23:61–66.
de Rooster H, de Bruin T, van Bree H. Morphologic
and functional features of the canine cruciate ligaments. Vet Surg 2006;35:769–780.
Harari J. Caudal cruciate ligament injury. Vet Clin
North Am Small Anim Pract 1993;23:821–829.
Haut RC, Little RW. Rheological properties of canine
anterior cruciate ligaments. J Biomech 1969;2:289–
298.
Hayashi K, Bhandal J, Kim SY, et al. Immunohistochemical and histomorphometric evaluation of
vascular distribution in intact canine cranial cruciate ligament. Vet Surg 2011;40:192–197.
Heffron LE, Campbell JR. Morphology, histology and
functional anatomy of the canine cranial cruciate
ligament. Vet Rec 1978;102:280–283.
Kobayashi S, Baba H, Uchida K, et al. Microvascular system of anterior cruciate ligament in dogs.
J Orthop Res 2006;24:1509–1520.
O’Connor BL, Woodbury P. The primary articular
nerves to the dogs knee. J Anat 1982;134:563–
572.
Rudy RL. Stifle joint. In: Canine Surgery, Archibald J,
ed. Santa Barbara CA, American Veterinary Publications Inc. 1974, pp 1104–1115.
Sha L, Zhao L. Quantitative study on mechanoreceptors in tibial remnants of ruptured anterior cruciate
ligament in human knees. Zhongguo Xiu Fu Chong
Jian Wai Ke Za Zhi 2010;24:1318–1322.
Singleton WB. The diagnosis and surgical treatment
of some abnormal stifle conditions in the dog. Vet
Rec 1957;69:1387–1394.
Smith KD, Vaughan-Thomas A, Spiller DG, et al. The
organisation of elastin and fibrillins 1 and 2 in the
cruciate ligament complex. J Anat 2011;218:600–
607.
Smith KD, Vaughan-Thomas A, Spiller DG, et al. Variations in cell morphology in the canine cruciate ligament complex. Vet J 2012;193:561–566.
Tirgari M. The surgical significance of the blood supply of the canine stifle joint. J Small Anim Pract
1978;19:451–462.
Vasseur PB, Arnoczky SP. Collateral ligaments of the
canine stifle joint: Anatomic and functional analysis. Am J Vet Res 1981;42:1133–1137.
Vasseur PB, Pool RR, Arnoczky SP, et al. Correlative biomechanical and histologic study of the
cranial cruciate ligament in dogs. Am J Vet Res
1985;46:1842–1854.
Wingfield C, Amis AA, Stead AC, et al. Cranial
cruciate stability in the Rottweiler and racing
VetBooks.ir
Morphology and Function of the Cruciate Ligaments
Greyhound: an in vitro study. J Small Anim Pract
2000;41:193–197.
Yahia LH, Drouin G. Microscopical investigation of
canine anterior cruciate ligament and patellar tendon: Collagen fascicle morphology and architecture. J Orthop Res 1989;7:243–251.
11
Yahia LH, Newman NM, St Georges M. Innervation
of the canine cruciate ligaments. A neurohistological study. Anat Histol Embryol 1992;21:1–8.
Zahm H. Die Ligamenta decussata in gesunden und
arthrotischen Kniegelenk des Hundes. Kleintierprax 1965;10:38–47.
VetBooks.ir
VetBooks.ir
2
Biomechanics of the Cruciate
Ligaments
Susannah J. Sample
Introduction
Stifle joint kinematics is the result of a complex
mechanical system. Stability is provided by a
combination of static and dynamic structures,
with the cruciate ligaments acting as main stabilizers, providing transitional and rotational
constraint. The canine cranial cruciate ligament
(CrCL) is the most widely studied ligament in
veterinary medicine. Over the past 40 years,
studies of the CrCL have been primarily focused
on either surgical methods to replace its function after rupture, or advancing the understanding of histological and mechanical age-related
degeneration. Unlike in humans, little is known
about the specific biomechanical properties of
the CrCL in dogs. More detailed biomechanical descriptions of the CrCL are needed as technologies for ligament replacement procedures
in dogs evolve.
Biomechanical properties refer to the relationship between the length and tension of a
given biologic material. This chapter will provide a short overview of the biomechanical
properties of ligaments, and summarize what
is known about the biomechanics of the canine
CrCL. Biologic factors and disease conditions
that are known to influence the biomechanical
properties of ligament will also be discussed,
as will the biomechanics of graft materials
that have been considered for possible cruciate
repair.
Ligament composition
Ligaments have a hierarchical architecture (Figure 2.1) and consist of a combination of water
and longitudinally running collagen fibers,
which are mostly type I collagen (70–80% of tissue dry weight and >90% of collagen), with a
small amount of type III collagen (3–10%). Minimal amounts of types V, X, XII and XIV collagen,
elastin, and proteoglycans are also components.
The hierarchical architecture of the ligament
influences its mechanical properties. Ligament
is made up of multiple smaller structures called
fiber bundles (Figures 2.1 and 2.2). Each fiber
bundle, in turn, is comprised of the basic fibers
of the ligament and includes fibroblasts; fibroblasts are the primary cells that make up both ligament and tendon. Ligament fibers have a varying amount of crimp (Figure 2.2). Crimp is a sort
of wave within collagen fibers (Figures 2.1 and
2.2), and is the primary driving force behind the
nonlinear stress–strain relationship that exists
initially when the ligament undergoes tensile loading. Crimp facilitates a progressive
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
13
VetBooks.ir
14
Structure and Function
Evidence:
x-ray
EM
x-ray
EM
x-ray
MICROFIBRIL
SUBFIBRIL
x-ray
EM
SEM
EM
SEM
OM
SEM
OM
FIBRIL
FIBER
BUNDLES
FIBER
TROPOCOLLAGEN
3.5 nm staining
sites
64 nm
periodicity
crimp structure
fibroblasts
fascicular
(45–50 μ)
membrane
1.5 nm
10–20 nm
50–500 nm
50–300 μ
reticular
membrane
100–500 μ
3.5 nm
Size scale
Figure 2.1 Diagram illustrating the hierarchical organization of ligaments and tendons. Ligament has a hierarchical
structure, starting at the level of individual fibroblasts. These cells are arranged to create a series of fibril structures,
which eventually results in the formation of fibers. Fiber bundles or fascicles then combine to create the ligament itself. It
should be noted that tendons also possess this basic hierarchical architecture. EM, electron microscopy; SEM, scanning
electron microscopy; OM, optical microscopy. Source: SEB Symposia XXXIV 1980 The mechanical properties of
biological tissues. Reproduced with permission from the Society of Experimental Biology.
recruitment of fibers to resist load. Crimped
fibers also help to provide resistance at extremes
of joint motion.
The strength of ligament and tendon relates
to the diameter of its composite fibrils; thicker
fibrils have a greater effect on tensile strength,
and are considered determinants thereof
(Ottani et al. 2001). In horses, the effect of
exercise on collagen fibril diameter has been
of great interest, particularly with regards
to superficial and deep digital flexor tendon
injury. These studies have shown that exercise
initially increases fibril diameter, but exerciseinduced microdamage results in a decrease in
fibril diameter (Cherdchutham et al. 2001).
The CrCL is unique in architecture and function. It is a continuum of fibers from a distal cranial medial orientation on the lateral
femoral condyle to the cranial central interspinous area of the tibial plateau. These fibers
are recruited differentially throughout stifle
flexion so that fibers are often defined by functional bundles. Most commonly, two bundles
are described, the cranial medial (CM) bundle
and the caudal lateral (CL) bundle. In extension, both fiber bundles are tight and parallel,
whereas in flexion the structure twists when
the femoral attachment of the CrCL rolls back.
When this occurs, the CL bundle becomes slack,
while the CM bundle remains load-bearing.
The reduced number of CrCL fibers which
are load-bearing during flexion consequently
makes them more vulnerable to overstretch
damage.
Biomechanical properties
Because ligaments are designed to transfer load
from bone to bone in a longitudinal direction, uniaxial tensile tests are used to characterize structural and material properties of ligament using force–deformation and stress–strain
curves, respectively. Typically, all CrCL testing is done with the stifle extended to recruit
fibers from both fiber bundles. This provides a
best case scenario for strength and stiffness and
comparable biomechanical properties. Stifle
Biomechanics of the Cruciate Ligaments
15
VetBooks.ir
during sustained loads (creep), and tensile
load required to maintain a fixed position will
decrease with time (relaxation). While important, these biomechanical characteristics are
often considered secondary. Consequently, testing protocols ‘pre-condition’ specimens with
repeated loads and testing at a constant rate of
loading to minimize secondary effects, producing a standard force versus deformation curve
that can be used for biomechanical comparison.
Force–deformation curve
(A)
Structural properties are described using a
force–deformation curve, which can be divided
into three regions (Figure 2.3). The first is the
toe region, which is nonlinear and has a low initial stiffness; in this region, due to the crimped
nature of collagen fibers, small forces result in
a relatively large degree of lengthening. The
next region is the linear region, which displays
700
Ultimate Strength
(B)
Figure 2.2 Longitudinal section of intact cranial
cruciate ligament (CrCL) from a 1.5-year-old female
beagle viewed using bright light (A) and circularly
polarized light (B). Intact CrCL from young dogs has a
hierarchically organized structure. Birefringence of the
extracellular matrix collagen and the crimped structure
are clearly visible in polarized light as bright and dark
repeating bands within ligament fibers. Crimp is a
wave-like feature of ligament that exists at the level of the
fiber, and is the primary reason for ligament’s nonlinear
elasticity. Scale bar = 50 μm.
loading in any off-axis direction and/or with
some stifle flexion would result in different stiffness and strength.
All ligaments are viscoelastic in their mechanical behavior. That is, their stretch will increase
500
Linear Slope
400
300
Energy-to-failure
200
100
0
5
10
Deformation (mm)
Ultimate Elongation
Force (N)
600
15
Figure 2.3 Typical force–deformation curve for
ligament during uniaxial tensile testing. The
force–deformation curve of ligament can be divided into
three regions. The toe region is the initial nonlinear part
of the curve, which is primarily due to the existence of
crimp at the level of the fiber. In this region, small forces
result in a large degree of lengthening because of the
crimped nature of the collagen fibers. The second is the
linear region, which occurs after crimp has been
maximally stretched. The linear slope of this region is
reflective of the material’s stiffness. The final region is the
point at which a ligament begins to rupture; the peak of
this part of the curve gives the material’s ultimate strength
and ultimate elongation values.
Structure and Function
Stress–strain curve
Stress is defined as load (MPa) divided by crosssectional area, and is calculated using known
load data and a cross-sectional measurement of
the ligament. Strain can be thought of as deformation, and is defined as the change in length
divided by original length; during uniaxial tensile testing, strain can be directly determined.
The stress–strain curve can be divided into three
regions (Figure 2.4). The first is the toe region,
at which point large changes in strain result in
minimal stress being applied; it is in this region
that the “un-crimping” of collagen fibers occurs
as they are being recruited to bear load. The
next is the linear region, which occurs when the
ligament fibers themselves are being stretched.
The slope of this linear region defines Young’s
modulus (a.k.a. elastic modulus or modulus).
Young’s modulus describes the properties of
the composite material, including all of its solid
and fluid constituents. The last region occurs
when the ligament begins to rupture, when
the stiffness is reduced. The point before this
decrease in stiffness defines ultimate stress and
ultimate strain of the tissue. When sufficient
fiber damage has occurred and elongation continues, the remaining fibers rupture and the ligament breaks. The area under the curve before
failure is called the strain–energy density, and
reflects the energy stored in the elastic ligamentous material.
80
Yi
el
d
Ultimate Stress
70
60
50
40
Young’s
Modulus
30
Strain-energy
density
20
Ultimate Strain
a high degree of stiffness due to the collagen
fibers being stretched. The final region is the
point at which the ultimate strength has been
reached, when the ligament is no longer able
to sustain a given force and consequently ruptures. The structural properties of a ligament
can be derived from the force–deformation
curve. The linear stiffness is the slope of the linear portion of the curve; stiffness is an extensive material property, meaning that it depends
both on the material being measured and its size
or boundary conditions. The material’s ultimate
strength and ultimate elongation are the determined at the point of rupture, and the energy to
failure is the area under the curve prior to failure. Force–deformation curves can also be used
to determine attachment site behavior as part of
the structure.
Stress (MPa)
VetBooks.ir
16
10
0
10
20
30
Strain
40
50
Figure 2.4 Typical stress–strain curve for ligament
during uniaxial tensile testing. A stress–strain curve is
determined by calculating the amount of strain
(deformation) that occurs as a result of varying levels of
tensile (or compressive) loading. The slope of the linear
aspect of the stress–strain curve defines Young’s modulus.
A material’s yield point occurs once the material begins
to plastically deform prior to rupture. The point of rupture
is where the ultimate stress and ultimate strain are
defined.
Viscoelasticity
Ligament, like all soft collagenous connective
tissues, is considered a viscoelastic material, in
that it exhibits both viscous and elastic properties when undergoing deformation, and, therefore, has time-dependent mechanical behavior. Two characteristic material properties that
are exhibited by viscoelastic materials are creep
and relaxation. Creep describes how a ligament
continues to stretch under a sustained force,
while relaxation describes how the tensile force
required to keep a stretched ligament at a constant length diminishes over time. As a consequence of relaxation, the stiffness of a viscoelastic material depends on the rate at which
load is applied. For a fast rate of loading, the
viscoelastic CrCL will be stiffer than if it is
stretched slowly. Another viscoelastic property
is hysteresis or energy dissipation. Ligaments
exhibit hysteresis during loading, which can
be seen when a ligament is loaded and then
unloaded, as the loading and unloading stress–
strain curves do not follow the same path. This
is due to a loss of energy that occurs during loading. However, during repetitive loading
VetBooks.ir
Biomechanics of the Cruciate Ligaments
and unloading, stress–strain curves eventually
synchronize, which underscores the importance
for pre-conditioning before experimental ligament biomechanical testing.
Biologic factors
There are a number of non-disease-related factors that affect ligament biomechanical properties, including age, body weight, phenotype, whether animals are gonadectomized,
and use/disuse (Laros et al. 1971; Vasseur et al.
1985; Duval et al. 1999).
In dogs, the effect of age on CrCL mechanical properties has been of particular interest.
Skeletal maturity has been shown to increase
strength, stiffness and other mechanical properties of ligaments. In a rabbit model, stiffness and
ultimate strength dramatically increase from 6
to 12 months of age, followed by insignificant
changes from 1 to 4 years of age (Woo et al.
1990). However, significant weakening occurs
in the CrCL with age. Decreases in modulus,
ultimate stress and strain energy density have
been reported, particularly in dogs weighing
more than 15 kg (Vasseur et al. 1985).
It is recognized that excessive body condition is a risk factor for cruciate ligament rupture (see also Chapter 14). Specific breeds of
dog are also at increased risk, such as the Newfoundland, Labrador Retriever, and Rottweiler,
while others, such as the Greyhound, are relatively protected from the condition (Whitehair
et al. 1993; Duval et al. 1999), suggesting a
genetic component to disease predisposition
(Baird et al. 2014). Additionally, histologic,
metabolic, anatomic and immune cell populations have also been considered possible risk
factors (Wingfield et al. 2000; Comerford et al.
2005; Comerford et al. 2006; Muir et al. 2007;
Ragetly et al. 2011). Neutering of either gender
has been reported to increase the prevalence of
CrCL rupture (Slauterbeck et al. 2004), although
recent studies have reported conflicting results
regarding both neuter status and gender predisposition (Adams et al. 2011; Grierson et al. 2011)
(see also Chapter 14).
As is seen with bone, immobilization results
in significant decreases in ligament strength. A
study using a 9-week rabbit stifle immobilization model showed that CrCL cross-sectional
17
area is significantly decreased and ultimate
strain significantly increased with immobilization, although decreases in modulus were not
significant, and no changes in ultimate stress
were found (Newton et al. 1995). Pelvic limb
disuse also results in impaired ligament healing; the CrCL of male rats that underwent
hindlimb suspension for 3 weeks had significantly decreased ultimate strength, ultimate
stress, and elastic modulus versus controls
(Provenzano et al. 2003). Relatively few studies have been performed studying the biomechanical effects of remobilization on previously
immobilized ligament, but over time material
properties appear to be restored before structural properties (Woo et al. 1987).
Sites of ligament rupture
In human beings and dogs, most CrCL/anterior
cruciate ligament (ACL) ruptures occur through
the body of the ligament. Similar to CrCL rupture in dogs, most ACL ruptures in human
beings occur via a non-contact mechanism
(Cimino et al. 2010). More recent evidence has
also suggested genetic predisposition for disease development (Rahim et al. 2014; StepienSlodkowska et al. 2016; Svoboda et al. 2016).
It has been shown in dogs with normal stifles
that tensile tests of the femur–CrCL–tibia complex result in avulsion factures of the CrCL tibial attachment site, as opposed to tears through
the CrCL body (Klein et al. 1982). This suggests that the mechanism resulting in CrCL rupture in the majority of dogs is due to a pathologic process that results in the degradation of
CrCL material properties. Much work has been
focused on the specific histologic changes that
occur in ligaments that have ruptured, such
as the development of chondroid transformation of ligament fibroblasts, alterations to collagen structure, changes in collagen fiber crimp,
and loss of ligament fibroblasts. However, the
cause and timeline of these changes and how
they relate to the progression of the cruciate ligament rupture condition and development of
CrCL rupture remains unclear (Vasseur et al.
1985; Narama et al. 1996; Hayashi et al. 2003).
It should be noted that avulsion fractures do
occur clinically in dogs, particularly immature
dogs. Such fractures are typically associated
VetBooks.ir
18
Structure and Function
with obvious trauma and present with an acute
onset of severe lameness (Reinke 1982).
Synovitis and ligament biomechanics
The development of synovitis and joint degradation has been clearly associated with CrCL
transection models that create joint instability
(Lipowitz et al. 1985). A relationship between
synovitis and joint instability in the canine cruciate rupture arthropathy has been well established over the past decade (see also Chapter 12). One of the initial studies examining
the effect of synovitis on ligament biomechanics was in a rabbit model, wherein the presence
of chronic synovitis significantly decreased ligament strength. Histologically, these ligaments
showed a loss of normal fiber orientation, a disorganized cellular pattern, changes in the interstitial matrix, and some infiltration of inflammatory cells within the ligament body (Goldberg
et al. 1982). This work has led to the hypothesis
that synovitis precedes cruciate ligament rupture in affected dogs, fitting with the clinical
observation that mid-body CrCL ruptures are
typical.
Another landmark study in this field evaluated Wistar rats that are predisposed to spontaneous synovitis. In these animals, a correlation was found between stifle synovitis and
chondroid metaplasia of the cruciate ligaments;
these changes were not age-related (Sasaki et al.
1998). Taken together, these data support the
hypothesis that stifle synovitis is a key factor
promoting joint degradation and diminished
ligament strength in dogs with cruciate ligament rupture. Numerous studies undertaken
over the past decade, focused on understanding
the pathologic basis of canine cruciate ligament
rupture, have resulted in a body of work supporting the hypothesis that osteoarthritis and
progressive cruciate ligament fiber rupture is
influenced by stifle synovitis (Muir et al. 2007;
Erne et al. 2009; Muir et al. 2011; Chuang et al.
2014; Little et al. 2014). Further work to understand the effects of synovitis on ligament structural properties is warranted.
Isometric points
With finite-sized areas of CrCL attachment, it
is not possible for all CrCL fibers to be isomet-
ric throughout flexion, and thus the CM and
CL bundles have differing biomechanical properties. Surgical protocols, however, require the
most isometric points to be used for joint stabilization or ligament reconstruction. Stabilization of the cruciate-deficient canine stifle occurs
primarily through either intra-articular or extracapsular techniques. Extracapsular stabilization
methods are still commonly employed today.
The general concept of these methods are to
align a suture outside the stifle joint capsule in
the direction of the previously existing CrCL.
Biomechanically speaking, the placement of
such a suture should not be considered so simplistically. Ideally, sutures should be placed in
an isometric manner, which means that during motion the suture attachment sites should
remain a constant distance apart, thus preventing laxity of the suture material and consequent cranial translation of the joint. Numerous studies have sought to identify isometric
points (Guénégo et al. 2007; Roe et al. 2008;
Hulse et al. 2010). It is important to note that
while these techniques attempt to use isometric points, such points do not exist biomechanically in the extracapsular space of the canine
stifle.
Biomechanics of grafts
The use of intra-articular grafts for the restoration of joint stability has been well established
in human orthopaedics. However, in dogs with
cruciate ligament rupture the use of grafts in
CrCL-deficient stifles has fallen out of favor
in the clinical setting. Various allografts, autografts, and synthetic materials have been tested
in experimental animals, but none has shown to
be mechanically equivalent to an intact CrCL.
One challenge of using grafts to replace CrCLs
in dogs is the lack of strength they display over
time (Cabaud et al. 1980; Shino et al. 1984; Curtis
et al. 1985; Vasseur et al. 1985; McFarland et al.
1986; van Rens et al. 1986; Yoshiya et al. 1986;
Johnson et al. 1989; Thorson et al. 1989). Unlike
experimental dogs used in these studies, clientowned dogs affected with cruciate ligament
rupture typically exhibit moderate to severe
synovitis at the time of surgical treatment.
Therefore, without a disease-modifying treatment, the use of grafts in these patients would
be even less likely to provide long-term stifle
VetBooks.ir
Biomechanics of the Cruciate Ligaments
stability compared to experimental dogs, as stifle inflammation will promote graft resorption.
Conclusions
The biomechanical properties of the cruciate ligaments are essential for stifle joint stabilization.
It is the degradation of these properties that
ultimately leads to cruciate ligament rupture
and loss of joint stability. Further understanding of the relationship between synovitis,
ligament degradation and ligament biomechanical properties is needed, as is development of
disease-modifying treatments to combat the
inflammatory joint environment associated
with cruciate ligament rupture in the dog.
Although progress has been made, the continued lack of understanding regarding the mechanisms involved in the development of cruciate
ligament rupture in affected dogs, particularly
with regard to synovitis, remains a barrier to
the development of better surgical treatments.
References
Adams P, Bolus R, Middleton S, et al. Influence of signalment on developing cranial cruciate rupture in
dogs in the UK. J Small Anim Pract 2011;52:347–
352.
Baird AE, Carter SD, Innes JF, et al. Genetic basis of
cranial cruciate ligament rupture in dogs. Connect
Tissue Res 2014;55:275–281.
Cabaud EH, Feagin JA, Rodkey WG. Acute anterior cruciate ligament injury and augmented repair.
Am J Sports Med 1980;8:395–401.
Chuang C, Ramaker MA, Kaur S, et al. Radiographic
risk factors for contralateral rupture in dogs with
unilateral cranial cruciate ligament rupture. PLoS
One 2014;9:e106389.
Cherdchutham W, Becker CK, Spek ER, et al. Effects
of exercise on the diameter of collagen fibrils in the
central core and periphery of the superficial digital
flexor tension in foals. Am J Vet Res 2001;62:1563–
1570.
Cimino F, Volk BS, Setter D. Anterior cruciate ligament injury: diagnosis, management, and prevention. Am Fam Physician 2010;82:917–922.
Comerford EJ, Tarlton JF, Innes JF, et al. Metabolism
and composition of the canine anterior cruciate ligament relate to differences in knee joint mechanics
and predisposition to ligament rupture. J Orthop
Res 2005;23:61–66.
Comerford EJ, Tarlton JF, Wales A, et al. Ultrasound
differences in cranial cruciate ligaments from dogs
of two breeds with a differing predisposition to
19
ligament degeneration and rupture. J Comp Path
2006;134:8–16.
Curtis RJ, Delee JC, Drez DJ. Reconstruction of the
anterior cruciate ligament with freeze-dried fascia
lata allografts in dogs. Am J Sports Med 1985;13:
408–414.
Duval JM, Budsberg SC, Flo GL, et al. Breed, sex and
body weight as risk factors for rupture of the cranial cruciate ligament in young dogs. J Am Vet Med
Assoc 1999;215:811–814.
Erne JB, Goring RL, Kennedy FA, et al. Prevalence
of lymphoplasmacytic synovitis in dogs with naturally occurring cranial cruciate ligament rupture.
J Am Vet Med Assoc 2009;235:386–390.
Goldberg VM, Burstein A, Dawson M. The influence
of an experimental immune synovitis on the failure
mode and strength of the rabbit anterior cruciate
ligament. J Bone Joint Surg 1982;64A:900–906.
Grierson J, Asher L, Grainger K. An investigation into
risk factors for bilateral canine cruciate ligament
rupture. Vet Comp Orthop Traumatol 2011;24:192–
196.
Guénégo L, Zahra A, Madelénat A, et al. Cranial cruciate ligament rupture in large and giant dogs. A
retrospective evaluation of a modified lateral extracapuslar stabilization. Vet Comp Orthop Traumatol
2007;20:43–50.
Hayashi K, Frank JD, Dubinsky C, et al. Histologic
changes in ruptured canine cranial cruciate ligament. Vet Surg 2003;32:269–277.
Hulse D, Hyman W, Beale B, et al. Determination of
isometric points for placement of a lateral suture in
treatment of the cranial cruciate ligament deficient
stifle. Vet Comp Orthop Traumatol 2010;23:163–
167.
Johnson SG, Hulse DA, Hogan HA, et al. System
behavior of commonly used cranial cruciate ligament reconstruction autographs. Vet Surg 1989;18:
459–465.
Klein L, Player JS, Heiple KG, et al. Isotopic evidence
for resorption of soft tissues and bone in immobilized dogs. J Bone Joint Surg Am 1982;64:225–
230.
Laros GS, Tipton CM, Cooper RR. Influence of physical activity on the ligament insertions in the knees
of dogs. J Bone Joint Surg Am 1971;53:275–285.
Lipowitz AJ, Wong PL, Stevens JB. Synovial membrane changes after experimental transection of the
cranial cruciate ligament in dogs. Am J Vet Res
1985;46:1166–1170.
Little JP, Bleedorn JA, Sutherland BJ, et al. Arthroscopic assessment of stifle synovitis in dogs with
cranial cruciate ligament rupture. PLoS One 2014;9:
e97329.
McFarland EG, Morrey BF, An KN, et al. The relationship of vascularity and water content to tensile strength in a patellar tendon replacement of the
anterior cruciate in dogs. Am J Sports Med 1986;14:
436–448.
Muir P, Schaefer SL, Manley PA, et al. Expression of
immune response genes in the stifle joint of dogs
VetBooks.ir
20
Structure and Function
with oligoarthritis and degenerative cranial cruciate ligament rupture. Vet Immunol Immunopathol
2007;119:214–221.
Muir P, Kelly JL, Marvel SJ, et al. Lymphocyte populations in joint tissues from dogs with inflammatory
stifle arthritis and associated degenerative cranial
cruciate ligament rupture. Vet Surg 2011;40:753–
761.
Narama I, Masuoka-Nishiyama M, Matsuura T, et al.
Morphogenesis of degenerative changes predisposing dogs to rupture of the cranial cruciate ligament. J Vet Med Sci 1996;58:1091–1097.
Newton PO, Woo SL, MacKenna DA, et al. Immobilization of the knee joint alters the mechanical and
ultrastructural properties of the rabbit anterior cruciate ligament. J Orthop Res 1995;13:191–200.
Ottani V, Raspanti M, Ruggeri A. Collagen structure
and functional implications. Micron 2001;32:251–
260.
Provenzano PP, Martinez DA, Grindeland RE, et al.
Hindlimb unloading alters ligament healing.
J Appl Physiol 2003;94:314–324.
Ragetly CA, Evans R, Mostafa AA, et al. Multivariate
analysis of morphometric characteristics to evaluate risk factors for cranial cruciate ligament deficiency in Labrador retrievers. Vet Surg 2011;40:327–
333.
Rahim M, Gibbon A, Hobbs H, et al. The association of
genes involved in the angiogenesis-associated signaling pathway with risk of anterior cruciate ligament rupture. J Orthop Res 2014;32:1612–1618.
Reinke JD. Cruciate ligament avulsion injury in the
dog. J Am Hosp Assoc 1982;18:257–264.
Roe SC, Kue J, Gemma J. Isometry of potential suture
attachment sites for the cranial cruciate ligament
deficient canine stifle. Vet Comp Orthop Traumatol
2008;21:215–220.
Sasaki S, Nagai H, Mori I, et al. Spontaneous synovitis
in Wistar Rats. Toxicol Pathol 1998;26:687–690.
Shino K, Kawasaki T, Hirose H, et al. Replacement of
the anterior cruciate ligament by an allogeneic tendon graft. J Bone Joint Surg Br 1984;66:672–681.
Slauterbeck JR, Pankratz K, Xu KT, et al. Canine
ovariohysterectomy and orchiectomy increases the
prevalence of ACL injury. Clin Orthop Relat Res
2004;429:301–305.
Stepien-Slodkowska M, Ficek K, Zeitek P, et al.
Whether the combination of COL1A1 gene polymorphisms may be a marker of the risk of injury?
J Sport Rehabil 2016; [Epub ahead of print].
Svodoba SJ, Owens BD, Harvey TM, et al. The
association between serum anterior biomarkers of
collagen turnover and subsequent cruciate ligament rupture. Am J Sports Med 2016;44:1687–
1693.
Thorson E, Rodrigo JJ, Vasseur P, et al. Replacement
of the anterior cruciate ligament. A comparison
of autografts and allografts in dogs. Acta Orthop
Scand 1989;60:555–560.
van Rens TJ, van den Berg AF, Huiskes R, et al.
Substitution of the anterior cruciate ligament: A
long-term histologic and biomechanical study with
autogenous pedicled grafts of the iliotibial band in
dogs. Arthroscopy 1986;2:139–154.
Vasseur PB, Pool RR, Arnoczky SP, et al. Correlative
biomechanical and histologic study of the cranial
cruciate ligament in dogs. Am J Vet Res 1985;46:
1842–1854.
Whitehair JG, Vasseur PB, Willits NH. Epidemiology
of cranial cruciate ligament rupture in dogs. J Am
Vet Med Assoc 1993;203:1016–1019.
Wingfield C, Amis AA, Stead AC, et al. Comparison of
the biomechanical properties of Rottweiler and racing greyhound cranial cruciate ligaments. J Small
Anim Pract 2000;41:303–307.
Woo SL, Ohland KJ, Weiss JA. Aging and sex-related
changes in the biomechanical properties of the rabbit medial collateral ligament. Mech Ageing Dev
1990;56:129–142.
Woo SL, Gomez MA, Sites TJ, et al. The biomechanical and morphological changes in the medial collateral ligament of the rabbit after immobilization and
remobilization. J Bone Joint Surg Am 1987;69:1200–
1211.
Yoshiya S, Andrish JT, Manley MT, et al. Augmentation of anterior cruciate ligament reconstruction
in dogs with prostheses of different stiffnesses.
J Orthop Res 1986;4:475–485.
VetBooks.ir
3
Cruciate Ligament Remodeling
and Repair
Connie S. Chamberlain, Erin E. Crowley, and Ray Vanderby Jr.
Introduction
Multiple factors adversely affect the healing
capacity of the cranial cruciate ligament (CrCL),
including complex ligament anatomy, biomechanical forces, nutritional delivery, as well as
the biologic milieu. These factors prevent a ruptured CrCL from regenerating its native tissue
or recapitulating mechanical function. With little intrinsic healing potential, ruptures of the
CrCL are often reconstructed. The repair process may extend from months to years and
the injured ligament or replacement graft never
fully recovers the original mechanical properties (Levenson et al. 1965; Lin et al. 2004). CrCL
grafts usually lengthen, and their initial tissue strength can drop by approximately 50%
after remodeling (Feagin & Curl 1976; Sherman & Bonamo 1988; Kaplan et al. 1990). Reconstructed stifles are often less stable and fail to
restore normal joint kinematics. These deficiencies contribute to premature joint degeneration,
osteoarthritis, and compromised function. This
chapter will briefly discuss the biologic processes for natural CrCL healing, as well as the
biological steps occurring during the healing of
a reconstructed CrCL graft.
Healing potential of the
extracapsular ligament
For comparison, consider healing of an extracapsular ligament (e.g., a medial collateral
ligament, MCL; Figure 3.1). A robust healing
cascade occurs consisting of hemostasis and
inflammation, proliferation, and remodeling
(Frank et al. 1983; Clark 1985; Clark 1993; Chamberlain et al. 2009). Hemostasis and inflammation immediately follow injury, and are
characterized by the formation of a hematoma
organized into a fibrinogen mesh and the
accumulation of neutrophils, monocytes/
macrophages, and T-lymphocytes (Chamberlain et al. 2009). These inflammatory cells
rid injured tissue of debris, and secrete
cytokines and growth factors that modulate inflammation, attract fibroblasts to the
injury, and stimulate subsequent activities in
the healing cascade. The proliferative phase
follows the inflammatory stage, and consists
of increased fibroblasts, myofibroblasts, additional macrophages, and endothelial cells
(Chamberlain et al. 2009). These cells and their
products form granulation tissue within the
injured region. Remodeling is the final phase
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
21
Structure and Function
VetBooks.ir
22
Remodeling
Proliferation
Decorin (↓↓)
Hemostasis
Inflammation
Type I Collagen (↓↓)
Type I Collagen (↓↓)
Type III Collagen
Relative Level
Fibromodulin
Total Cells
VEGF
Neutrophils
Apoptosis
Apoptosis
Hematopoietic Cells
Myofibroblasts
Mitotic Cells
Macrophages
Largest Wound Region
Angiogenesis
T-Lymphocytes
MCL Edema
Injury
1
3
5
7
9
11
14
21
28
Days Post-Injury
Figure 3.1 Process of normal, extracapsular healing by the rat medial collateral ligament. Healing involves three
complex and overlapping processes, including hemostasis and inflammation, proliferation, and remodeling. Hemostasis
and inflammation involves clot formation and the infiltration of inflammatory cells, such as neutrophils, macrophages
and T lymphocytes, immediately after injury. Proliferation is characterized by the formation of granulation tissue,
including fibroblast proliferation and angiogenesis. Remodeling is the final phase and involves cell number reduction
and scar formation. Source: Chamberlain et al. 2009. Reproduced with permission from John Wiley & Sons, Inc.
of healing and follows proliferation. The earlier
infiltration of fibroblasts, inflammatory cells,
and endothelial cells diminish to basal levels
during this stage (Chamberlain et al. 2009). This
phase of healing lasts many months in ligaments and results in scar-like neo-ligamentous
tissue that can still be found two years post
injury (Frank et al. 1983). The cellular profile of
the remodeling ligament is somewhat similar
to uninjured tissue compared to the previous
inflammatory or proliferative phases, but
complete functional recovery may never occur.
With or without surgical intervention, the
injured MCL will heal, but it results in tissue
that is more scar-like than the native tissue and
is mechanically inferior.
Healing potential of the completely
ruptured CrCL
Unlike the extracapsular MCL, the intracapsular CrCL does not heal without early surgical
intervention. A native CrCL is a highly organized, dense connective tissue composed of
dense parallel collagen bundles, exhibiting birefringence and crimping under polarized light
(Hayashi et al. 2003a). Small blood vessels and
fusiform- and ovoid-shaped fibroblasts surround the collagen bundles. A synovial membrane surrounds the CrCL and consists of dense
connective tissue, small fibroblasts, and some
adipocytes (Heffron & Campbell 1978; Hayashi
et al. 2003a). Healing phases are summarized
VetBooks.ir
Cruciate Ligament Remodeling and Repair
23
Table 3.1 Healing response over the course of 10 weeks by the CrCL after complete or partial rupture, or surgical repair.
Time post injury
Complete rupture
Partial rupture
Immediately
No hematoma
Possible hematoma
1 week
Necrosis
Inflammation
Necrosis
Inflammation
Provisional matrix
Fibroblast proliferation throughout
Inflammation
Provisional matrix
2 weeks
Edema
Ligament retraction
Fibroblast proliferation
of ends
Necrosis
No granulation tissue formation
Fibroblast proliferation throughout
ligament
Proliferation
Granulation tissue
4 weeks
Collagen formation
Ligament resorption
No granulation tissue formation
Fibroblast proliferation throughout
ligament
Collagen formation
Fibroblast proliferation
Collagen formation
6 weeks
Collagen formation
Ligament resorption
Fibroblast proliferation
Collagen formation
8 weeks
Collagen formation
Ligament resorption
Fibroblast proliferation
Collagen formation
10 weeks
Collagen formation
Ligament resorption
in Table 3.1. Immediately after complete CrCL
rupture the synovial joint fluid bathes the ligament, and prevents clot formation and union
of the ligament ends (O’Donoghue et al. 1966).
The lack of hematoma precludes the formation
of a provisional matrix and granulation tissue
to start the healing process. One week after
rupture, the CrCL undergoes necrosis and
inflammatory cell infiltration; B and T lymphocytes, macrophages, dendritic cells, and IgG,
IgM, and IgA plasma cells infiltrate the inflamed
synovium (O’Donoghue et al. 1966; Lemburg
et al. 2004). The extracellular matrix (ECM)
collagenous structure is partially lost or disorganized, lacks birefringence, and exhibits little
or no crimp (Hayashi et al. 2003b). At 2 weeks
the CrCL becomes edematous, the injured ends
retract, and fibroblasts proliferate and accumulate near the ruptured ends and decrease within
the inner ligament (O’Donoghue et al. 1966;
Hayashi et al. 2003b). Atypical spheroid-shaped
fibroblasts appear with the typical fusiformand ovoid-shaped fibroblasts (Hayashi et al.
2003b). Surviving centralized spheroid fibroblasts undergo chondroid transformation
and become devitalized as a result of inadequate blood flow, tissue hypoxia, and oxidative
Surgical repair
Collagen formation
stress (Hayashi et al. 2003a,b). A diminished blood supply to the ruptured ligament
also results in resorption of the ligament
(O’Donoghue et al. 1966). Occasionally, the
ruptured CrCL will fuse to the caudal cruciate
ligament and maintain vascularity. Similar to a
partial CrCL rupture, contact to a blood supply
limits necrosis. By 8 weeks, the remaining CrCL
segment shortens, precluding the possibility of
suturing the ends together (O’Donoghue et al.
1966). Similar to the rabbit, after 3–12 months
very few remnants of ligament exist and stifles
show signs of osteoarthritis, with cartilaginous
damage localizing primarily at the femoral
condyle (Hefti et al. 1991).
Healing potential of the partially
ruptured CrCL
The partially torn CrCL initially exhibits a
weak healing response (Table 3.1). Partial CrCL
ruptures form a hematoma and produce an
organized fibrin meshwork to promote an early
inflammatory response (Hefti et al. 1991). At 1
week post injury the ligaments remain intact,
and a gelatinous provisional matrix fills the
VetBooks.ir
24
Structure and Function
gap (O’Donoghue et al. 1966). Between 2 and
4 weeks, proliferating fibroblasts infiltrate the
entire ligament, but the formation of granulation tissue is delayed (O’Donoghue et al. 1966).
Fibroblast proliferation continues throughout
the ligament, and the partially torn CrCL develops longitudinally oriented collagen fibers in
the defect by 10 weeks (O’Donoghue et al. 1966).
Although partial ruptures form a hematoma
and provisional matrix (unlike complete ruptures), the partial defect remains incompletely
filled and therefore functionally deficient.
Healing potential of the surgically
repaired CrCL
Surgical repair of the CrCL via suturing the ligament ends together immediately after injury
can provide some degree of healing (Table 3.1).
Similar to the extracapsular MCL, the sutured
CrCL undergoes inflammation, proliferation
and remodeling, albeit a slower process. Granulation tissue forms in the sutured region, the
inflammatory response progressively subsides,
and the region of scar formation stabilizes. At
1 and 2 weeks post surgery the ligament forms
a provisional matrix consisting of inflammatory cells (O’Donoghue et al. 1966). By week
4, fibroblast proliferation and collagen formation increases within the defect (O’Donoghue
et al. 1966). Between 6–10 weeks, the newly
formed collagen within the defect blends with
the intact portion of the CrCL. However, the
tensile strength of the ligament remains substantially weaker than that of the uninjured
CrCL (O’Donoghue et al. 1966). This promising healing outcome is found when the surgically repaired ligament was initially transected.
A typical injury results in frayed ends, which
complicates successful closure of the ligament
ends. Additionally, if the repair is not completed immediately after rupture the ligament
ends undergo necrosis and resorption, thereby
inhibiting successful surgical intervention.
Healing potential of the reconstructed
CrCL graft
Rupture of the CrCL often involves reconstruction with an autograft or allograft due to the
poor functional outcomes with non-operative
treatment. In a process that is slower and less
efficient than MCL healing, a CrCL graft undergoes a complex healing process which includes
synovialization, avascular necrosis, revascularization, cellular proliferation, and remodeling.
At the time of transplantation, the central core
of the graft is avascular. After transplantation, a
synovial layer forms around the graft, providing a blood supply to the transplanted tissue.
The inner core remains avascular and acellular
for up to 3 months post surgery, but the peripheral graft repopulates with fibroblasts. The lack
of vascularity and cellularity within the ligament core results in central graft necrosis, leading to collagen destruction. Eventually, vascular buds originating from the infrapatellar fat
pad and synovial tissue form within the graft.
The vessels progress from the epiligament to the
central portion of the graft, and by 4–6 months
the specimens typically revascularize. Vascularization helps to transport inflammatory cells
and supply nutrients to the healing tissue; infiltrating vessels also contribute to cellular repopulation of the graft. Avascular necrosis may be
limited or prevented if using vascularized autografts or grafts with preserved peritendinous
connective tissue (Lambert 1983; van Rens et al.
1986; Butler 1989; Butler et al. 1989; Sckell et al.
1999).
Cell proliferation follows revascularization
of the ligament graft. A limited proliferation
of intrinsic graft tendon cells occurs, even
without a peritendinous connective tissue or
vascularized graft. However, allografts need
further processing (e.g., deep freezing, etc.)
to eradicate the intrinsic cells. Fresh allografts
cause a severe inflammatory reaction and
rejection response, implying some degree of
intrinsic cellular influence after grafting. Proliferating cells, including fibroblasts, neutrophils,
circulating M1 and resident M2 macrophages,
initially appear within the bone–tendon interface (Kawamura et al. 2005). Circulating M1
macrophages remain in the bloodstream until
the initiation of an immune response. After
injury, cells travel to the compromised site and
promote inflammation, resulting in phagocytosis and tissue destruction. In contrast, the
resident M2 macrophages are intrinsic cells that
reduce inflammation and stimulate healing.
With time, cell proliferation progresses from
the interface to the outer and inner tendon
VetBooks.ir
Cruciate Ligament Remodeling and Repair
(A)
Week 1
(B)
Week 7
Figure 3.2 Macrophage localization within the
reconstructed cranial cruciate ligament (CrCL).
Immunohistochemistry of the circulating M1
macrophages within a reconstructed rat CrCL at 1 week
(A) and 7 weeks (B) after transplantation. Similar to the
canine reconstructed CrCL, few macrophages localize to
the graft at week 1 after injury. As time progresses, more
cells infiltrate the ligament. Original magnification, ×600.
(Figure 3.2). Neutrophils and macrophages,
derived from the bone marrow or synovial
membrane, accumulate within the outer graft
by day 4 (Kawamura et al. 2005). Proliferating
cells and M1 and M2 macrophages continue to
progress into the inner tendon and are evident
by 14 days post-transplantation (Kawamura
et al. 2005). Few to no neutrophils or T lymphocytes localize to the inner graft (Kawamura et al.
2005). Evidence suggests that the macrophages
differentiate into a fibroblast phenotype to
synthesize collagen (Vaage & Lindblad 1990).
During remodeling, the graft undergoes ligamentization, with characteristic restructuring
of the graft towards the properties of the intact
CrCL (Amiel et al. 1984; Amiel et al. 1986;
25
Murray et al. 2000; Marumo et al. 2005). Collagen fibers regain organization, which resembles the appearance of the intact CrCL. However, the initial loss of collagen crimp, size of
collagen fibrils, and parallel alignment is only
partially restored (Liu et al. 1995; Scheffler et al.
2008). Additionally, the graft remains mechanically inferior when compared to the uninjured
tissue. Grafts initially pull from the osseous tunnel. A study in sheep showed that load to failure
of the reconstructed graft averaged 5% of the
normal ligament at 3 weeks (graft 37.8 ± 17.8 N
versus intact 759.2 ± 114.1 N), and typically
fails in the intra-articular portion (Meller et al.
2008). Graft load to failure improved to 15%
of the normal ligament by 6 weeks, and exhibited a decline in grip-to-grip elongation (Meller
et al. 2008). By 12 and 24 weeks, the strength
of the graft had improved to 41% and 69% of
the normal ligament, respectively, but the graft
strength remained far less than the normal CrCL
at even 52 weeks after transplantation (Meller
et al. 2008).
Healing potential of the reconstructed
graft interface tissue
CrCL reconstruction requires healing of the
tendon graft and bone tunnels in the femur
and tibia. Repair of the CrCL proceeds via
the formation of a fibrovascular interface tissue (Figure 3.3) between the graft and bone,
bone in-growth into the graft–bone interface,
and the progression of collagen fiber continuity
between tendon and bone to result in a reestablished tendo-osseous junction (Rodeo et al. 1993;
Rodeo et al. 1999). After CrCL reconstruction,
the graft and original cancellous bone fills with
fibroblast-deposited fibrovascular interface tissue (Figure 3.4). Inflammatory cells and type
III collagen initially accumulate in the interface granulation tissue. A few neutrophils and
T lymphocytes are found within the granulation tissue the first week after surgery (Kawamura et al. 2005). After the neutrophil numbers
have decreased, M1 macrophages, followed by
M2 macrophages, appear. While the inflammatory cells infiltrate the granulation tissue, new
bone also permeates the interface. Chondroid
cells then appear from the side of the bone
tunnel and degrade the granulation tissue and
2.0
2.5
3.0
5
3
Weeks Post-Repair
Inflammation
7
0
0.5
Figure 3.3 H&E staining of the rat reconstructed cranial cruciate ligament graft at 1 week and 7 weeks after surgery. Similar to the dog at 1 week (A) and 2 weeks (B) after
repair, the graft exhibits little cellularity, whereas the interface is cellularly active and inflamed. The graft displays more disorganization and cellularity by 3 weeks, whereas
the interface becomes less inflamed (C). By 5 weeks, the graft organization is improving while the cell infiltration remains similar to that after 3 weeks (D). The 7-week
reconstructed CrCL shows reduced cell numbers, more organization, and smaller interface as the tendon remodels (E). (F) Graph summarizing graft tissue organization and
inflammation post reconstruction. B, bone; IF, interface; G, graft.
(F)
0
0.5
1.0
2
2.0
2.5
3.0
1.0
Organization
0 - None
1 - Mild
2 - Moderate
Inflammation
3 - Marked
1.5
1
Graft Organization
3 - Markedly Disorganized
2 - Moderately Disorganized
1 - Mildly Disorganized
0 - Organized
VetBooks.ir
Rank
1.5
Rank
26
Structure and Function
Figure 3.4 H&E and respective multiphoton microscopy images of the reconstructed CrCL graft. H&E (upper row) and multiphoton images (lower row) demonstrate an
inflamed and cellular interface tissue at weeks 1, 2, and 3 after repair. By weeks 5 and 7, the interface is less inflamed and less cellular. Yellow lines indicate the interface area.
VetBooks.ir
Cruciate Ligament Remodeling and Repair
27
VetBooks.ir
28
Structure and Function
deposit type II collagen. The granulation tissue is progressively replaced with maturing
lamellar bone. As healing progresses, numerous
cells consisting of osteoblasts and osteoclasts
scatter throughout the tunnel. Graft incorporation initiates at the fixation sites and progresses
towards the articular tunnel entrance, where
graft motion may impair early graft incorporation. At approximately 3–4 weeks after surgery,
an indirect graft insertion forms perpendicular collagen fibers resembling Sharpey’s fibers
(Gulotta & Rodeo 2007). The type III collagenpositive fibers are present 1 year after surgery,
and the number and size are associated with the
pull-out strength of the graft (Gulotta & Rodeo
2007).
Summary
Without surgical repair, the ruptured CrCL
cannot form a hematoma or subsequent granulation tissue, and the ligament eventually
degenerates. Healing of repaired tissue in
a synovial environment is incomplete and
functionally undesirable. Surgical reconstruction of the CrCL can improve outcome, but
launches a healing and remodeling cascade
that is slow and not functionally regenerative. Many factors modulate the ineffective
healing response between tendon and bone,
including the presence of inflammatory cells
in the graft, limited bone ingrowth into the
tendon graft, graft-tunnel motion, the paucity
of undifferentiated progenitor cells, and lack
of a coordinated signaling cascade towards
regenerative healing (Gulotta & Rodeo 2007).
Reconstruction of a CrCL using graft tissue
improves healing, but does not regenerate
native ligament tissue. The reconstructed CrCL
undergoes synovialization, avascular necrosis, vascularization, cellular proliferation and
remodeling, but this still results in a mechanically compromised tissue. The interface
between graft and bone likewise undergoes
a repair process involving development of a
fibrovascular interface, bone in-growth, and
collagen fiber continuity. Studies have quantified deficiencies in the healing and remodeling
processes in repaired or reconstructed CrCLs.
Recent advances to modulate the CrCL healing or graft-healing processes documented
above (advances such as tissue engineering,
targeted delivery of bioactive molecules,
platelet-rich plasma, or healing augmented
with mesenchymal stromal cells) provide
optimism for improved and accelerated mechanisms to repair or reconstruct the ruptured
CrCL (Linon et al. 2014; Proffen et al. 2015;
LaPrade et al. 2016).
References
Amiel D, Frank C, Harwood F, et al. Tendons and ligaments: a morphological and biochemical comparison. J Orthop Res 1984;1:257–265.
Amiel D, Kleiner JB, Roux RD, et al. The phenomenon of ‘ligamentization’: anterior cruciate ligament reconstruction with autogenous patellar tendon. J Orthop Res 1986;4:162–172.
Butler DL. Kappa Delta Award paper. Anterior cruciate ligament: its normal response and replacement.
J Orthop Res 1989;7:910–921.
Butler DL, Grood ES, Noyes FR, et al. Mechanical
properties of primate vascularized vs. nonvascularized patellar tendon grafts; changes over time.
J Orthop Res 1989;7:68–79.
Chamberlain CS, Crowley E, Vanderby R. The spatiotemporal dynamics of ligament healing. Wound
Repair Regen 2009;17:206–215.
Clark RA. Cutaneous tissue repair: basic biologic considerations. I. J Am Acad Dermatol 1985;13:701–
725.
Clark RA. Biology of dermal wound repair. Dermatol
Clin 1993;11:647–666.
Feagin JA, Jr, Curl WW. Isolated tear of the anterior cruciate ligament: 5-year follow-up study. Am
J Sports Med 1976;4:95–100.
Frank C, Schachar N, Dittrich D. Natural history of
healing in the repaired medial collateral ligament.
J Orthop Res 1983;1:179–188.
Gulotta LV, Rodeo SA. Biology of autograft and allograft healing in anterior cruciate ligament reconstruction. Clin Sports Med 2007;26:509–524.
Hayashi K, Frank JD, Dubinsky C, et al. Histologic
changes in ruptured canine cranial cruciate ligament. Vet Surg 2003a;32:269–277.
Hayashi K, Frank JD, Hao Z, et al. Evaluation of ligament fibroblast viability in ruptured cranial cruciate ligament of dogs. Am J Vet Res 2003b;64:1010–
1016.
Heffron LE, Campbell JR. Morphology, histology and
functional anatomy of the canine cranial cruciate
ligament. Vet Rec 1978;102:280–283.
Hefti FL, Kress A, Fasel J, et al. Healing of the transected anterior cruciate ligament in the rabbit. J
Bone Joint Surg 1991;73A:373–383.
Kaplan N, Wickiewicz TL, Warren RF. Primary
surgical treatment of anterior cruciate ligament
ruptures: a long-term follow-up study. Am J Sports
Med 1990;18:354–358.
VetBooks.ir
Cruciate Ligament Remodeling and Repair
Kawamura S, Ying L, Kim HJ, et al. Macrophages
accumulate in the early phase of tendon-bone healing. J Orthop Res 2005;23:1425–1432.
Lambert KL. Vascularized patellar tendon graft with
rigid internal fixation for anterior cruciate ligament
insufficiency. Clin Orthop Relat Res 1983;172:85–89.
LaPrade RF, Dragoo JL, Koh JL, et al. AAOS Research
Symposium Updates and Consensus: Biologic
Treatment of Orthopaedic Injuries. J Am Acad
Orthop Surg 2016;24:e62–e78.
Lemburg AK, Meyer-Lindenberg A, HewickerTrautwein M. Immunohistochemical characterization of inflammatory cell populations and adhesion
molecule expression in synovial membranes from
dogs with spontaneous cranial cruciate ligament
rupture. Vet Immunol Immunopathol 2004;97:231–
240.
Levenson SM, Geever EF, Crowley LV, et al. The Healing of Rat Skin Wounds. Ann Surg 1965;161: 293–
308.
Lin TW, Cardenas L, Soslowsky LJ. Biomechanics of
tendon injury and repair. J Biomech 2004;37:865–
877.
Linon E, Spreng D, Rytz U, et al. Engraftment of autologous bone marrow cells into the injured cranial
cruciate ligament in dogs. Vet J 2014;202:448–454.
Liu SH, Yang RS, al-Shaikh R, et al. Collagen in tendon, ligament, and bone healing. A current review.
Clin Orthop Rel Res 1995;318:265–278.
Marumo K, Saito M, Yamagishi T, et al. The ‘ligamentization’ process in human anterior cruciate
ligament reconstruction with autogenous patellar
and hamstring tendons: a biochemical study. Am J
Sports Med 2005;33:1166–1173.
Meller R, Willbold E, Hesse E, et al. Histologic and
biomechanical analysis of anterior cruciate ligament graft to bone healing in skeletally immature
sheep. Arthroscopy 2008;24:1221–1231.
29
Murray MM, Martin SD, Martin TL, et al. Histological changes in the human anterior cruciate ligament
after rupture. J Bone Joint Surg 2000;82A:1387–
1397.
O’Donoghue DH, Rockwood CA, Jr, Frank GR, et al.
Repair of the anterior cruciate ligament in dogs. J
Bone Joint Surg Am 1966;48:503–519.
Proffen BL, Perrone GS, Roberts G, et al. Bridgeenhanced ACL repair: A review of the science and
the pathway through FDA investigational device
approval. Ann Biomed Eng 2015;43:805–818.
Rodeo SA, Arnoczky SP, Torzilli PA, et al. Tendonhealing in a bone tunnel. A biomechanical and histological study in the dog. J Bone Joint Surg Am
1993;75:1795–1803.
Rodeo SA, Suzuki K, Deng XH, et al. Use of recombinant human bone morphogenetic protein-2 to
enhance tendon healing in a bone tunnel. Am J
Sports Med 1999;27:476–488.
Scheffler SU, Unterhauser FN, Weiler A. Graft
remodeling and ligamentization after cruciate ligament reconstruction. Knee Surg Sports Traumatol
Arthrosc 2008;16:834–842.
Sckell A, Leunig M, Fraitzl CR, et al. The connectivetissue envelope in revascularisation of patellar
tendon grafts. J Bone Joint Surg 1999;81B:915–
920.
Sherman MF, Bonamo JR. Primary repair of the anterior cruciate ligament. Clin Sports Med 1988;7:739–
750.
Vaage J, Lindblad WJ. Production of collagen type I
by mouse peritoneal macrophages. J Leukoc Biol
1990;48:274–280.
van Rens TJ, van den Berg AF, Huiskes R, et al. Substitution of the anterior cruciate ligament: a long-term
histologic and biomechanical study with autogenous pedicled grafts of the iliotibial band in dogs.
Arthroscopy 1986;2:139–154.
VetBooks.ir
VetBooks.ir
4
Meniscal Structure and Function
Antonio Pozzi and James L. Cook
Surgical anatomy
The menisci are crescent-shaped wedges of
fibrocartilage that rest on the peripheral aspects
of the articular surfaces of the proximal tibia.
They function to effectively deepen the medial
and lateral tibial fossae for articulation with the
condyles of the femur (Figure 4.1). They are
thickest abaxially and taper to thin, unattached
edges axially. The superior femoral surfaces are
slightly concave to accommodate the femoral
condyles, thus providing greater articular contact area and improved stifle joint congruity. In
dogs, the medial meniscus is larger than the lateral and more ovoid in shape. The lateral meniscus is smaller and more circular (Hulse & Shires
1983; Arnoczky 1993; Evans 1993; Carpenter &
Cooper 2000).
Both medial and lateral menisci have attachments that influence their mobility and function (Figure 4.2). The medial meniscus is firmly
attached to the tibia through cranial and caudal
menisco-tibial ligaments. Strong attachments
are also present between the abaxial aspect of
the medial meniscus and the medial collateral
ligament. The abaxial periphery of the medial
meniscus is also attached to the joint capsule
via short ligaments that blend with the joint
capsule (sometimes referred to as the coronal
ligaments). A cranial menisco-tibial ligament
anchors the lateral meniscus to the tibial plateau
caudo-lateral to the cranial cruciate ligament
(CrCL). Small caudal menisco-tibial ligament(s)
may or may not be present in dogs, and can be
attached cranial or caudal to the caudal cruciate ligament (CaCL) attachment when present.
The lateral meniscus differs from the medial
meniscus, however, in that the caudal pole of
the lateral meniscus is attached firmly to the
femur through the menisco-femoral ligament,
which attaches onto the caudo-medial aspect of
the intercondylar notch, caudal to the CaCL. In
addition, the abaxial border of the lateral meniscus lacks a firm attachment to the lateral collateral ligament or joint capsule, and instead forms
a groove where the popliteal tendon slides
between the meniscus and joint capsule during stifle motion. The resultant mobility of the
lateral meniscus helps to explain the decreased
incidence of severe lateral meniscal tears concurrent to CrCL insufficiency when compared
to the medial meniscus in dogs (Ralphs & Whitney 2002). The intermeniscal or transverse ligament connects the cranial poles of the lateral and medial menisci, and blends with fibers
from the cranial menisco-tibial ligaments. The
intermeniscal ligament lies just cranial to the
tibial attachment of the CrCL and is covered
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
31
Structure and Function
VetBooks.ir
32
Figure 4.1 Frontal plane image of an ex vivo specimen
showing the congruity provided by the menisci to the
femoral and tibial articulation. The wedge-shaped
menisci fill the space between the femoral and the tibial
condyles.
by the infrapatellar fat pad. A comprehensive
understanding of meniscal anatomy is integral
to understanding disease mechanisms, and for
avoiding iatrogenic damage to these important
structures during surgical treatment of stifle
disorders.
Structure and composition
The menisci consist of highly differentiated cells
of various phenotypes within an intricately
arranged extracellular matrix (ECM). Meniscal cells vary from fusiform, fibroblastic to
rounded, chondrocytic phenotypes, depending
on location. The morphological similarities of
these meniscal cells to those of other musculoskeletal tissues suggest specific functions in
connective tissue synthesis and maintenance
for each phenotype. For example, cells in the
periphery of menisci are similar to those in ligament and tendon, while cells in the central
region are similar to hyaline cartilage (Helio Le
Graverand et al. 2001). The ECM associated with
the cells in these different regions also mimics
the composition and function of the respective
tissues.
The ECM of menisci is composed primarily of
water, collagens, and proteoglycan aggregates
(Adams & Ho 1987; Stephan et al. 1998; Cook
et al. 1999; Noone et al. 2002). Although meniscal tissue contains several different molecular
types of collagen, type I collagen accounts for
about 90% of the total collagen present (Eyre &
Wu 1983). Other types of collagen are also
present and demonstrate regional differences.
For example, type I collagen is more abundant
in the periphery, while type II is predominant in
the axial third of the meniscus (Cheung 1987).
This arrangement is most likely related to the
specific biomechanical functions of each region
(Bullough et al. 1970). On the meniscal surfaces,
the collagen fibrils are randomly oriented and
form a mesh. Just beneath this layer the collagen bundles show a more irregular orientation.
Deep to these layers in the peripheral meniscus,
the collagen fibers are organized in large bundles, which are circumferentially arranged from
cranial to caudal attachments sites. Small radial
fibers, also called ‘tie fibers,’ are arranged across
the circumferential fibers and connect the abaxial region to the axial regions, where collagen
II fibers and proteoglycan predominate. The tie
fibers provide structural rigidity by resisting
the splitting force that arises from compressive
loading to the axial region and helping to transfer it to a radial load, which the circumferential
fibers can resist.
Several types of proteoglycan exist in the
meniscus. In the adult dog a relatively constant
distribution of 60% chondroitin-6-sulfate, 25%
chondroitin-4-sulfate, 10% chondroitin, and 5%
dermatan sulfate is found (Adams & Muir
1981). The distribution of the proteoglycan
depends on the region of the meniscus, the inner
third being approximately 8% proteoglycan and
the outer third only 2% proteoglycan.
Neurovascular anatomy
The menisci are relatively avascular. Both
menisci demonstrate a common pattern and
distribution of blood vessels that arise from
the medial and lateral genicular arteries
(Arnoczky & Warren 1983). Within the synovial
and capsular tissue of the stifle, an extensive
perimeniscal capillary plexus supplies the
peripheral border of the meniscus throughout
VetBooks.ir
Meniscal Structure and Function
(A)
33
Meniscal ligaments
Cranial and caudal
cruciate ligaments
Medial collateral
ligament
Coronal ligament
(C)
Patellar tendon
Cranial
cruciate
ligament
Transverse ligament
Cranial
menisco-tibial
ligament
Cranial
menisco-tibial
ligament
Medial
collateral
ligament
Lateral
collateral
ligament
Medial meniscus
Caudal
menisco-tibial
ligament
(B)
Lateral meniscus
Caudal menisco-tibial
ligament
Caudal
cruciate
ligament
Menisco-femoral
ligament
Figure 4.2 (A) Photograph of right tibial plateau illustrating the meniscal attachments and their relationship to the other
intra-articular structures. (B) Line drawing of the tibial plateau, showing the meniscal ligaments. (C) Line drawing of the
tibial plateau after removal of the menisci and the other structures, showing the footprints of the meniscal ligaments and
cruciate ligaments. Copyright © Samantha J. Elmhurst at www.livingart.org.uk.
its attachment to the joint capsule. These vessels
are limited to the peripheral 10% to 25% of the
meniscus. Synovial vessels are also found in
regions where there is no direct contact between
meniscus and cartilage (Arnoczky & Warren
1983). Although the peripheral portion of the
menisci is vascularized, most of the meniscus
is avascular and must rely to a large degree on
synovial sources of nutrition. Alternative mechanisms for nutrition are diffusion or mechanical
pumping of synovial fluid from compression
of the tissue during stifle motion (Arnoczky
et al. 1980). These regional differences have
profound implications for meniscal pathology
and treatment considerations (Figure 4.3).
The innervation of the meniscus is not as
well delineated as its blood supply. Nerve fibers
originating from the perimeniscal tissue radiate
into the peripheral third of the meniscus, and
are most dense in the cranial and caudal poles.
Structure and Function
VetBooks.ir
34
F
M
PCP
T
(A)
(B)
Figure 4.3 (A) Frontal plane section of the medial compartment of a dog’s stifle prepared with the Spalteholz
technique, showing the perimeniscal capillary plexus forming the red-red zone of the meniscus. Note that the red-red or
vascular zone is only about 25% of the radial width, which corresponds to about 2 mm-wide peripheral tissue. PCP,
perimeniscal capillary plexus; F, femur; M, avascular zone of the meniscus; T, tibia. (B) View of the entire medial
meniscus. The avascular axial margin of the medial meniscus is indicated (arrows). Sources: (A) Arnoczky & Warren
1983. Reproduced with permission from SAGE Publications. (B) Courtesy of Dr Steven Arnoczky.
Nerve fibers in the menisci appear to predominately serve propioceptive and mechanoreceptive roles, with little if any nociceptive function
recognized. Meniscal-derived sensory signals
during loading may contribute to protective
neuromuscular reflex control of joint motion.
Biomechanical and material properties
The meniscus demonstrates a complex set
of material properties that vary nonlinearly
with location (inhomogeneous) and direction
(anisotropic). These properties are important
for the biomechanical functions of the meniscus,
such as load transmission at the tibiofemoral
articulation, shock absorption, and stability.
These functions are important for normal homeostasis of the cartilage and the function of the
stifle. The tensile properties of meniscal tissue
are closely related to the collagen fiber architecture. Variations in tensile stiffness and strength
of meniscal tissue correspond to local differences in collagen ultrastructure and fiber bundle orientation.
In compression, the meniscal tissue should
be considered as a biphasic composite material
because of its composition of 75% water and
25% collagen and proteoglycan. During loading, most of the water is forced to flow through
the matrix to redistribute within the tissue or to
exude from the tissue. The high frictional drag
forces associated with water flow through the
porous-permeable solid matrix give rise to timedependent viscoelastic behaviors such as creep
and stress relaxation. The significance of the viscoelastic behavior of the meniscus is that when
the joint is loaded for long periods the contact area increases, thereby reducing the stress
per unit area of the tissue. The concentration of
VetBooks.ir
Meniscal Structure and Function
proteoglycans influences the viscoelastic behavior of the meniscus because their negative
charges counteract fluid flow.
The material properties of the meniscus are
also very important for its behavior in tension.
Variations in tensile stiffness and strength are
found in different regions, and relate to local
differences in collagen fiber ultrastructure and
fiber bundle orientation. Intact tie fibers are
also very important as they restrain motion
between circumferential fibers and improve the
stiffness characteristics of meniscus (Bullough
et al. 1970). The importance of the integrity of
the collagen network cannot be overemphasized, because disruption of this precise collagen ultrastructure results directly in alterations
in tissue biomechanics, predisposing to tearing
and a clinically significant loss of meniscal function (Thieman et al. 2009).
Meniscal function
The material properties of the meniscus are
closely related to its function. The combination of low compressive stiffness and low permeability suggests that the menisci are highly
efficient shock absorbers in the stifle. This is
crucial for the activities of dogs. When the
menisci are subjected to loading during weightbearing activities, they act as ‘firm pillows’
between the femoral and tibial condyles. Based
on their viscoelastic properties the wedgeshaped menisci also adapt to the incongruent articular surfaces until fluid flow ceases as
equilibrium is reached. Repeated compressive
loading and unloading of menisci create a circulation pathway that is important for tissue
nutrition and joint lubrication (Arnoczky et al.
1980).
Another important concept for understanding the role of the meniscus as a shock absorber
is the hoop tension theory. Shrive et al. (1978)
proposed that the meniscus is able to absorb
high loads across the joint by converting the
compressive forces into radially directed forces.
This theory has been confirmed in dogs by
direct measurements of hoop strain and contact pressures of the medial meniscus (Pozzi
et al. 2010a). As the meniscus is loaded, the
cranial and caudal attachments of the meniscus
are tensioned, along with the circumferential
fibers, to prevent the meniscus from extruding
35
(Figure 4.4). The tension developed in the
circumferential fibers from the cranial to the
caudal attachments is called ‘hoop tension.’ The
integrity of both collagen network and meniscal
attachments is critical for the hoop tension to
develop. A transection of the meniscus or its
attachments disrupts completely the primary
functions of the meniscus because it eliminates
the hoop tension (Pozzi et al. 2008; Pozzi et al.
2010b).
The meniscus contributes to stifle stability
and joint kinematics by enhancing congruity
between the convex tibial plateau and the round
femoral condyle. The effect of the meniscus
on joint congruity is evident when assessing
meniscal motion during flexion–extension. Both
menisci translate more than 13 mm caudally
on average as the stifle goes from extension
to flexion. Meniscal displacement maintains
congruity during the pronounced roll-back of
the femoral condyle (Park et al. 2016). This
increased congruity is important for joint stability. In the normal stifle, the CrCL is considered a primary restraint, while the menisci
act as secondary stabilizers. However, in the
CrCL-deficient stifle the menisci become primary stabilizers of the uncontrolled translation
and rotation of the joint. The caudal pole of
the medial meniscus is particularly important in
providing this stability, and as such is at highest
risk of injury if excessive femoro-tibial motion
is present, such as in the CrCL-deficient stifle
(Pozzi et al. 2006).
The contributions of the menisci to joint congruity and stability in both intact and CrCLdeficient stifles suggest that a functionally intact
meniscus should be preserved whenever possible. This approach may be especially important in the CrCL-deficient stifle, which may benefit significantly from the stabilizing effects of
the meniscus for improving already disrupted
joint kinematics. In a weight-bearing radiographic study evaluating joint stability after tibial plateau leveling osteotomy (TPLO), dogs
with an intact meniscus had a normal femorotibial alignment while dogs that underwent
meniscectomy had a small degree of tibial subluxation (Kim et al. 2012). For meniscal preservation it becomes crucial to protect the menisci
by stabilizing the joint with a technique that
most optimally reestablishes normal kinematics, neutralizing both cranio-caudal and rotational instability. On the other hand, it could be
Structure and Function
VetBooks.ir
36
(A)
(B)
(C)
Figure 4.4 Schematic depiction of the hoop tension theory. (A,B) The intact meniscus acts as a hammock hanging under
tension between the palms. The hammock holds a person only if it is firmly secured to the palms. Similarly, the meniscus
acts as a load-bearing structure only if its ligaments are firmly anchored to the tibia. (C) If the anchorage of the hammock
is cut, the person falls to the ground. The failure of the hammock is caused by its inability to develop the tension between
the two palms. Similarly, a transected meniscus (meniscal release) cannot develop the hoop tension (tension between the
palms) to function as a load-bearing structure. Copyright © Samantha J. Elmhurst at www.livingart.org.uk.
argued that leaving intact menisci in a CrCLdeficient stifle places them at unacceptable risk
for subsequent damage, driving the need for
additional surgery. This latter argument has
been used as the rationale for meniscal release
or meniscectomy in TPLO-, tibial tuberosity
advancement (TTA)-, and extracapsular-treated
CrCL-deficient stifles for the past 15 years (see
Chapters 25, 27, and 28). Meniscal release eliminates important functions in the stifle joint, but
may decrease the risk of subsequent meniscal
tear. As such, the surgeon needs to make treatment decisions regarding the menisci carefully
and with informed client consent (see Chapters 35 and 36).
References
Adams ME, Muir H. The glycosaminoglycans of
canine menisci. Biochem J 1981;197:385–389.
Adams ME, Ho YA. Localization of glycosaminoglycans in human and canine menisci and their
attachments. Connect Tissue Res. 1987;16:269–
279.
Arnoczky SP. Pathomechanics of cruciate ligaments
and meniscal injuries. In: Disease Mechanisms in
Small Animal Surgery, Bojrab MJ, ed, second edition. Philadelphia PA, Lea & Febiger. 1993, pp. 764–
776.
Arnoczky SP, Warren RF. The microvasculature of the
meniscus and its response to injury: an experimental study in the dog. Am J Sports Med 1983;11:131–
141.
Arnoczky SP, Marshall JL, Joseph A, et al. Meniscal
diffusion: an experimental study in the dog. Trans
Orthop Res Soc 1980;5:42.
Bullough PG, Munuera L, Murphy J, et al. The
strength of the menisci of the knee as it relates to
their fine structure. J Bone Joint Surg 1970;52B:564–
567.
Carpenter DH, Cooper RC. Mini review of canine
stifle joint anatomy. Anat Histol Embryol
2000;29:321–329.
VetBooks.ir
Meniscal Structure and Function
Cheung HS. Distribution of type I, II, III, V in the
pepsin solubilized collagen in bovine menisci. Connect Tissue Res 1987;16:343–356.
Cook JL, Tomlinson JL, Kreeger JM, et al. Induction of
meniscal regeneration in dogs using a novel biomaterial. Am J Sports Med 1999;27:658–665.
Evans HE. The skeleton, arthrology, the muscular system. In: Miller’s Anatomy of the Dog, third edition.
Philadelphia PA, WB Saunders. 1993, pp. 122–384.
Eyre DR, Wu JJ. Collagen of fibrocartilage: a distinctive molecular phenotype in bovine meniscus.
FEBS Lett 1983;158:265–270.
Helio Le Graverand MP, Ou Y, Schield-Yee T, et al.
The cells of the rabbit meniscus: their arrangement, interrelationship, morphological variations
and cytoarchitecture. J Anat 2001;198:525–535.
Hulse DA, Shires PK. The meniscus: anatomy, function and treatment. Comp Cont Ed Pract Vet
1983;5:765–774.
Kim SE, Lewis DD, Pozzi A. Effect of tibial plateau
leveling osteotomy on femorotibial subluxation: in vivo analysis during standing. Vet Surg
2012;41:465–470.
Noone TJ, Millis DL, Korvick DL, et al. Influence
of canine recombinant somatotropin hormone on
biomechanical and biochemical properties of the
medial meniscus in stifles with altered stability. Am
J Vet Res 2002;63:419–426.
Park B, Banks S, Pozzi A. Meniscal kinematics
through automatic 3D meniscus model extraction
from MR images: validation and application in
37
canine stifles. Annual Veterinary Orthopedic Society Meeting, Snowbird, Utah, March 12–18, 2016.
Pozzi A, Tonks CA, Ling H. Femorotibial contact
mechanics and meniscal strain after serial meniscectomy. Vet Surg 2010a;39:482–488.
Pozzi A, Kowaleski MP, Apelt D, et al. Effect of
medial meniscal release on tibial translation following tibial plateau leveling osteotomy. Vet Surg
2006;35:486–494.
Pozzi A, Kim SE, Lewis DD. Effect of transection of the caudal menisco-tibial ligament on
medial femorotibial contact mechanics. Vet Surg
2010b;39:489–495.
Pozzi A, Litsky AS, Field J, et al. Effect of medial
meniscal release on load transmission following tibial plateau leveling osteotomy. Vet Comp
Orthop Traumatol 2008;17:198–203.
Ralphs SC, Whitney WO. Arthroscopic evaluation
of menisci in dogs with cranial cruciate ligament
injuries: 100 cases (1999–2000). J Am Vet Med
Assoc. 2002;221:1601–1604.
Stephan JS, McLaughlin RM, Griffith G. Water content and glycosaminoglycan disaccharide concentration of the canine meniscus. Am J Vet Res
1998;59:213–216.
Shrive NG, O’Connor JJ, Goodfellow JW, et al. Loadbearing in the knee joint. Clin Orthop 1978;131:279–
287.
Thieman KM, Pozzi A, Ling HY, et al. Contact
mechanics of simulated meniscal tears in cadaveric
canine stifles. Vet Surg 2009;38:803–810.
VetBooks.ir
VetBooks.ir
5
Biomechanics of the Normal
and Cranial Cruciate
Ligament-Deficient Stifle
Antonio Pozzi and Stanley E. Kim
Normal stifle
The stifle is a complex, diarthrodial, synovial
joint that allows motion in three planes (Figure 5.1). The round femoral condyles articulate with the flat tibial condyles with a range of
motion about the medial-lateral axis of approximately 120◦ . Normal stifle angles range from
160◦ in full extension, to 40◦ in full flexion (Jaegger et al. 2002; Allen et al. 2009). Based on fluoroscopic kinematics during trot, walk, stair ascent
and sit, the stifle flexes to 35◦ and extends to
145◦ during these activities (Kim et al. 2015).
The flexion–extension motion occurs through a
combination of rolling and gliding of the femur
on the tibia. With rolling alone, the femoral
condyle would roll off the tibial plateau before
maximum flexion was achieved, whereas with
gliding alone the femoral shaft would impinge
on the tibia. Rollback is asymmetric: femorotibial contact translates more caudally on the lateral than on the medial plateau, resulting in
internal tibial rotation during stifle flexion with
a range of motion that can vary from 6◦ to 15◦
during sitting and trot (Vasseur & Arnoczky
1981). This change in rotational constraint over
a range of motion, which also occurs in the
human knee, has been termed the ‘screw-home’
mechanism.
Due to the slight tibial translation in the sagittal plane that is coupled with flexion and extension, it is clear that the stifle does not function as
a pure hinge joint. Medial-lateral and proximaldistal translation is tightly constrained by the
collateral ligaments, but still allows for rotation about the medial-lateral and longitudinal axes. Although the rotational motion about
the medial-lateral axis far exceeds the motion
about the other two axes, approximately 20◦
of varus–valgus and internal–external rotation
occurs over an entire walking–gait cycle in normal dogs (Korvick et al. 1994). Understanding
stifle kinematics in three dimensions rather than
simply attempting to address cranio-caudal stability is important for the treatment of cranial cruciate ligament (CrCL) deficiency. Both
a lack of neutralization (e.g., tibial osteotomies)
or absolute constraint (e.g., extracapsular stabilization) of internal–external rotation may lead
to abnormal mechanical stresses on the articular surfaces and progression of osteoarthritis
(Chailleux et al. 2007; Kim et al. 2008).
The patellofemoral joint is an important
contributor to complex stifle biomechanics
(Moore et al. 2016). Patellofemoral kinematics is
closely coupled with femorotibial kinematics,
as patellar flexion angle increases and the
patella translates distally as the femorotibial
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
39
VetBooks.ir
40
Structure and Function
TRANSLATIONS
Proximo-Distal
ROTATIONS
Internal–External
Medio-Lateral
Flexion–Extension
Cranio-Caudal
Adduction–Abduction
Figure 5.1 Line drawing illustrating the six degrees-of-freedom of the femoro-tibial articulation. The femur and the tibia
rotate and translate about the three axes shown in the drawing. Copyright © Samantha J. Elmhurst at www.livingart.org.uk.
joint flexes (Moore et al. 2016). The patella acts
as a pulley mechanism to improve the efficiency
of stifle extension, as it increases the lever arm
of the quadriceps mechanism by lengthening
the distance between the quadriceps muscle
force and the center of flexion–extension rotation of the stifle. In doing so, a significant force
compressing the patella against the femoral
condyle is generated as the muscle contracts.
This retropatellar force is an important contributor to the stability of the patello-femoral joint,
and results in a force acting on the distal femur
in the cranial–caudal direction. The balance of
extensor and flexor moment acting at the stifle
joint contributes to dynamic stability (Tepic et al.
2002).
Unlike most other diarthrodial joints in the
dog, the bony congruency between the femoral
condyle and the tibial plateau adds little to
the stability of the stifle. Rather, primary and
secondary soft-tissue stabilizers provide stability to the stifle. The CrCL acts as primary stabilizer for both cranial–caudal translation and
internal–external rotation. The caudal cruciate
ligament (CaCL) has a primary role in limiting caudal tibial translation, and also helps
to limit excessive internal–external rotation
(Arnockzky & Marshall 1977). The menisci act
as secondary stabilizers. The degree to which
they contribute to joint stability is dependent
on the condition of the primary stabilizers, in
particular the CrCL. In a CrCL-deficient stifle the medial meniscus plays a role in primary stabilization, acting as a wedge opposing
femoral condyle translation and rotation (Pozzi
et al. 2006). The increased mobility of the lateral
meniscus does not allow it to act as a wedge
between the femur and the tibia, and may protect it from impingement and tearing. Other
passive stabilizers include the collateral ligaments and the joint capsule.
The dynamic stability of the stifle in the various daily activities is provided by a delicate
interplay between passive stabilizers and active
musculature. The stifle is controlled mostly by
two-joint muscles that cross either the hip and
the stifle, or the stifle and the hock. Contraction
of one of these muscles alone produces movement of all the joints that the muscle crosses.
To isolate movement at a single joint, twojoint muscles contract with other muscles, frequently with a one-joint synergist. The quadriceps and the hamstrings act as synergists in
the stifle and simultaneously contract during
activity (co-contraction). Co-contraction is considered an important mechanism in functional
adaptation in human patients with anterior cruciate ligament rupture, but further research is
needed to understand its role in dogs.
The clinician needs to understand all the
motions in the stifle joint that are normally limited by the ligaments to perform and interpret
manual stress tests and correctly determine
the abnormality. The term instability has been
used to describe an abnormal motion that
exists in the joint due to a ligament injury.
The term laxity simply indicates increases in
motion or looseness, without providing any
direct indication of whether abnormal motion
occurs in vivo. The goal of a comprehensive
stifle examination is to detect an increase in the
amount of motion (translation or rotation) or an
abnormal position (subluxation) to determine
the specific anatomic defect that is present.
The manual stress examinations are designed
to test only one or two motions at a time,
and therefore the diagnosis cannot be based
solely on the abnormal motion detected with
a single manual stress. The diagnosis requires
knowledge of stifle biomechanics, and which
ligaments limit each of the possible motions in
the stifle. Ultimately, the clinical examination
must be interpreted considering the stifle in
a six-degrees of freedom system, recognizing
that six possible motions may occur in three
dimensions.
30
25
The CrCL contributes to passive restraint of the
stifle by limiting cranial translation of the tibia
relative to the femur, excessive internal rotation of the tibia, and hyperextension of the stifle
(Arnoczky & Marshall 1977). In vivo kinematic
studies have demonstrated that most changes
after CrCL transection are noted in the stance
phase of the gait (Korvick et al. 1994; Tashman
et al. 2004). Approximately 10 mm of cranial tibial translation is consistently observed and sustained throughout stance. Femorotibial alignment is restored during the swing phase, and is,
therefore, largely unaffected by CrCL deficiency
at a walk. The initial pattern of cranial translation progressively changes over time. Tashman
et al. (2004) demonstrated that by two years after
CrCL transection, the position of the tibia at the
terminal swing is shifted cranially by approximately 5 mm (Figure 5.2). Thus, the decrease
in dynamic instability was considered to be an
indication of more persistent tibial subluxation
throughout the gait cycle, rather than a return
towards normal stifle kinematics (Tashman et al.
2004). The in vivo investigations by Tashman
et al. and Korvick et al. were performed in normal dogs with acute, experimental CrCL transection. It is likely that stifles affected by naturally occurring CrCL rupture in clinical dogs
30
Pre-Treatment
2 Months
24 Months
20
15
(A)
Pre-Treatment
2 Months
24 Months
25
20
15
10
10
-0.05
41
Cranial cruciate ligament-deficient
stifle
Cranial Translation (mm)
Cranial Translation (mm)
VetBooks.ir
Biomechanics of the Normal and Cranial Cruciate Ligament-Deficient Stifle
0
0.05
0.1
Time (s)
0.15
0.2
-0.05
(B)
0
0.05
0.1
Time (s)
0.15
0.2
Figure 5.2 Craniocaudal translation of the canine stifle during the stance phase of gait in cranial cruciate ligament
(CrCL) intact (A) and CrCL-deficient (B) dogs. Data represent baseline before CrCL transection or sham CrCL-transection,
2 months after surgery, and 24 months after surgery. Note that there are obvious changes in tibial translation after CrCL
transection, whereas there is relatively little laxity in the intact CrCL during locomotion. Over time, cranial translation of
the tibia becomes incrementally worse, suggesting that periarticular fibrosis does not provide much dynamic stability to
the CrCL-deficient stifle. Source: Tashman et al. 2004. Reproduced with permission from John Wiley & Sons, Inc.
VetBooks.ir
42
Structure and Function
may not exhibit the same magnitude of subluxation, as periarticular fibrosis often exists at the
time of complete CrCL rupture (Hayashi et al.
2004).
The cranial tibial subluxation occurring during the stance phase of gait may be driven by
the quadriceps contraction, among other factors (Korvick et al. 1994; Tashman et al. 2004).
In the dog, the moment across the joint is
flexor from ground contact until mid-stance,
and then extensor until the end of the stance
phase (Colborne et al. 2005). Quadriceps contraction at extended joint angles produces CrCL
strain, but in the CrCL-deficient stifle in flexion,
quadriceps contraction cannot load the CrCL or
cause tibial subluxation. Thus, during the swing
phase quadriceps activation on a flexed stifle
does not cause subluxation, suggesting that the
swing phase is CrCL-independent in the dog
(Korvick et al. 1994; Tashman et al. 2004).
The CrCL is a passive restraint to excessive internal tibial rotation, and ex vivo studies
simulating weight-bearing demonstrated 14◦ of
internal tibial rotation after CrCL transection
(Warzee et al. 2001; Kim et al. 2009). Articular
surface geometry and lower tension in the lateral collateral ligament with the stifle in extension were thought to have induced this axial
rotational malalignment (Warzee et al., 2001,
Kim et al. 2009). Excessive peak internal rotation in CrCL-deficient stifles, however, has not
been observed in vivo (Tashman et al. 2004).
This suggests that the muscular forces about
the stifle, which have not been reproduced
in bench-top studies, are the primary stabilizers against abnormal axial rotation, and the
CrCL is a secondary rotational stabilizer at a
walk or trot. High-demand activities, however,
may generate higher axial torques that overcome muscular compensation, and elicit abnormal rotational stability in CrCL-deficient stifles.
Such investigations have yet to be performed in
the dog.
Joints and joint structures are complex systems whose components are interdependent on
one another and are constantly altering their
cellular and molecular mechanisms to maintain
and restore tissue homeostasis. In the stifle,
CrCL function is fundamentally important
in maintaining tissue homeostasis of other
structures such as the meniscus and cartilage.
In an attempt to maintain stifle function and
tissue homeostasis, these abnormal stresses on
compensating joint structures can then result
in their adaptation or their failure. This concept
has led to the idea that there is an envelope of
function or a range of loading that is compatible with overall homeostasis. Loads above or
below this ‘zone of homeostasis’ may lead to
pathologic changes. In vivo three-dimensional
kinematic studies have shown that the dog has
little capability for eliminating cranio-caudal
instability via neuromuscular compensation to
stay in the ‘zone of homeostasis’ (Korvick et al.
1994; Tashman et al. 2004; Anderst & Tashman
2009). In addition, both ex vivo and in vivo studies have reported abnormal contact mechanics
and increased tangential shear loading caused
by femoro-tibial subluxation (Pozzi et al. 2006;
Anderst & Tashman 2009). These alterations
in stifle biomechanics are likely an important
factor in osteoarthritis progression in the CrCLdeficient stifle. Cranial tibial subluxation results
in a spatial shift of loading patterns to where
articular cartilage is unable to accommodate
these loads, inducing osteoarthritis (Andriacchi
et al. 2004) (Figure 5.3). Cartilage metabolism
is dependent on maintenance of the mechanical stimuli that chondrocytes are adapted
for (Carter et al. 2004). Therefore, reduced or
increased loading of specific regions of the articular cartilage may trigger cartilage breakdown.
To prevent osteoarthritis, surgical treatment
of the CrCL-deficient stifle should aim at
restoring normal joint function. For an optimal
outcome, not only should cranio-caudal instability be restored but normal three-dimensional
kinematics and contact mechanics should be
obtained after surgical stabilization of the joint.
While aiming for normal joint biomechanics is
crucial when selecting surgical techniques for
stifle stabilization or CrCL repair, joint adaptation should be taken in account when selecting
the treatment for the CrCL-deficient stifle. For
example, a dog with a chronic CrCL-deficient
stifle may be at a too-advanced adaptation
stage to allow significant improvement of its
joint biomechanics. In this case, arthroscopy or
arthrotomy and meniscal treatment, followed
by rehabilitation, may be selected over a stabilization technique (Tivers et al. 2009). Further
work needs to be done to understand how
differences in stage of CrCL rupture may play a
role in treatment selection.
VetBooks.ir
Biomechanics of the Normal and Cranial Cruciate Ligament-Deficient Stifle
43
HEALTHY CARTILAGE TOLERATES
HIGH TO LOW PHYSIOLOGIC LOAD
BIOLOGIC
TRIGGER
Metabolic or
enzymatic
en matic
changes
MECHANICAL
TRIGGER
Loading
g shifts or
increases
FAILURE OF ADAPTATION OF THE
CARTILAGE
Chondrocyte death
Collagen breakage / fibrillation
Loss of macromolecules
INITIATION OF OA
HIGH LOAD
DEGENERATIVE CARTILAGE
Unable to tolerate physiologic loads
RAPID
PROGRESSION
LOW LOAD
SLOW
PROGRESSION
Figure 5.3 Diagram illustrating the pathomechanics theory of osteoarthritis (OA) proposed by Andriacchi. This theory
suggests that the mechanical environment of the stifle influences the initiation and progression of stifle osteoarthritis. A
healthy stifle can tolerate increased loads on cartilage without developing osteoarthritis. In contrast, a joint with
abnormal kinematics and contact pressure (i.e. shift of contact areas) responds to high loads with progression of
osteoarthritis. Therefore, decreasing load on degenerated cartilage may decrease progression of osteoarthritis. Notice that
biological as well as mechanical factors can act as the trigger for osteoarthritis.
References
Allen MJ, Leone KA, Lamonte K, et al. Cemented total
knee replacement in 24 dogs. Vet Surg 2009;38:555–
567.
Anderst WJ, Tashman. The association between
velocity of the center of closest proximity on
subchondral bones and osteoarthritis progression.
J Orthop Res 2009;27:71–77.
Andriacchi TP, Mündermann A, Smith RL, et al.
A framework for the in vivo pathomechanics
of osteoarthritis at the knee. Ann Biomed Eng
2004;32:447–457.
Arnoczky SP, Marshall JL. The cruciate ligaments of
the canine stifle: an anatomical and functional analysis. Am J Vet Res 1977;38:1807–1814.
Carter DR, Beaupre GS, Wong M, et al. The
mechanobiology of articular cartilage development and degeneration. Clin Orthop Relat Res
2004;427:S69–S77.
Chailleux N, Lussier B, De Guise J, et al. In vitro 3dimensional kinematic evaluation of 2 corrective
operations for cranial cruciate ligament-deficient
stifle. Can J Vet Res 2007;71:175–180.
Colborne GR, Innes JF, Comerford EJ, et al. Distribution of power across the hind limb joints in
Labrador Retrievers and Greyhounds. Am J Vet Res
2005;66:1563–1571.
Hayashi K, Manley PA, Muir P. Cranial cruciate
ligament physiology in dogs with cruciate disease: a review. J Am Anim Hosp 2004;40:385–
390.
VetBooks.ir
44
Structure and Function
Jaegger G, Marcellin-Little DJ, Levine D. Reliability of
goniometry in Labrador Retrievers. Am J Vet Res
2002;63:979–986.
Kim SE, Pozzi A, Banks SA, et al. Effect of tibial
plateau leveling osteotomy on femorotibial contact mechanics and stifle kinematics. Vet Surg
2009;38:33–39.
Kim SE, Pozzi A, Kowaleski MP, et al. Tibial
osteotomies for cranial cruciate ligament insufficiency in dogs. Vet Surg 2008;37:111–125.
Kim SE, Jones SC, Lewis DD, et al. In vivo three
dimensional knee kinematics during daily
activities in dogs. J Orthop Res 2015;33:1603–
1610.
Korvick DL, Pijanowski GJ, Schaeffer DJ. Threedimensional kinematics of the intact and cranial
cruciate ligament-deficient stifle of dogs. J Biomech
1994;27:77–87.
Moore EJ, Kim SE, Banks SA, et al. Normal
patellofemoral kinematic patterns during daily
activities in dogs. BMC Vet Res. 2016;12:262.
Pozzi A, Kowaleski MP, Apelt D, et al. Effect of medial
meniscal release on tibial translation after tibial
plateau leveling osteotomy. Vet Surg 2006;35:486–
494.
Tashman S, Anderst W, Kolowich P, et al. Kinematics
of the ACL deficient canine knee during gait: serial
changes over two years. J Orthop Res 2004;22:931–
941.
Tivers MS, Commerford EJ, Owen MR. Does a fabellatibial suture alter the outcome for dogs with cranial
cruciate ligament insufficiency undergoing arthrotomy and caudal pole medial meniscectomy? Vet
Comp Orthop Traumatol 2009;22:283–288.
Tepic S, Damur DM, Montavon PM. Biomechanics of
the stifle joint. Proceedings, 1st World Orthopaedic
Veterinary Congress. Munich, Germany. 2002,
pp. 189–190.
Vasseur PB, Arnoczky SP. Collateral ligaments of the
canine stifle joint: anatomic and functional analysis. Am J Vet Res 1981;42:1133–1137.
Warzee CC, Dejardin LM, Arnoczky SP, et al. Effect
of tibial plateau leveling on cranial and caudal
tibial thrusts in canine cranial cruciate-deficient
stifles: an in vitro experimental study. Vet Surg
2001;30:278–286.
VetBooks.ir
Section II
Etiopathogenesis of Cruciate
Ligament Rupture
Introduction
Historically, cruciate ligament rupture (CR) in
the dog has been considered a consequence
of accidental injury, with subsequent development of stifle arthritis. However, particularly
since the late 1980s, this paradigm has been
challenged. Second cruciate ruptures were
found to be common in affected dogs, with
many dogs initially presenting with bilateral
CR. More recent work has shown that stifle
arthritis is present during the early phase of
the disease as cruciate ligament fiber rupture
develops in the stable stifle. Disease progres-
sion then leads to the development of complete
CR and associated stifle instability in most
affected dogs. Recent publications have shown
that stifle synovitis is a significant factor in
progression of the disease over time. Although,
a substantial genetic contribution to risk of CR
exists, the specific events that initiate the disease remain poorly understood. Recent genetic
research has highlighted the polygenic nature
of the trait and confirmed moderate heritability.
Future research should be focused on advancing understanding of the factors that lead to
disease initiation, particularly causal genetic
variants.
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
45
VetBooks.ir
VetBooks.ir
6
Histology of Cruciate
Ligament Rupture
Kei Hayashi
Pathology of cranial cruciate
ligament rupture
The exact etiopathogenesis of canine cruciate
ligament rupture (CR) is not defined. Although
acute cranial cruciate ligament injury does
occur with trauma, a number of previous studies have suggested that the majority of CR cases
are the result of chronic degenerative changes
within the ligament (Vasseur et al. 1985; Hayashi
et al. 2003a).
The development of progressive CR appears
to involve a gradual degeneration of both cruciate ligaments, inflammatory disease in the stifle
joint, partial CR, and eventually complete rupture. After rupture, secondary changes such as
progressive arthritis and meniscal injury often
develop. Initially, slight weakening or stretching of the cranial cruciate ligament (CrCL)
may not cause lameness, but can produce mild
instability within the joint, and therefore initiate arthritic joint degeneration. However, it is
unclear whether this represents the initial phase
of the condition, or whether the development
of stifle synovitis is an initial event. Dogs with
incipient or partial CR have a stable joint, but
are presented with lameness, effusion of the stifle joint, and synovitis. Complete CR produces
obvious instability of the stifle joint, resulting in
more severe joint pain, lameness, and progressive degenerative changes within the joint. Clinical observations have demonstrated that these
changes consist of periarticular osteophyte formation, capsular thickening, and meniscal damage. As these changes progress, the joints may
become more stable, although a recent experimental study suggested that periarticular fibrosis does little to improve dynamic instability
during locomotion (Tashman et al. 2004). Dogs
with advanced or end-stage pathologic changes
within the stifle may have little palpable passive instability because of extensive periarticular fibrosis. After a partial or complete CR,
some degree of tissue repair response arises in
the epiligamentous region of the CrCL (Hayashi
et al. 2003a). In the human anterior cruciate ligament (ACL), distinct histologic phases of tissue repair, including an inflammatory phase,
a epiligamentous repair phase, a proliferative
phase and a remodeling phase, develop after
rupture (Murray et al. 2000). Whether similar phases exist in dogs is not known. Expansion of the volume of the epiligamentous tissue does occur in the dog during a repair phase
that lasts many weeks. However, a bridging
scar does not form in the rupture site. Eventually, synovial tissue covers the ruptured ends of
the CrCL.
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
47
VetBooks.ir
48
Etiopathogenesis of Cruciate Ligament Rupture
Histologic features of cruciate
ligament
The CrCL is a complex structure consisting of an
extracellular matrix (ECM) and a diverse population of cells. It has distinctive histologic features typical of dense collagenous connective
tissues (ligaments and tendons). The ECM proteins in CrCL are primarily composed of type
I collagen. Bundles of collagen fibers are longitudinally oriented, mostly running parallel
to one another. Normal CrCL collagen fibers
have a recurrent undulating wave or crimped
structure (Figure 6.1) (Hayashi et al. 2003a).
The human ACL has been shown to also contain collagen types III, IV, V and VI and other
ECM components, including glycosaminogly-
cans, fibronectin, laminin, entactin, tenascin,
and undulin (Neurath & Stofft 1992). The matrix
of the CrCL represents a complicated regulatory
network of proteins, glycoproteins, viscoelastic fibers and glycosaminoglycans with multiple
functional interactions.
The predominant cell type in the CrCL
is the fibroblast. Ligament fibroblasts are
arranged in long parallel rows between collagen fiber bundles. In the human ACL, three
different phenotypes of fibroblasts have been
described: fusiform or spindle-shaped, ovoid,
and spheroid (Murray & Spector 1999). The
cytoplasm of fusiform fibroblasts is intimately
attached to the extracellular collagen and
follows the crimped waveform of the fibers.
Ovoid and spheroid fibroblasts are situated in
Figure 6.1 Longitudinal sections of intact (A,B) and ruptured CrCL (C,D) from a 2-year-old ovariohysterectomized
Beagle and a 7-year-old castrated male Golden Retriever, respectively, viewed using bright-light (A,C) and circularly
polarized light (B,D) microscopy. (A,B) Intact CrCL from young dogs has a hierarchically organized structure.
Birefringence of the extracellular matrix (ECM) collagen and the crimped structure of collagen fiber bundles are clearly
visible in polarized light. (C,D) The disorganized regions of the ECM in ruptured CrCL exhibit a loss of birefringence and
crimp, as well as a loss of ligament fibroblasts. Scale bars = 100 μm. Source: Hayashi et al. 2003a. Reproduced with
permission from John Wiley & Sons, Inc.
VetBooks.ir
Histology of Cruciate Ligament Rupture
the loose connective tissue between collagen
fibers. It is presently unclear whether these cells
represent differing metabolic states of the same
cells or whether they are distinctly different
fibroblasts.
A histologic study of the human ACL identified three histologically different zones along
the anteromedial bundle as it coursed from
the femoral to the tibial attachment (Murray &
Spector 1999). Two of the zones, the fusiform
and ovoid, were located in the proximal onequarter of the bundle, while the third spheroid
zone occupied the distal three-quarters of the
fiber bundles. The fusiform cell zone was characterized by a high number density of longitudinally oriented cells with a fusiform-shaped
nucleus, longitudinal blood vessels, and high
crimp length. The cytoplasm of the cells in this
zone appeared to be intimately attached to the
extracellular collagen and followed the crimp
waveform of the fibers. The ovoid cell zone
was characterized by a high number density of
cells with an ovoid-shaped nucleus, longitudinal vessels, and a high crimp length. Also in this
zone, the cytoplasm of the cells appeared to follow the waveform of the adjacent collagen. The
spheroid cell zone was characterized by a low
density of spheroid cells, few blood vessels, and
a short crimp length. Cells were noted within
and among fascicles, as well as within lacunae.
The role of the various fibroblast phenotypes
in the maintenance of the human ACL is not
known.
The histologic structure of the cruciate ligament is not homogeneous. In ACL, it has been
reported that there is a zone where the tissue
resembles fibrocartilage (Petersen & Tillmann
1999). The fibrocartilaginous zone is located
5–10 mm proximal to the tibial attachment in
the anterior portion of the ligament. Within this
zone, the cells are arranged in columns and
the cell shape is round to ovoid. Transmission
electron microscopy reveals typical features of
chondrocytes. These chondrocyte-like cells are
surrounded by a felt-like pericellular matrix,
a high content of cellular organelles, and short
processes on the cell surface. The pericellular
collagen is positive for type II collagen. An
avascular zone is located within the fibrocartilage of the anterior part where the ligament
faces the anterior rim of the intercondylar
fossa. It has been proposed that the stimulus
49
for the development of fibrocartilage within
dense connective tissue is shearing and compressive stress (Milz et al. 2005). In the ACL,
this biomechanical situation may occur when
the ligament impinges on the anterior rim of
the intercondylar fossa when the knee is fully
extended (Quasnichka et al. 2005).
Histologic features of both the ligament cells
and the ECM appear to change with aging
(Hasegawa et al. 2013). In a study characterizing age-related changes in ACL from 80 subjects (age 23–94 years), the total cell number in normal ACL decreased with aging but
increased in degenerated ACL with the formation of perivascular cell aggregates and islands
of chondrocyte-like cells. Based on immunohistochemical staining, collagen I was expressed
throughout normal and degenerated ACL. Collagen II and X were detected only in the
areas with chondroid metaplasia. This study
suggested that the chondrocyte-like phenotype
produces an abnormal ECM and may predispose ACL to mechanical failure. Similar agerelated changes are reported in canine CrCL, as
described later in this chapter.
Histopathology of the canine cranial
cruciate ligament
Cell morphology was studied in normal cruciate ligaments from disease-free stifle joints
from dogs with a high (Labrador Retriever)
and low (Greyhound) risk of CR (Smith et al.
2012). Both CrCL and caudal cruciate ligament
(CdCL) contained cells of heterogeneous morphologies, where cells were arranged between
collagen bundles and frequently had cytoplasmic processes. Some of these processes were
long (type A cells), others were shorter, thicker
and more branched (type B cells), and some had
no processes (type C cells). Processes were frequently shown to contact other cells, extending longitudinally and transversely through the
cruciate ligaments. Cells with longer processes
had fusiform nuclei, and those with no processes had rounded nuclei and were more frequent in the mid-substance of both the CrCL
and the CdCL. Cells with long processes were
more commonly noted in the cruciate ligaments
of the Greyhound. As contact between cells may
VetBooks.ir
50
Etiopathogenesis of Cruciate Ligament Rupture
facilitate direct communication, variation in cell
morphology between breeds with a different
risk of CrCL rupture may reflect differences in
cruciate ligament physiology.
The canine CrCL undergoes a partial fibrocartilagenous transformation as described in
human ACL, which may represent chronic
and irreversible degeneration. This idiopathic
degeneration is a common histologic finding of
intact CrCL, despite its grossly normal appearance. A histologic study reported that the CrCL
of dogs weighing greater than 15 kg consistently had microscopic evidence of degenerative changes by 5 years of age (Vasseur et al.
1985). These changes are characterized by a loss
of ligament fibroblasts, metaplasia of surviving
fibroblasts to chondrocytes, and failure to maintain collagen fiber bundles, which progressed
in severity with age. The CrCL in dogs weighing less than 15 kg generally had less severe
alterations than those in heavier dogs, and the
onset of the degenerative process was delayed
by several years. The deep core region of the
CrCL deteriorates earlier than the superficial
epiligamentous region, and the mid-portion of
the CrCL deteriorates earlier than regions close
to bony attachments.
In ruptured CrCL, more severe changes such
as hyalinization, mineralization, and cloning
of chondrocyte-like cells can also occur. However, inflammatory or reparative responses are
rarely observed (Hayashi et al. 2003a). Significant loss of fibroblasts from the core region of
ruptured CrCL occurs. In contrast, cell number densities are similar in ruptured and intact
CrCL in the epiligamentous region (Hayashi
et al. 2003a,b). In ruptured CrCL, the numbers of typical ligament fibroblasts (fusiform
and ovoid cells) are decreased, while numbers of cells exhibiting chondroid transformation (spheroid cells) are increased in the core
region (Figures 6.1–6.3). The structure of the
ECM collagen in the core region is extensively
disrupted in ruptured CrCL. Rupture of the
CrCL is also associated with disruption of the
hierarchical architecture of ECM collagen, with
a loss of the normal crimp and loss of birefringence (Figures 6.1, 6.2, and 6.4). A histological study reported that crimp was no longer
detectable in many ligament specimens from
dogs with CrCL rupture (Figures 6.1, 6.4, and
6.5) (Hayashi et al. 2003a). Interestingly, in the
50 μm
50 μm
(A)
(B)
Figure 6.2 Photomicrographs of longitudinal frozen
sections of intact cranial cruciate ligament (CrCL) from a
2-year-old ovariohysterectomized Beagle (A) and an
8-year-old ovariohysterectomized Labrador Retriever (B)
obtained via bright-light microscopy. Specimens were
stained histochemically for lactate dehydrogenase (LDH),
a marker of cell viability. (A) Central part of the core
region of the intact CrCL from a young dog. Notice
parallel rows of fusiform and ovoid LDH-stained ligament
fibroblasts, with an organized extracellular matrix (ECM)
containing crimped collagen fibers. (B) Central part of the
core region of the intact CCL from an old dog. Note the
decreased number of ligament fibroblasts; many cells are
devitalized (low LDH) with an ovoid phenotype.
Collagen fibers within the ECM have also been
disrupted.
ruptured CrCL specimens in which crimp was
still detectable, crimp length was significantly
increased, and the crimp angle tended to be
lower compared with intact CrCL from young
dogs (Figure 6.5) (Hayashi et al. 2003a). These
data suggest that the remaining organized collagen experiences mechanical overload that elongates the crimp within the collagen fibers, as
progressive CrCL rupture develops over time,
Fusiform Phenotype
Ovoid Phenotype
Spheroid Phenotype
600
500
400
300
*
200
*
*
100
0
(A)
5000
4000
Intact
Ruptured
CrCL Status
Fusiform Phenotype
Ovoid Phenotype
Spheroid Phenotype
Epiligamentous
Region
3000
2000
1000
*
0
(B)
Intact
Ruptured
CrCL Status
Figure 6.3 Relationship of cell number densities to
cranial cruciate ligament (CrCL) rupture status in the core
(A) and epiligamentous (B) regions-of-interest. ∗ Columns
are significantly different from intact CrCL (P < 0.05).
Source: Hayashi et al. 2003a. Reproduced with
permission from John Wiley & Sons, Inc.
thereby causing the collagen to have a longer
crimp length and a smaller crimp angle. These
findings also support the general hypothesis
that microinjury to the ligament from mechanical overload may form an important part of
the mechanically induced signaling events that
orchestrate CrCL remodeling, and may be a key
factor in the mechanism that leads to gradual
CR over time.
Fibroblast viability and metabolism are different in young intact, aged intact, and ruptured CrCL (Hayashi et al. 2003b). Metabolically
active viable fibroblasts detected by a metabolic
marker, lactate dehydrogenase (LDH), were
seen in all intact and ruptured CrCLs. However, the number of nonviable cells in the core
region of ruptured CrCLs was greater than that
in intact CrCLs of young and aged dogs (Figures 6.6 and 6.7).
Extracellular Matrix Grade
3.0
Core Region
51
*
2.5
2.0
1.5
1.0
0.5
0.0
(A)
Percentage Birefringent Collagen
Cell Number Density (#/mm2)
700
Cell Number Density (#/mm2)
VetBooks.ir
Histology of Cruciate Ligament Rupture
Intact
Ruptured
CrCL Status
100
(B)
80
60
40
*
20
0
Intact
Ruptured
CrCL Status
Figure 6.4 Relationship of extracellular matrix (ECM)
organization (A) and collagen birefringence (B) to cranial
cruciate ligament (CrCL) rupture status in the core
region-of-interest. CrCL were graded using a numerical
rating scale (1, highly organized fibrous tissue structure
with parallel alignment and dense packing of collagen
fibers; 2, partially disrupted organized fibrous structure of
collagen fibers; 3, total loss of organized fibrous structure
of collagen with homogenous appearance of the ECM).
Values represent the mean of five fields-of-view.
∗ Columns are significantly different from intact CrCL
(P < 0.05). Source: Hayashi et al. 2003a. Reproduced
with permission from John Wiley & Sons, Inc.
Cruciate ligament adaptation
and repair
The CrCL is a hypovascular tissue and its vascular distribution is not homogeneous (Hayashi
et al. 2011a). In a study describing vascular distribution in grossly intact canine CrCL using
immunohistochemical staining for two components of blood vessels (factor VIII for endothelial cells, and laminin for basement membrane),
vascular staining was sparsely identified
Etiopathogenesis of Cruciate Ligament Rupture
Crimp Angle (degree)
60
50
#
40
30
20
10
0
Intact
Ruptured
CrCL Status
(A)
60
Crimp Length (μm)
VetBooks.ir
52
*
40
20
0
(B)
(A)
Intact
Ruptured
CrCL Status
Figure 6.5 Relationship of crimp angle (A) and crimp
length (B) to cranial cruciate ligament (CrCL) rupture.
∗ Significantly different from intact CrCL (P < 0.05).
# Lower crimp angle compared with intact CrCL
(P < 0.15). Source: Hayashi et al. 2003a. Reproduced
with permission from John Wiley & Sons, Inc.
throughout the entire CrCL. However, the
proximal portion of the CrCL appears to have
a greater number of vessels than the middle or
distal portions of the ligament. In a study determining the microanatomic vascular distribution
in ruptured canine CrCL using specific vascular
immunohistochemical staining, the ruptured
CrCL was more vascular than intact CrCL.
However, there was no difference in vascular
density between the torn end and the remaining
core area of the ruptured CrCL (Hayashi et al.
2011b) (Figure 6.8). It remains to be determined
whether this finding is associated with the
cause of CrCL rupture, or is a result of CrCL
rupture.
Ruptured CrCLs have significantly higher
amounts of immature collagen crosslinks, total
and sulfated glycosaminoglycans and water
(B)
Figure 6.6 Photomicrographs of longitudinal frozen
sections of ruptured cranial cruciate ligament (CrCL) from
a 6-year-old ovariohysterectomized Labrador Retriever
obtained via bright-light microscopy. Specimens were
stained histochemically for lactate dehydrogenase (LDH),
a marker of cell viability. (A) Periphery of the main axial
tissue component (core) region of the ruptured CrCL.
Note the parallel rows of fusiform and ovoid
LDH-positive ligament fibroblasts, with an organized
extracellular matrix (ECM) containing crimped collagen
fibers. (B) Central part of the core region of the ruptured
CrCL. Note the low number of ligament fibroblasts; many
cells are devitalized (no LDH staining) with a spheroid
phenotype (arrows). Most of the collagen fibrils within
the ECM have been disrupted. Scale bar = 50 μm. Source:
Hayashi et al. 2003b. Reproduced with permission from
the American Veterinary Medical Association.
content (cartilage-like material), and concentration of pro-matrix metalloproteinase 2 (gelatinase), compared to those of the intact ligament
(Comerford et al. 2004). These findings suggest
that the ECM of ruptured CrCL has an increased
matrix turnover. Cartilage-like tissue is more
vulnerable to disruption under normal tensile
loading, and therefore CrCL degeneration with
3500
Total cell density (#/mm2)
3000
Epiligamentous region
Core region
A,I
53
A,I
A,I
2500
2000
1500
1000
a,ll
a,b,ll
b,ll
500
0
(A)
Young - Intact Aged - Intact
dogs
dogs
Group
Ruptured
(A)
140
Non viable LDH– cell density (#/mm2)
VetBooks.ir
Histology of Cruciate Ligament Rupture
b,ll
Epiligamentous region
120
Core region
100
(B)
80
60
40
20
0
A,I
a,ll
Young - Intact
dogs
a,l
A,I
Aged - Intact
dogs
Group
A,I
Ruptured
(B)
Figure 6.7 Relationship of total cell number densities to
CrCL disease status in the epiligamentous and core
regions of the CrCL (A), and relationship of non-viable
LDH– cell densities to CrCL disease status in the
epiligamentous and core regions of the CrCL (B).
Columns within a region with differing upper- or
lower-case letters are significantly different (P < 0.05).
Columns within a CrCL status group with differing Roman
numerals are significantly different. Source: Hayashi et al.
2003b. Reproduced with permission from the American
Veterinary Medical Association.
fibrocartilaginous transformation may predispose CrCL to pathological rupture.
Areas of fibrocartilage are also observed,
however, in grossly normal CrCL in lowrisk breeds (Greyhounds), when intrinsic ECM
changes in the CrCLs of Labrador Retriever
(high-risk breed) are compared with those in
Greyhounds (Comerford et al. 2006). Transmission electron microscopy revealed that the collagen fibril diameters of Greyhound CrCL were
larger than those of Labrador Retrievers, which
may relate to tissue maturity and the tissue’s
mechanical properties. Histology revealed the
(C)
Figure 6.8 Immunohistochemical staining for factor VIII
in the core region of intact (A) and ruptured (B) canine
cranial cruciate ligaments, and the torn end of ruptured
canine cruciate ligament (C). Scale bars = 50 μm. Positive
red staining can be identified in the lumen of vascular
structures. Source: Hayashi et al. 2011b. Reproduced
with permission from John Wiley & Sons, Inc.
VetBooks.ir
54
Etiopathogenesis of Cruciate Ligament Rupture
presence of fibrocartilagenous areas in both
breeds.
Elastin fibers, composed of an elastin core
and fibrillin containing microfibrils, are traditionally considered minor components of the
ligament ECM. The elastin content is high in
Greyhound CrCL, and is associated with histological signs of degeneration (Smith et al. 2014).
The appearance of oxytalan fibers (bundles of
microfibrils) in degenerative CrCL ECM may
reflect an adaptive or reparative response to
normal or increased loads (Smith et al. 2014).
These observations suggest that the formation of fibrocartilage is clearly not a disadvantage to healthy racing Greyhounds, and cannot
be regarded as pathological degeneration in this
breed. Fibrocartilage would appear to protect
CrCLs in Greyhounds, but in high-risk breeds
it may be indicative of a mild degenerative
change that is a risk factor for ligament rupture.
It is currently unclear whether CrCL degeneration and transformation into fibrocartilage is
a key pathologic change that is an important
risk factor for eventual CrCL rupture in certain
breeds of dog. Elastin fibers may have an adaptive or reparative role secondary to normal or
increased loads.
Conclusions
Taken together, the current literature suggests
that progressive CrCL fiber tearing during the
development of stifle instability is associated
with histologic changes to the matrix that
include a loss of ligament fibroblasts and chondroid transformation of surviving cells. The
disruption of matrix collagen includes a loss
of crimp. Two central hypotheses have been
proposed regarding the initial mechanism that
leads to cruciate ligament degeneration and
then rupture: (1) A primary defect in the ligament tissue itself or in the metabolism of the
cruciate ligaments that leads to fiber rupture
and eventual partial rupture, particularly of the
CrCL, with development of microinstability of
the stifle; and (2) a dysregulation of synovial
immune responses and the development of a
chronic synovitis that promotes cruciate ligament degeneration, as ligament nutrition and
metabolism are related to synovial fluid phys-
iology. These hypotheses are discussed further
in other chapters in this section. Confirmation
that one or both of these hypotheses is correct
should be a focus of future work studying the
CR mechanism in the dog.
References
Comerford EJ, Innes JF, Tarlton JF, et al. Investigation
of the composition, turnover, and thermal properties of rupture cranial cruciate ligaments of dogs.
Am J Vet Res 2004;65:1136–1141.
Comerford EJ, Tarlton JF, Wales A, et al. Ultrastructural differences in cranial cruciate ligaments from
dogs of two breeds with a differing predisposition to ligament degeneration and rupture. J Comp
Pathol 2006;134:8–16.
Hayashi K, Frank JD, Dubinsky C, et al. Histologic
changes in ruptured canine cranial cruciate ligament. Vet Surg 2003a; 32:269–277.
Hayashi K, Frank JD, Hao Z, et al. Evaluation of ligament fibroblast viability in ruptured cranial cruciate ligament of dogs. Am J Vet Res 2003b;64:1010–
1016.
Hayashi K, Bhandal J, Kim SY, et al. Immunohistochemical and histomorphometric evaluation of
vascular distribution in intact canine cranial cruciate ligament. Vet Surg 2011a;40:192–197.
Hayashi K, Bhandal J, Rodriguez CO, Jr, et al. Vascular distribution in ruptured canine cranial cruciate
ligament. Vet Surg 2011b; 40:198–203.
Hasegawa A, Nakahara H, Kinoshita M, et al. Cellular and extracellular matrix changes in anterior
cruciate ligaments during human knee aging and
osteoarthritis. Arthritis Res Ther 2013;15:R29.
Milz S, Benjamin M, Putz R. Molecular parameters indicating adaptation to mechanical stress in
fibrous connective tissue. Adv Anat Embryol Cell
Biol 2005;178:1–71.
Murray MM, Spector M. Fibroblast distribution in the
anteromedial bundle of the human anterior cruciate ligament: the presence of alpha-smooth muscle
actin-positive cells. J Orthop Res 1999;17:18–27.
Murray MM, Martin SD, Martin TL, et al. Histological changes in the human anterior cruciate ligament
after rupture. J Bone Joint Surg Am 2000;82A:1387–
1397.
Neurath MF, Stofft E. Structure and function of
matrix components in the cruciate ligaments. An
immunohistochemical, electron-microscopic, and
immunoelectron-microscopic study. Acta Anat
1992;145:387–394.
Petersen W, Tillmann B. Structure and vascularization of the cruciate ligaments of the human knee
joint. Anat Embryol 1999;200:325–334.
Quasnichka HL, Anderson-MacKenzie JM, Tarlton
JF, et al. Cruciate ligament laxity and femoral
VetBooks.ir
Histology of Cruciate Ligament Rupture
intercondylar notch narrowing in early-stage knee
osteoarthritis. Arthritis Rheum 2005;52:3100–3109.
Smith KD, Vaughan-Thomas A, Spiller DG, et al. Variations in cell morphology in the canine cruciate ligament complex. Vet J. 2012;193:561–566.
Smith KD, Clegg PD, Innes JF, et al. Elastin content is
high in the canine cruciate ligament and is associated with degeneration. Vet J. 2014;199:169–74.
55
Tashman S, Anderst W, Kolowich P, et al. Kinematics
of the ACL-deficient canine knee during gait: serial
changes over two years. J Orthop Res 2004;22:931–
941.
Vasseur PB, Pool RR, Arnoczky SP, et al. Correlative
biomechanical and histologic study of the cranial
cruciate ligament in dogs. Am J Vet Res 1985;46:
1842–1854.
VetBooks.ir
VetBooks.ir
7
Genetics of Cruciate
Ligament Rupture
Lauren A. Baker and Peter Muir
Introduction
Multiple epidemiologic factors have been identified that may influence the risk of cruciate
ligament rupture (CR) (for a full discussion, see
Chapter 14). Of these, the most important risk
factor for disease initiation is breed. Dogs of
high-risk breeds tend to present with CR at an
earlier age, and are more likely to present with
bilateral rupture (Harasen 2008; Guthrie et al.
2012). The effect of breed on CR presentation
suggests that genetic factors play a role in CR
pathogenesis. It is likely that genetic risk factors
combine with environmental modifiers such as
body condition score or neuter status to affect
expression of the CR trait. Identification of
valid genetic risk factors influencing CR may
lead to the discovery of targets for medical
intervention and aid in the development of
a predictive genetic test for the condition.
A predictive test of CR risk may be used to
screen young dogs for predisposition to the
disease. This information can then be used
to develop selective breeding strategies or to
counsel clients on environmental modifications
to minimize the impact of the clinical course of
the disease. In order to meet these goals, several
recent investigations have been conducted to
discover the genetic basis of CR.
Heritability
Statistically, heritability is defined as the proportion of phenotypic variance that may be
explained by genetic variance. It may be loosely
defined as the extent to which individual
genetic differences contribute to changes in
observable phenotype. Heritability is expressed
as a number between 0.0 and 1.0. For example,
a heritability of 0.5 says that approximately 50%
of a disease risk is genetic, and the other 50%
must come from environmental influences. A
disease that is 100% genetic would have a heritability of 1.
The heritability of CR has been assessed in
three high-risk breeds: the Boxer, the Newfoundland, and the Labrador Retriever (Nielen
et al. 2001; Wilke et al. 2006; Baker et al. 2017).
Newfoundlands have the highest prevalence of
CR compared to any other breed. A study of 411
Newfoundlands (92 cases, 319 controls) estimated narrow-sense heritability derived from
an 11-generation pedigree at 0.27 (Wilke et al.
2006). Nielen et al. (2001) reported heritability of
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
57
VetBooks.ir
58
Etiopathogenesis of Cruciate Ligament Rupture
CR at 0.28 in a prospective study of 414 Boxer
litters. Both of these studies used restricted
maximum likelihood (REML) analysis for calculating heritability estimates. In a study of 237
Labrador Retrievers, the present authors’ group
employed a Bayesian method (Pérez & de los
Campos 2014) to estimate narrow-sense heritability from single nucleotide polymorphism
(SNP) markers, as well as from pedigrees. Both
methods gave similar results, with a heritability of CR in Labrador Retrievers estimated at
0.49 and 0.48, respectively (Baker et al. 2017).
It is unclear whether the higher heritability
indicates that CR is truly more heritable in the
Labrador Retriever, or if it is a reflection of the
Bayesian method used.
Taken together, these results suggest that
canine CR is moderately heritable within the
range of 0.3–0.5. Heritability estimates of this
level indicate that a reasonable reduction can be
expected in overall prevalence of the condition
through genetic screening applied to a selective
breeding program (Nielen et al. 2001). While it
has previously been suggested that CR has an
autosomal recessive mode of inheritance (Wilke
et al. 2006), recent research suggests that CR is
a complex polygenic trait (Baird et al. 2014a,b;
Baker et al. 2017).
Complex trait genetics
Complex traits or diseases are simply defined
as phenotypic traits that are determined by
both genetic and non-genetic (environmental) factors. The genetic factors that influence
complex traits are typically composed of many
small-effect mutations and fewer large-effect
mutations that contribute predominantly additively to phenotypic variation (Robinson et al.
2014). These mutations are expected to be
large in number, and so their contribution to
variance on a population level is quite small
(Robinson et al. 2014). The relatively small contribution of individual mutations makes all but
the largest effect mutations difficult to detect
without very large sample sizes. Complete discovery of genetic variants contributing to CR
(and other complex traits) will likely require
a combination of complementary analyses
including candidate gene analyses, large-scale
genome-wide association studies (GWAS), and
next-generation sequencing.
Candidate gene analyses
For many, the candidate gene approach represents the first logical step for genetic association testing. Prior knowledge of gene function is used to choose candidate genes to test
for association, based on their potential role in
disease etiology. Candidate gene studies have
been successful in identifying large-effect mutations, and mutations associated with Mendelian
(monogenic) traits. However, this approach has
faced criticism as current knowledge of gene
functions is limited, and thus disease associations may be missed when they are not within
‘obvious’ genes (Tabor et al. 2002; Baird et al.
2014a). Additionally, the genetic contribution to
complex traits, such as CR, likely includes many
small-effect variants. Therefore, it is doubtful
that associations identified in a candidate gene
study would explain a large proportion of the
genetic variance for the trait. With that being
said, associations identified in these studies
are still valuable as part of genetic discovery,
and should be considered complementary to
genome-wide approaches.
In a study of a population of Newfoundland dogs, several genes were selected for analysis based on their known association with
joint hypermobility in cattle or development
of primary arthritis in humans. These included
Cartilage Oligomeric Matrix Protein (COMP),
Matrilin-3 (MATN), Collagen Type 9 alpha 1, 2,
and 3 (COL9A1, COL9A2, COL9A3), Fibrillin-1
(FBN1), and Interleukin Receptor 4 (IL4R). Single
nucleotide polymorphisms (SNPs) were identified in COMP, COL9A1, COL9A2, and FBN1.
Based on chi-square analyses, there was no significant association between the SNPs and CR
status (affected and unaffected), although some
suggestion of an association was found between
COL9A1 (located on CFA 12) and CR affected
status (P = 0.10) (Wilke et al. 2005).
Another study evaluated microsatellite
markers closely located to the genes Collagen
Type 9 alpha 1, 2, and 3 (COL9A1, COL9A2,
and COL9A3) in a population of Boxers with a
high incidence of CR (Temwichitr et al. 2007).
Data arising from this study suggested that the
VetBooks.ir
Genetics of Cruciate Ligament Rupture
candidate genes were not related to CR
in the population studied. However, the
microsatellites they identified could be possible
candidates for other collagenopathies.
More recently, a candidate gene SNP genotyping approach was used to evaluate several
potential CR genes in high-risk breeds including the Newfoundland, Labrador Retriever,
Rottweiler, and Staffordshire Bull Terrier (Baird
et al. 2014a). Genes tested for association
included collagen genes: COL1A1, COL1A2,
COL3A1, COL5A1, COL5A2, COL5A3, COL6A1,
COL6A3, COL11A1, COL11A2, COL14A1, and
COL24A1; fibril/elastic fiber formation genes:
FMOD (fibromodulin), DCN (decorin), ELN
(elastin), OPTC (opticin), LTBP2 (latent transforming growth factor beta binding protein
2), and BGN (biglycan); extracellular matrix
genes: FBN1 (fibrillin 1), COMP (cartilage
oligomeric matrix protein), and ACAN (aggrecan); collagen-formation genes: SERPINH1 (serpin pertidase inhibitor clade H (heat shock protein 47) member 1 (collagen binding protein
1), PLOD1 (procollagen-lysine, 2-oxoglutarate
5-dehydrogenase), and LOX (lysyl oxidase); collagen cleavage genes: MMP1 (matrix metallopeptidase 1) and CTSK (cathepsin K); and
ligament/tendon/limb development gene SIX1
(SIX homeobox 1).
When breeds were analyzed separately, two
significant SNPs were identified: one in the
Labrador Retriever (corrected P < 0.001) and
one in the Rottweiler (corrected P = 0.02).
The SNP identified in Labrador Retrievers was
located within COL24A1. The SNP identified
in Rottweilers was initially considered to be
located within the elastin gene, but was remapped to an intergenic region when the
data were updated to the newest build of the
canine genome. When all breeds were considered together, three significant SNPs were
identified: two were located in COL5A1 and
the third was located within COL1A1. These
results suggest that collagen genes, particularly
COL24A1, COL5A1, and COL1A1, play some
role in CR pathogenesis. It is also important
to note that the associations on COL5A1 and
COL1A1 were shared across all four breeds.
This provides evidence that these mutations
occurred in the canine genome before breed
formation (Karlsson et al. 2008). The discovery of genetic mutations that are shared across
59
multiple breeds has the most potential for clinical impact.
Genome-wide association
Genome-wide association studies (GWAS) use
genetic markers across the entire set of DNA
for an individual (genome) to first identify a
chromosomal region that is associated with a
disorder, and then identify all genes located
in that region. The genes are then organized
by function and selected for further investigation according to possible involvement in
the development of the disease or trait being
investigated. Before the advent of commercial
SNP arrays, GWAS could be performed using
microsatellites (MSATs). A microsatellite is a
variable repeating segment of DNA, usually
found in a non-coding segment. Microsatellites can be highly polymorphic and very informative. However, recent advances in DNA
sequencing technology, computational hardware and bioinformatics have made SNP arrays
the tool of choice for GWAS.
Using microsatellites, a GWAS for CR was
performed using 90 Newfoundlands that were
selected for the GWAS based on their degree
of inter-relatedness and the statistical likelihood that they segregated into homozygous
unaffected and homozygous affected animals
(Macrossan et al. 2005). Age and other potential
contributors to the cause of CR were not considered in this analysis. A total of 495 MSATs was
used to compare genotypes and allele frequencies between CR-affected and unaffected dogs.
Four markers (located on four chromosomes)
were significant after the false discovery rate
was controlled at the 0.05 level using the Storey
and Tibshirani method (Storey & Tibshirani
2003; Wilke et al. 2009; Wilke 2010). The MSATs
were CPH19 located on chromosome 3, FH3702
on chromosome 5, REN147D07 located on chromosome 13, and FH3750 located on chromosome 24. Initial validation of the four markers
confirmed significance of three; canine chromosomes 3, 5, and 13. Positional candidate genes
located on chromosome 3 were sequenced for
mutation identification; Versican core protein
precursor (VCAN) and aggrecan core protein
precursor (cartilage-specific protein core protein;
CSPCP). Proteoglycans are major components
VetBooks.ir
60
Etiopathogenesis of Cruciate Ligament Rupture
of the extracellular matrix (ECM) of cartilage
(Schwartz & Domowicz 2002). A significant
association was identified with a SNP found in
CSPCP, but not VCAN, and the trait, suggesting
a role for aggrecan in CR pathogenesis.
More recently, an updated GWAS of CR was
performed in a population of Newfoundlands
using SNP genotyping (Baird et al. 2014b). Initially, 96 dogs (48 cases, 48 controls) were
genotyped using a SNP array with >170,000
SNP markers evenly spaced across the canine
genome. Clinical diagnoses were confirmed
by a veterinary surgeon. Control dogs were
defined as dogs over the age of 5 years with no
history of stifle injury, stifle instability, or pelvic
limb lameness. After quality control, the samples were analyzed using the Cochran–Mantel–
Haenszel (CMH) test as well as Efficient MixedModel Association Expedited (EMMAX) analysis. Both the CMH test and EMMAX are used
to correct for relatedness that may exist in the
population, an important step for canine GWAS
studies. The 65 most significant SNPs from this
analysis were re-genotyped in a larger group
of 271 Newfoundlands (96 from the preliminary GWAS and 175 new) using Sequenom
genotyping, and case-control association was
re-analyzed. Three main associations were identified on chromosomes 1, 3, and 33. The association on chromosome 1 included SNPs within
the RNF152 gene, the association on chromosome 3 included SNPs within the SORCS2 gene,
and the association on chromosome 33 included
SNPs within SEMA5B, DIRC2, and ZDHHC23.
SEMA5B, SORCS2, and ZDHHC23 all have various roles in the nervous system. Other nervous
system genes were also identified in regions
that did not maintain statistical significance
after correction for multiple testing. This provides evidence for the potential role of neurological pathways in CR disease risk. The authors
cited the importance of mechanoreceptors for
appropriate proprioception, as reduced proprioception may prevent appropriate response
to mechanical loading, placing the CrCL at
increased risk of matrix damage and fiber rupture (Baird et al. 2014b). These regions did not
overlap with the regions identified in the earlier
Newfoundland CR GWAS (Wilke et al. 2009).
Most recently, a GWAS of CR was performed
in another high-risk breed, the Labrador
Retriever (Baker et al. 2017). Purebred Labrador
Retrievers (237 dogs consisting of 98 cases,
139 controls) were genotyped using an array
with >170,000 SNPs evenly spaced across the
canine genome. Clinical diagnosis of CR was
confirmed by a veterinary surgeon. Controls
were over the age of 8 years (Reif & Probst
2003) with a normal orthopaedic examination.
Additionally, lateral standing stifle radiographs
were taken of all control dogs to confirm that
there were no signs of stifle pathology before
enrollment (Chuang et al. 2014). This level of
phenotyping is more stringent than in previous
studies (Wilke et al. 2009; Baird et al. 2014b).
After quality control, ∼119,000 SNPs remained
for linear mixed model association using two
algorithms, GEMMA (Zhou & Stephens 2012)
and GCTA (Yang et al. 2011), as well as Penalized Unified Multiple-locus Association using
PUMA (Hoffman et al. 2013). Genome-wide
significance was defined separately for each
algorithm using a permutation procedure
(Baker et al. 2017). To facilitate pathway analysis, an additional set of candidate loci was
identified with a cutoff of P < 5E-04 (Karlsson
et al. 2013), and results from all three algorithms
were combined. This approach identified 129
SNPs associated with CR. These SNPs were
grouped into 99 regions based on linkage
disequilibrium (r2 > 0.8).
One region containing two SNPs on chromosome 24 met genome-wide significance.
Nine genes were identified in this region
with diverse physiological effects on cellular and tissue homeostasis. These included
bactericidal/permeability-increased
protein
(BPI), lipopolysaccharide-binding protein
(LBP), Ral GTPase activation protein beta subunit (RALGAPB), adipogenin (ADIG), solute
carrier family 32, member 1 (SLC32A1), ARP5
actin-related protein 5 (ACTR5), protein phosphatase 1, regulatory subunit 16B (PPP1R16B),
family with sequence similarity 83, member
D (FAM83D), and DEAH (Asp-Glu-Ala-His)
box polypeptide 35 (DHX35). An additional 98
regions were identified at the candidate level.
All regions were combined for pathway analysis using DAVID (Huang et al. 2009). Pathway
analysis revealed an association with a cluster
of 11 genes encoding proteins with antimicrobial activity (corrected P = 0.02) and a cluster of
24 genes encoding carbohydrate-binding proteins (corrected P = 1.21E-04). Notably, the cluster of antimicrobial genes included LBP and BPI,
which were also present in the genome-wide
VetBooks.ir
Genetics of Cruciate Ligament Rupture
significant locus on chromosome 24. The majority of the carbohydrate-binding genes also had a
role in immune function as pattern-recognition
receptors. Of note, this cluster also included
aggrecan (ACAN), hyaluronan and proteoglycan link protein 3 (HAPLN3), also known as
cartilage link protein. Aggrecan and link protein are important for maintaining hydration in
collagenous tissues. Tissue hydration is important for the efficient distribution of mechanical
load and cellular repair. A link between aggrecan and canine CR is also supported by earlier
work (Wilke et al. 2009; Wilke 2010), which identified an association with a microsatellite within
aggrecan core protein precursor. The upregulation of aggrecan has also been associated
with human ACL rupture (Mannion et al. 2014;
Johnson et al. 2015), as well as equine degenerative suspensory ligament desmitis (DSLD),
a debilitating disorder of horses that leads to
collagen disruption and eventual rupture of the
suspensory ligament (Plaas et al. 2011).
While GWAS has most often been used for
the identification of candidate genes and biological pathways that may be contributing to
disease pathogenesis, this approach may also
be used to develop genomic prediction algorithms for genetic screening. Here, research is
less concerned with the biological effect of a
mutation tagged by a SNP, but instead focuses
on the statistical effect of a particular genotype and its ability to predict a disease outcome, often in combination with other SNP
genotypes. In a recent study, GWA was performed separately in a population of 46 Newfoundlands (22 cases and 24 controls) and 333
Labrador Retrievers (190 cases and 143 controls)
using a mixed linear model approach. Associated SNPs from GWAS were used to develop a
classification tree, which is a statistical method
that evaluates each SNP for its classifying ability and selects the best SNPs to create a classification model. In Newfoundlands, 19 SNPs
were used for diagnostic model assessment. The
model selected three SNPs for best classification. Cross-validation of the model yielded an
area under the receiver operator characteristic
(ROC) curve of 95.5%, indicating that the model
had a good ability to classify cases and controls
in the sample population. In Labrador Retrievers, 13 SNPs were used in the same procedure.
The diagnostic model selected all 13 SNPs for
best classification, with an area under the ROC
61
curve of 88.4%, indicating that the model was
also able to classify cases and controls in the
sample population, but slightly reduced compared to Newfoundland dogs (Wilke et al. 2015).
The SNPs identified in this GWAS did not overlap with regions identified in other Newfoundland or Labrador GWAS (Wilke et al. 2009; Baird
et al. 2014b; Baker et al. 2017). While the results
of these studies are promising, they should
not be over-interpreted as the population used
for GWAS was also used for diagnostic model
development and testing. A truly predictive
model must be tested in new populations that
were not used to train the model. Nevertheless,
these results speak to the concept that development of a genetic test for CR is an achievable
research goal, as accurate stratification of cases
and controls can be achieved (Wilke et al. 2015;
Baker et al. 2017).
Canine and human cruciate
ligament rupture
The young (human) female athlete is another
cohort that shares characteristics of the CR phenotype found in dogs. This cohort experiences
anterior cruciate ligament (ACL) injuries two to
eight fold more frequently than their counterpart young athletic males (Arendt & Dick 1995;
Gwinn et al. 2000; Lohmander et al. 2004). ACL
tears in people often involve contact trauma;
however, in this select population ACL rupture usually occurs via a non-contact mechanism (Arendt & Dick 1995).
Several studies have evaluated the potential
genetic contribution to ACL injuries in humans.
The first was a case-control study that found
those with an ACL injury to be twice as likely to
have had a family member with an ACL injury
as those study participants that did not have an
ACL injury (Flynn et al. 2005). Additionally, a
more recent study noted that individuals with
a first-degree relative with an ACL injury were
at 2.2 times greater risk of both graft rupture
and contralateral injury (Webster et al. 2014).
These findings support a familial predisposition
to ACL rupture.
Further research has targeted mutations in
collagen genes as risk factors for ACL injuries.
Two separate studies have evaluated a mutation (G1023T; rs1800012) in intron 1 of Collagen Type 1 alpha 1 (COL1A1), the binding site
VetBooks.ir
62
Etiopathogenesis of Cruciate Ligament Rupture
for the transcription factor Sp1, in relation to
ACL injury (Khoschnau et al. 2008; Posthumus
et al. 2009). Although the TT genotype was rare,
both studies concluded that the homozygous
TT genotype seemed to have a protective effect
on the development of ACL rupture. It is proposed that the increased binding of the Sp1
transcription factor increases the expression of
the alpha 1 chain, but it is unknown how this
protects against ACL injury. In another study,
female participants with an ACL injury were
2.4-fold more likely to have the AA homozygous genotype for the SNP (rs970547, S3058G)
in exon 65 of Collagen Type 12 alpha 1 (COL12A1)
(Posthumus et al. 2010). This finding was confirmed in a separate cohort (O’Connell et al.
2015). This study also reported an interaction
between the COL5A1 rs12722 and COL12A1
rs970547, such that individuals with the T+A–
pseudo-haplotype were at greater risk of experiencing ACL rupture (O’Connell et al. 2015).
Another candidate gene study identified an
association between matrix metalloproteinase
genes and ACL rupture, particularly MMP12
rs2276109, where the AA genotype is significantly more prevalent among individuals
with confirmed non-contact cruciate rupture
(Posthumus et al. 2012). Angiogenesis signaling may also play a role in ACL rupture risk,
as the VEGFA rs699947 CC genotype is also
significantly over-represented among individuals with non-contact ACL rupture (Rahim et al.
2014). Proteoglycans have also been identified
as a potential factor influencing the risk of ACL
rupture in human beings. Proteoglycans play
important roles in fibrillogenesis and ECM collagen. A candidate gene study identified loci in
ACAN (aggrecan) and DCN (decorin) that were
associated with ACL injury susceptibility (Mannion et al. 2014). A separate study evaluated
gene expression in biopsies taken from ruptured ACL ligament, and noted that the expression of ACAN was significantly upregulated in
female compared to male patients. This suggests that aggrecan may be playing a role in the
observed sex-related differences regarding susceptibility to ACL rupture (Johnson et al. 2015).
Summary and future recommendations
The combined results of these studies suggest that canine CR is a moderately heritable
(Nielen et al. 2001; Wilke et al. 2006; Baker
et al. 2017), highly polygenic complex trait disease. Biological networks that control collagen
genes (Wilke et al. 2005; Baird et al. 2014b),
neurologic pathways (Baird et al. 2014a), innate
immune mechanisms (Baker et al. 2017), and
aggrecan signaling (Wilke et al. 2009; Wilke
2010; Baker et al. 2017) may all play a role in
CR pathogenesis and warrant further investigation. The overlap between the results of canine,
equine, and human discovery research implicating aggrecan in susceptibility to ACL rupture
makes ACAN a particularly interesting target
for further genetic investigation. Given the complex nature of this condition, further investigation of mutations with larger effects will likely
require a combination of high-powered GWAS
with large sample sizes and next-generation
sequencing.
A genetic test for CR is possible and should
remain a goal of current research efforts. Genotyping dogs at individual loci is not likely to
be predictive, as individual genetic mutations
most likely contribute small amounts to phenotypic variance. A predictive test for CR is more
likely to resemble genomic prediction methods
commonly employed in animal and dairy science (Vazquez et al. 2012). These approaches
consider the additive effect of all non-null-effect
SNPs, which may be used to develop a genetic
risk assessment tool.
The comparative value of the canine model
for complex trait disease has received much
attention during recent years (Karlsson &
Lindblad-Toh 2008; Shearin & Ostrander 2010;
Hayward et al. 2016; van Steenbeek et al. 2016).
There are many similarities between canine CR
and human ACL rupture. It is very likely that
advances made in understanding how genetic
variants may affect biological pathways that
influence disease risk in the dog will lead to
similar advancements in the understanding and
treatment of ACL rupture in human beings.
References
Arendt E, Dick R. Knee injury patterns among men
and women in collegiate basketball and soccer.
NCAA data and review of literature. Am J Sports
Med 1995;23:694–701.
Baird AEG, Carter SD, Innes JF, et al. Genetic basis of
cranial cruciate ligament rupture (CCLR) in dogs.
Connect Tissue Res, 2014a;55;275–281.
VetBooks.ir
Genetics of Cruciate Ligament Rupture
Baird AEG, Carter SD, Innes JF, et al. Genome-wide
association study identifies genomic regions of
association for cruciate ligament rupture in Newfoundland dogs. Anim Genet 2014b;45:542–549.
Baker LA, Kirkpatrick B, Rosa GJM, et al. Genomewide association analysis in dogs implicates 99 loci
as risk variants for anterior cruciate ligament rupture. PLoS One 2017;12;e0173810.
Chuang C, Ramaker MA, Kaur S, et al. Radiographic
risk factors for contralateral rupture in dogs with
unilateral cranial cruciate ligament rupture. PLoS
One 2014;9:e106389.
Flynn RK, Pedersen CL, Birmingham TB, et al. The
familial predisposition toward tearing the anterior
cruciate ligament. Am J Sports Med 2005;33:23–28.
Guthrie JW, Keeley BJ, Maddock E, et al. Effect of
signalment on the presentation of canine patients
suffering from cranial cruciate ligament disease.
J Small Anim Pract 2012;53:273–277.
Gwinn DE, Wilckens JH, McDevitt ER, et al. The relative incidence of anterior cruciate ligament injury
in men and women at the United States Naval
Academy. Am J Sp Med 2000;28:98–102.
Harasen G. Canine cranial cruciate ligament rupture
in profile: 2002–2007. Canadian Vet J 2008;49:193–
194.
Hayward JJ, Castelhano MG, Oliveira KC, et al. Complex disease and phenotype mapping in the domestic dog. Nat Commun 2016;7:10460.
Hoffman, GE, Logsdon BA, Mezey JG. PUMA: A
unified framework for penalized multiple regression analysis of GWAS data. PLoS Comput Biol
2013;9:p.e1003101.
Huang DW, Sherman BT, Lempicki RA. Bioinformatics enrichment tools: paths toward the comprehensive functional analysis of large gene lists. Nucleic
Acids Res 2009;37:1–13.
Johnson JS, Morscher MA, Jones KC, et al. Gene
expression differences between ruptured anterior
cruciate ligaments in young male and female subjects. J Bone Joint Surg 2015;97:71–79.
Karlsson EK, Lindblad-Toh K. Leader of the pack:
gene mapping in dogs and other model organisms.
Nat Rev Genet 2008;9:713–725.
Karlsson EK, Sigurdsson S, Ivansson E, et al. Genomewide analyses implicate 33 loci in heritable dog
osteosarcoma, including regulatory variants near
CDKN2A/B. Genome Biol 2013;14:R132.
Khoschnau S, Melhus H, Jacobson A, et al. Type 1 collagen α1 Sp1 polymorphism and the risk of cruciate
ligaments ruptures or shoulder dislocations. Am J
Sports Med 2008;36:2432–2436.
Lohmander LS, Ostenberg A, Englund M, et al.
High prevalence of knee osteoarthritis, pain, and
functional limitations in female soccer players
twelve years after anterior cruciate ligament injury.
Arthritis Rheum 2004;50:3145–3152.
Macrossan PE, Kinghorn BP, Wilke VL, et al. Selective genotyping for determination of a major gene
associated with cranial cruciate ligament disease in
63
the Newfoundland dog. Proc Assoc Adv Animal
Breeding Genet 2005;16:346–349.
Mannion S, Mtintsilana A, Posthumus M, et al. Genes
encoding proteoglycans are associated with the
risk of anterior cruciate ligament ruptures. Br J
Sports Med 2014;48:1640–1646.
Nielen AL, Janss LLG, Knol BW. Heritability estimations for diseases, coat color, body weight, and
height in a birth cohort of Boxers. Am J Vet Res
2001;62:1198–1206.
O’Connell K, Knight H, Ficek K, et al. Interactions
between collagen gene variants and risk of anterior cruciate ligament rupture. Eur J Sport Sci
2015;15:341–350.
Pérez P, de los Campos G. Genome-wide regression
and prediction with the BGLR statistical package.
Genetics 2014;198:483–495.
Plaas A, Sandy J, Liu H, et al. Biochemical identification and immunolocalizaton of aggrecan,
ADAMTS5 and inter-alpha-trypsin-inhibitor in
equine degenerative suspensory ligament desmitis. J Orthop Res 2011;29:900–906.
Posthumus M, September AV, Keegan M, et al.
Genetic risk factors for anterior cruciate ligament
ruptures: COL1A1 gene variant. Br J Sports Med
2009:43:352–356.
Posthumus M, September AV, O’Cuinneagain D, et al.
The association between the COL12a1 gene and
anterior cruciate ligament ruptures. Br J Sports
Med 2010;44:1160–1165.
Posthumus M, Collins M, van der Merwe L, et al.
Matrix metalloproteinase genes on chromosome
11q22 and the risk of anterior cruciate ligament
(ACL) rupture. Scand J Med Sci Sports 2012;22:523–
533.
Rahim M, Gibbon A, Hobbs H, et al. The association
of genes involved in the angiogenesis-associated
signaling pathway with risk of anterior cruciate ligament rupture. J Orthop Res 2014;32:1612–
1618.
Reif U, Probst CW. Comparison of tibial plateau
angles in normal and cranial cruciate deficient stifles of Labrador Retrievers. Vet Surg 2003;32:385–
389.
Robinson MR, Wray NR, Visscher PM. Explaining additional genetic variation in complex traits.
Trends Genet 2014;30:124–132.
Schwartz NB, Domowicz M. Chondrodysplasias due
to proteoglycan defects. Glycobiology 2002;12:57–
68.
Shearin AL, Ostrander EA. Leading the way: canine
models of genomics and disease. Dis Model Mech
2010;3:27–34.
Storey JD, Tibshirani R. Statistical significance for
genomewide studies. Proc Natl Acad Sci USA
2003;100:9440–9445.
Tabor HK, Risch NJ, Myers RM. Candidate-gene
approaches for studying complex genetic traits:
practical considerations. Nat Rev Genet 2002;3:
391–397.
VetBooks.ir
64
Etiopathogenesis of Cruciate Ligament Rupture
Temwichitr J, Hazewinkel AW, van Hagen MA,
et al. Polymorphic microsatellite markers for
genetic analysis of collagen genes in suspected
collagenopathies in dogs. J Vet Med A 2007;54:522–
526.
van Steenbeek FG, Hytonen MK, Leegwater PAJ, et al.
The canine era: the rise of a biomedical model.
Anim Genet 2016;47:519–527.
Vazquez AI, de los Campos G, Klimentidis YC, et al.
A comprehensive genetic approach for improving
prediction of skin cancer risk in humans. Genetics
2012;192:1493–1502.
Webster KE, Feller JA, Leigh WB, et al. Younger
patients are at increased risk for graft rupture and
contralateral injury following anterior cruciate ligament reconstruction surgery. Am J Sports Med
2014;42;641–647.
Wilke VL, Conzemius MG, Kinghorn BP, et al. Inheritance of rupture of the cranial cruciate ligament
in Newfoundlands. J Am Vet Med A 2006;228:
61–64.
Wilke VL, Conzemius MC, Rothschild MF. SNP
detection and association analyses of candidate
genes for rupture of the cranial cruciate ligament
in the dog. Anim Genet 2005;36:519–521.
Wilke VL, Zhang S, Evans RB, et al. Identification of
chromosomal regions associated with cranial cruciate ligament rupture in a population of Newfoundlands. Am J Vet Res 2009;70:1013–1017.
Wilke VL. Genetics of cruciate ligament rupture.
Advances in The Canine Cranial Cruciate Ligament.
P Muir, editor. Wiley Blackwell. 2010, pp. 53–58.
Wilke VL, Zaldivar-Lopez S, Ekenstedt K, et al. Genotype influences risk of cranial cruciate ligament disease in the Newfoundland and Labrador retriever
breeds. J Vet Med Res 2015;2:1028.
Yang J, Lee H, Goddard ME, Visscher PM. GCTA: A
tool for genome-wide complex trait analysis. Am J
Hum Genet 2011;88:76–82.
Zhou X, Stephens M. Genome-wide efficient mixedmodel analysis for association studies. Nat Genet
2012;44:821–824.
VetBooks.ir
8
Cruciate Ligament Matrix
Metabolism and Development
of Laxity
Eithne Comerford
Introduction
Cruciate ligaments are comprised of cells and
extracellular matrix (ECM). Most skeletal ligaments contain approximately 60–80% water,
while nearly 70–80% of the dry weight of ligament is collagen (Frank et al. 1985). Up to 90%
of the ligamentous collagens is type I collagen,
the principle tensile-resistant fiber, but smaller
quantities of types III, V, and VI are also present
(Waggett et al. 1996). Smaller proportions of
matrix are composed of elastin, proteoglycans
and other biochemical substances such as DNA
from cells, enzymes, glycoproteins, lipoproteins
and integrins (Frank et al. 1985; Amiel et al. 1995;
Smith et al. 2014; Kharaz et al. 2016; Ruschke et al.
2016).
The majority of cells in ligaments are fibroblasts (sometimes referred to as ligamentocytes)
(Vasseur et al. 1985), although fibrocartilage
cells are present at attachment sites. The fibroblasts have multiple small cellular processes or
microvilli which may alter in cruciate ligaments
from dog breeds with differing risk of cruciate
ligament rupture (CR) (Smith et al. 2012) (Figure 8.1). The cells are linked both within the
same row and in adjacent rows by connexins,
allowing a three-dimensional communicating
network that extends throughout the ligament
(Benjamin & Ralphs 1998).
The mechanical properties of cruciate ligaments are dependent on the composition and
structure of the ECM, in particular collagen.
Collagen turnover is a balance between its
synthesis and degradation (Cawston 1998). To
date, most interest in cruciate ligament ECM
metabolism has centered on degradation (Comerford et al. 2005; Hasegawa et al. 2013; Nakahara et al. 2013). However, some research has
been conducted into the synthesis of ECM components (e.g., collagen) in ligament, by measuring terminal propeptide levels (Sluss et al.
2001; Quasnichka et al. 2005), but this has yet to
be evaluated in the canine cranial cruciate ligament (CrCL). The synthesis of ECM components after mechanical load has been evaluated
in canine CrCL cells (Breshears et al. 2010a).
Proteases, such as the cathepsins (Muir et al.
2002; Barrett et al. 2005; Muir et al. 2005a,b)
and matrix metalloproteinases (MMPs; collagenases, stromelysins, and gelatinases) (Muir et al.
2005a,b; Comerford et al. 2006; Breshears et al.
2010b) have been mainly implicated in ECM
degradation.
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
65
Etiopathogenesis of Cruciate Ligament Rupture
VetBooks.ir
66
Figure 8.1 Confocal microscopy images of canine cranial cruciate ligament (CrCL) cellular matrix. Greyhound CrCL
longitudinal sections. Vimentin and α-tubulin immunohistochemistry (green) with DAPI for nuclear staining (blue). Scale
bars = 50 μm. (A) Interfascicular region showing dense cellularity with multiple branching processes. (B) Type A cells
with thin longitudinal processes of moderate length and minimal branching. (C) Type B cells showing shorter thicker
processes with branching. (D) Type C cell morphology showing rounded nuclei and an absence of processes. Source:
Smith et al. 2012. Reproduced with permission from Elsevier.
VetBooks.ir
Cruciate Ligament Matrix Metabolism and Development of Laxity
Cruciate ligament metabolism and
laxity in human beings and other
species
Ligament metabolism may affect ligament
strength, and it has been suggested that
upregulated anterior cruciate ligament (ACL)
remodeling may predispose women to ACL
injury (Foos et al. 2001). Hormonal factors
have been shown to play an important role in
ligament metabolism and increased anterior
knee laxity (Park et al. 2009). In a systematic
review (Hewett et al. 2007), it was demonstrated
that women were at risk for ACL injuries in
the first half or pre-ovulatory phase of their
menstrual cycle, with one recent study advising
that female athletes should not exercise aggressively during this part of their cycle (Stijak et al.
2015). Estrogen and progesterone appear to
influence collagen metabolism in both animal
models and human beings. Estrogen (i.e., estradiol) has been shown to decrease fibroblast
proliferation and type I pro-collagen, whereas
progesterone counterbalances the inhibitory
effect of estrogen on female ACLs (Yu et al.
1999). Estrogen-primed ACL cells are also very
responsive to relaxin, decreasing collagen type
I and III gene expression as well increasing
the expression of degradative enzymes such as
MMP-1 and 3 (Konopka et al. 2016).
Most studies concerning knee laxity have
been conducted on the ACL, and most have
involved ex vivo cadaveric testing. Ex vivo,
varus–valgus laxity and angulation is increased
greatly by sectioning the collateral ligaments
(Markolf et al. 1976). Anterior–posterior stability is affected by the transection of most ligaments, with ACL sectioning showing the greatest increase at full joint extension (Markolf et al.
1976). Varus–valgus and anteroposterior laxity
is thought to be an important contributor in the
pathogenesis of human knee arthritis (Sharma
et al. 1999). Increased laxity may contribute to
abnormal knee biomechanics and abnormally
distributed joint loads that likely lead to or
accelerate arthritis.
Increased knee laxity was demonstrated in
the ovulatory or post-ovulatory phases of the
female menstrual cycle (Zazulak et al. 2006; Park
et al. 2009; Lee et al. 2013). A significantly higher
anterior–posterior joint laxity and hyperextension has been identified in non-contact ACL
67
injury in females compared to males (Uhorchak
et al. 2003). Although studies have examined the
effects of sex hormones on ACL metabolism,
there are few reports of normal ACL ECM
remodeling/degradation and its relationship to
joint laxity.
It has been suggested that increased collagen remodeling of the normal guinea pig ACL
by gelatinases (MMP-2 and MMP-9) may contribute to ligament and, therefore, knee joint laxity (Quasnichka et al. 2005). Increased remodeling was demonstrated in CrCLs from a strain
of guinea pigs predisposed to the development
of spontaneous arthritis (i.e., Dunkin Hartley) at
12 weeks compared to a control strain (i.e., Bristol Strain-2). All of the biochemical and mechanical changes in the predisposed CrCLs occurred
before subchondral bone and cartilage changes
at 24 weeks (Anderson-MacKenzie et al. 2005).
These studies suggest that increased remodeling of the CrCL may contribute to ligament and,
therefore, knee joint laxity.
Canine cruciate ligament metabolism
and laxity
Introduction
Most interest in ECM degradation of canine
articular tissue has centered on the MMPs
(collagenases, stromelysins and gelatinases),
cathepsins (serine, cysteine and aspartic proteases), and the ADAMTs family of enzymes.
The MMPs are regulated by several natural
inhibitors, such as the tissue inhibitors of metalloproteinases (TIMPs) and α2 -macroglobulin,
in order to prevent excessive activity and resulting matrix degradation.
The collagenases (MMP-1, -8, and -13) (which
cleave the fibrillar collagens at a specific
site within their helical domain, generating
3/4 and 1/4 fragments) have been demonstrated in normal and in experimental arthritic
canine cartilage (Fernandes et al. 1998). The
stromelysins (MMP-3 and -10) and gelatinases
(MMP-2 and -9) have been identified in canine
synovial fluid associated with experimentally
induced and rheumatoid arthritis, respectively
(Coughlan et al. 1998; Panula et al. 1998).
Increased concentrations of the N-terminal
(393) Alanine-Arginine-Glycine-Serine (ARGS)
neoepitope (or ARGS-aggrecan), a breakdown
product of cartilage, have been found to be elevated in human synovial fluid after acute ACL
injury. An increase in TIMP-3 at six months
after the injury was reported, suggesting an
inhibitory effect on further cartilage degradation (Tourville et al. 2015). However, little attention has been centered on the presence and
expression of these proteases in the normal
canine CrCL.
The role that the CrCL plays in the mechanical integrity of the canine stifle joint has been
well described (Stouffer et al. 1983; Vasseur
1993; Wingfield et al. 2000). Excessive motion
of the canine stifle joint is prevented by ligamentous constraints (the CrCL primarily resisting cranial tibial displacement) and a complex
system of reflex arcs from surrounding muscle groups (Vasseur & Arnoczky 1981; Vasseur
1993). Although the joint capsule has also been
shown to contribute significantly to craniocaudal stability in the canine stifle, the role of
the CrCL surpasses this contribution (Lopez
et al. 2003).
Metabolism in ruptured canine cruciate
ligaments
ECM metabolism in ruptured canine CrCLs
has been investigated (Muir et al. 2002; Comerford et al. 2004). In one study (Comerford et al.
2004), CrCLs from normal Labrador Retrievers,
a breed at high-risk of CR, and from Labrador
Retrievers with CR were examined. Ruptured
CrCLs had significantly higher amounts of
immature crosslinks, total and sulfated glycosoaminoglycans (GAGs), and water content,
compared with that of the intact ligaments.
Compared with intact CrCLs, the concentration of pro-MMP-2 (inactive MMP-2) was significantly higher, and the maximum temperature of collagen denaturation was significantly
lower in the ruptured CrCLs (Figures 8.2 and
8.3) (Comerford et al. 2004). These studies suggested that the ECM of ruptured CrCLs had
an increased matrix turnover, as indicated by a
higher collagen and GAG synthesis, compared
with that of intact CrCLs. It is likely that the
ECM changes may have occurred before ligament rupture. However, it is possible that these
observed changes may form part of a reparative
Percentage of MMP-2 standard
Etiopathogenesis of Cruciate Ligament Rupture
300
p = 0.02
200
100
0
Ruptured CrCLs
Intact CrCLs
Figure 8.2 Dot diagram of the pro-form of matrix
metalloproteinase 2 (pro-MMP-2) as a percentage of the
MMP-2 standard indicative of collagen remodeling in
seven ruptured and 11 intact cranial cruciate ligaments
(CrCLs) from 18 dogs. Horizontal lines represent the
mean values of each data set. Source: Comerford et al.
2004. Reproduced with permission from the American
Veterinary Medical Association.
process after rupture. Interestingly, the opposite was found recently in ruptured human
ACLs, compared to non-ruptured ACLs, with
a reduction in collagen and proteoglycans content noted. The authors suggested that these
changes occurred before or very soon after
rupture. However, the non-ruptured ligaments
were collected from aged donors during total
knee replacement, and may not indicate normal
ECM levels (Young et al. 2011).
Ruptured CrCLs also contain greater numbers of cells with the proteinases TRAP and
75.0
Temperature (°C)
VetBooks.ir
68
p = 0.004
72.5
70.0
67.5
65.0
Ruptured CrCLs
Intact CrCLs
Figure 8.3 Dot diagram of the maximum temperature of
denaturation determined via differential scanning
calorimetry in eight ruptured and 11 intact cranial
cruciate ligaments (CrCLs) from 19 dogs. Horizontal lines
represent the mean values of each data set. Source:
Comerford et al. 2004. Reproduced with permission from
the American Veterinary Medical Association.
VetBooks.ir
Cruciate Ligament Matrix Metabolism and Development of Laxity
69
cathepsin K, when compared with CrCLs from
healthy, young, or aged dogs (Muir et al.
2002). Therefore, cell-signaling pathways that
regulate expression of these proteinases may
form part of the mechanism that leads to upregulation of collagen remodeling within the
CrCL (Muir et al. 2002). Levels of cathepsin
K and tartrate-resistant protein (TRAP) expression in the canine synovium and CrCL were also
found to be significantly correlated in dogs with
CR (Muir et al. 2005a).
The relationship of cruciate ligament
metabolism and stifle laxity
Detailed comparisons of joint laxity and other
mechanical parameters in stifle joints with normal CrCLs with other ligament parameters
(e.g., collagen and ECM biochemistry) have
been reported infrequently (Vasseur et al. 1985).
The latter authors compared the biomechanical and histological properties in dogs, and
found a positive relationship with age, increasing weight, and degenerative changes in the
canine CrCL (Vasseur et al. 1985). However, only
a mixed population of dogs of different breeds,
ages, gender, and weight was examined in this
study.
The present authors’ group hypothesized
that increased cranio-caudal stifle joint laxity
would be present in normal stifle joints from a
breed at high risk of developing CR (Labrador
Retriever), compared to a low-risk breed (Greyhound). It was also hypothesized that the stifle
joints with increased cranio-caudal laxity (highrisk breeds) would demonstrate increased ECM
metabolism of their CrCLs. This increased ECM
metabolism could result in reduced ligament
strength and increased joint laxity contributing
to eventual ligament rupture.
Mechanical, biochemical and thermal analyses were used to test the above hypothesis (Comerford 2002; Comerford et al. 2005).
Mechanical analyses involved the measurement of cranio-caudal laxity and tensile testing of the CrCL. Ex vivo mechanical testing
of the stifles from both high- and low-risk
breeds was performed as previously described
(Amis & Dawkins 1991). The stifle joints were
mounted in two different test positions (30◦
and 90◦ of flexion) (Figure 8.4), after which the
Figure 8.4 Photograph of a canine stifle joint positioned
in a materials testing machine (Instron 1122, Instron Ltd,
High Wycombe, UK) for cranio-caudal mechanical
testing. The tibia is positioned in the uppermost stainless
steel pot and the load cell is positioned to the top of the
picture.
CrCL dimensions were measured and the ligaments tested to failure (Woo et al. 1991). Biochemical and thermal analyses to assess ECM
metabolism, such as collagen crosslink analysis, gelatin and reverse gelatin zymography
(to measure MMPs and TIMPs, respectively),
total and sulfated GAGs, and differential scanning calorimetry, were performed on the CrCLs
from the stifles which had undergone mechanical testing. Cranio-caudal laxity measurements
showed the mean tibial displacements of the
Labrador Retriever stifle joints to be significantly greater than those of the Greyhound stifle joints at 30◦ and 90◦ of flexion, indicating
increased laxity within the high-risk stifle joints
(Figure 8.5) (Comerford et al. 2005). There was a
significantly higher expression of pro-MMP-2 in
the high-risk CrCLs (Labrador Retrievers) compared to the low-risk (Greyhound) CrCLs (Figure 8.6). Higher pro-MMP-2 levels can be associated with increased collagen turnover, though
this was not confirmed by changes in immature
collagen crosslinks in this study. The concentrations of pro-MMP-2 had a positive correlation (r = 0.5, P = 0.02) with cranio-caudal laxity at 90◦ , once both dog groups were combined.
The enthalpy of collagen denaturation (indicating the amount of heat required to denature the
collagen triple helices) was significantly lower
in the Labrador CrCLs, compared to that of
Etiopathogenesis of Cruciate Ligament Rupture
p = 0.04
p = 0.04
100
CC Laxity (mm)
(Mean+/– SEM)
**
5.0
*
*
**
2.5
0.0
30
30
90
Knee joint flexion (°)
Greyhound
Labrador Retriever
75
p = 0.02
50
25
Greyhound
Labrador Retriever
Figure 8.6 Levels of pro-MMP-2 (% inactive zymogen)
in Labrador Retriever and Greyhound cranial cruciate
ligaments. Source: Comerford et al. 2005. Reproduced
with permission from John Wiley & Sons, Inc.
Greyhounds (Figure 8.7). This implies the
presence of partially degraded collagen triple
helices in Labrador CrCLs. Increased collagen
degradation, as indicated by the high levels of
MMP-2, is consistent with the thermal properties of the collagenous matrix of the Labrador
CrCL, as well as the increased stifle joint laxity
within this breed. Interestingly, gender or bodyweight did not correlate significantly with any
of the mechanical, biochemical, or thermal analyses in this study.
Conclusions
Differences in cruciate ligament metabolism
(ACL and CrCL) indicated by greater MMP-2
expression and collagen denaturation are
p = 0.05
75
50
25
0
90
Figure 8.5 Cranio-caudal (CC) laxity testing in
Greyhounds (n = 11) and Labrador Retrievers (n = 11) at
100 N with the joint in 30◦ and 90◦ of flexion. Source:
Comerford et al. 2005. Reproduced with permission from
John Wiley & Sons, Inc.
0
Enthalpy (J/g collagen)
(Mean+/– SEM)
7.5
Expression of
pro-MMP–2 (% std)
(Mean+/– SEM)
VetBooks.ir
70
Greyhounds Labrador Retrievers
Figure 8.7 The enthalpy of denaturation (J/g collagen)
of the differential scanning calorimetry thermograms from
Labrador Retriever and Greyhound cranial cruciate
ligaments. Source: Comerford et al. 2005. Reproduced
with permission from John Wiley & Sons, Inc.
consistent with identified mechanical properties in guinea pigs and dogs. The ligaments
examined in these studies had no apparent
pathology and, therefore, the changes identified may be intrinsic to ligament metabolism.
This may be related to genetics (influencing
factors such as stifle joint morphology), and
may account for the differing breed predisposition to CR within these two species. Therefore,
subtle changes in cruciate ligament metabolism
and its influence on joint mechanics may play a
role in canine CrCL, and possibly human, ACL
rupture.
References
Amiel D, Chu CR, Lee J. Effect of loading on
metabolism and repair of tendons and ligaments.
Repetitive motion disorders of the upper extremity. S Gordon, Blair, SJ, Fine, LJ, eds. Rosemount,
IL, American Academy of Orthopaedic Surgeons,
1995. pp. 217–230.
Amis AA, Dawkins GP. Functional anatomy of the
anterior cruciate ligament. Fibre bundle actions
related to ligament replacements and injuries.
J Bone Joint Surg Br 1991;73:260–267.
Anderson-MacKenzie JM, Quasnichka HL, Starr RL,
et al. Fundamental subchondral bone changes in
spontaneous knee osteoarthritis. Int J Biochem Cell
Biol 2005;37:224–236.
Barrett JG, Hao Z, Graf BK, et al. Inflammatory changes in ruptured canine cranial and
human anterior cruciate ligaments. Am J Vet Res
2005;66:2073–2080.
Benjamin M, Ralphs JR. Fibrocartilage in tendons and
ligaments – an adaptation to compressive load.
J Anat 1998;193:481–494.
VetBooks.ir
Cruciate Ligament Matrix Metabolism and Development of Laxity
Breshears LA, Cook JL, Stoker AM, et al. The effect
of uniaxial cyclic tensile load on gene expression
in canine cranial cruciate ligamentocytes. Vet Surg
2010a;39:433–443.
Breshears LA, Cook JL, Stoker AM, et al. Detection and evaluation of matrix metalloproteinases
involved in cruciate ligament disease in dogs using
multiplex bead technology. Vet Surg 2010b;39:306–
314.
Cawston T. Matrix metalloproteinases and TIMPs:
properties and implications for the rheumatic diseases. Mol Med Today 1998;4:130–137.
Comerford E. Evaluation of extracellular matrix composition, metabolism, joint mechanics and joint
conformation as potential predisposing factors of
cranial cruciate ligament rupture in three dog
breeds. Thesis, Doctor of Philosophy, University of
Bristol, 2002.
Comerford EJ, Innes JF, Tarlton JF, et al. Investigation
of the composition, turnover, and thermal properties of ruptured cranial cruciate ligaments of dogs.
Am J Vet Res 2004;65:1136–1141.
Comerford EJ, Tarlton JF, Avery NC, et al. Distal
femoral intercondylar notch dimensions and their
relationship to composition and metabolism of the
canine anterior cruciate ligament. Osteoarthritis
Cartilage 2006;14:273–278.
Comerford EJ, Tarlton JF, Innes JF, et al. Metabolism
and composition of the canine anterior cruciate ligament relate to differences in knee joint mechanics
and predisposition to ligament rupture. J Orthop
Res 2005;23:61–66.
Coughlan AR, Robertson DH, Bennett D, et al. Matrix
metalloproteinases 2 and 9 in canine rheumatoid
arthritis. Vet Rec 1998;143:219–223.
Fernandes JC, Martel-Pelletier J, Lascau-Coman V,
et al. Collagenase-1 and collagenase-3 synthesis
in normal and early experimental osteoarthritic
canine cartilage: an immunohistochemical study.
J Rheumatol 1998;25:1585–1594.
Foos MJ, Hickox JR, Mansour PG, et al. Expression of
matrix metalloprotease and tissue inhibitor of metalloprotease genes in human anterior cruciate ligament. J Orthop Res 2001;19:642–649.
Frank C, Amiel D, Woo SL, et al. Normal ligament
properties and ligament healing. Clin Orthop Relat
Res 1985:15–25.
Hasegawa A, Nakahara H, Kinoshita M, et al. Cellular and extracellular matrix changes in anterior
cruciate ligaments during human knee aging and
osteoarthritis. Arthritis Res Ther 2013;15:R29.
Hewett TE, Zazulak BT, Myer GD. Effects of the
menstrual cycle on anterior cruciate ligament
injury risk: a systematic review. Am J Sports Med
2007;35:659–668.
Kharaz YA, Tew SR, Peffers M, et al. Proteomic differences between native and tissue-engineered tendon and ligament. Proteomics 2016;16:1547–1556.
Konopka JA, DeBaun MR, Chang W, et al. The intracellular effect of relaxin on female anterior cruciate
71
ligament cells. Am J Sports Med 2016;44:
2384–2392.
Lee H, Petrofsky JS, Daher N, et al. Anterior cruciate ligament elasticity and force for flexion during
the menstrual cycle. Med Sci Monit 2013;19:1080–
1088.
Lopez MJ, Kunz D, Vanderby R, Jr, et al. A comparison of joint stability between anterior cruciate
intact and deficient knees: a new canine model of
anterior cruciate ligament disruption. J Orthop Res
2003;21:224–230.
Markolf KL, Mensch JS, Amstutz HC. Stiffness and
laxity of the knee – the contributions of the supporting structures. A quantitative in vitro study. J Bone
Joint Surg Am 1976;58:583–594.
Muir P, Hayashi K, Manley PA, et al. Evaluation of
tartrate-resistant acid phosphatase and cathepsin K
in ruptured cranial cruciate ligaments in dogs. Am
J Vet Res 2002;63:1279–1284.
Muir P, Danova NA, Argyle DJ, et al. Collagenolytic
protease expression in cranial cruciate ligament
and stifle synovial fluid in dogs with cranial cruciate ligament rupture. Vet Surg 2005a;34:482–490.
Muir P, Schamberger GM, Manley PA, et al. Localization of cathepsin K and tartrate-resistant acid
phosphatase in synovium and cranial cruciate ligament in dogs with cruciate disease. Vet Surg
2005b;34:239–246.
Nakahara H, Hasegawa A, Otabe K, et al. Transcription factor Mohawk and the pathogenesis
of human anterior cruciate ligament degradation.
Arthritis Rheum 2013;65:2081–2089.
Panula HE, Lohmander LS, Ronkko S, et al. Elevated
levels of synovial fluid PLA2, stromelysin (MMP3) and TIMP in early osteoarthrosis after tibial valgus osteotomy in young beagle dogs. Acta Orthop
Scand 1998;69:152–158.
Park SK, Stefanyshyn DJ, Loitz-Ramage B, et al.
Changing hormone levels during the menstrual
cycle affect knee laxity and stiffness in healthy
female subjects. Am J Sports Med 2009;37:588–598.
Quasnichka HL, Anderson-MacKenzie JM, Tarlton
JF, et al. Cruciate ligament laxity and femoral
intercondylar notch narrowing in early-stage knee
osteoarthritis. Arthritis Rheum 2005;52:3100–3109.
Ruschke K, Meier C, Ullah M, et al. Bone morphogenetic protein 2/SMAD signalling in human
ligamentocytes of degenerated and aged anterior cruciate ligaments. Osteoarthritis Cartilage
2016;24:1816–1825.
Sharma L, Lou C, Felson DT, et al. Laxity in
healthy and osteoarthritic knees. Arthritis Rheum
1999;42:861–870.
Sluss JR, Liberti JP, Jiranek WA, et al. pN collagen type
III within tendon grafts used for anterior cruciate
ligament reconstruction. J Orthop Res 2001;19:852–
857.
Smith KD, Clegg PD, Innes JF, et al. Elastin content is
high in the canine cruciate ligament and is associated with degeneration. Vet J 2014;199:169–174.
VetBooks.ir
72
Etiopathogenesis of Cruciate Ligament Rupture
Smith KD, Vaughan-Thomas A, Spiller DG, et al. Variations in cell morphology in the canine cruciate ligament complex. Vet J 2012;193:561–566.
Stijak L, Kadija M, Djulejic V, et al. The influence of
sex hormones on anterior cruciate ligament rupture: female study. Knee Surg Sports Traumatol
Arthrosc 2015;23:2742–2749.
Stouffer DC, Butler DL, Kim H. Tension–torsion characteristics of the canine anterior cruciate ligament
– Part I: Theoretical framework. J Biomech Eng
1983;105:154–159.
Tourville TW, Poynter ME, DeSarno MJ, et al. Relationship between synovial fluid ARGS-aggrecan
fragments, cytokines, MMPs, and TIMPs following
acute ACL injury: A cross-sectional study. J Orthop
Res 2015;33:1796–1803.
Uhorchak JM, Scoville CR, Williams GN, et al. Risk
factors associated with noncontact injury of the
anterior cruciate ligament: a prospective four-year
evaluation of 859 West Point cadets. Am J Sports
Med 2003;31:831–842.
Vasseur P. Stifle joint. In: Textbook of Small Animal
Surgery. Slatter D, ed. New York, WB Saunders,
1993. pp. 1817–1867.
Vasseur PB, Arnoczky SP. Collateral ligaments of the
canine stifle joint: anatomic and functional analysis. Am J Vet Res 1981;42:1133–1137.
Vasseur PB, Pool RR, Arnoczky SP, et al. Correlative biomechanical and histologic study of the
cranial cruciate ligament in dogs. Am J Vet Res
1985;46:1842–1854.
Waggett A, Kwan A, Woodnutt D. Collagens in
fibrocartilages at the Achilles tendon insertion –
a biochemical, molecular biological and immunohistochemical study. Trans Orthop Res Soc 1996:
25.
Wingfield C, Amis AA, Stead AC, et al. Comparison of
the biomechanical properties of Rottweiler and racing greyhound cranial cruciate ligaments. J Small
Anim Pract 2000;41:303–307.
Woo SL, Hollis JM, Adams DJ, et al. Tensile properties
of the human femur–anterior cruciate ligament–
tibia complex. The effects of specimen age and orientation. Am J Sports Med 1991;19:217–225.
Young K, Samiric T, Feller J, et al. Extracellular matrix
content of ruptured anterior cruciate ligament tissue. Knee 2011;18:242–246.
Yu WD, Liu SH, Hatch JD, et al. Effect of estrogen
on cellular metabolism of the human anterior cruciate ligament. Clin Orthop Relat Res 1999:229–
238.
Zazulak BT, Paterno M, Myer GD, et al. The effects of
the menstrual cycle on anterior knee laxity: a systematic review. Sports Med 2006;36:847–862.
VetBooks.ir
9
Morphological Risk Factors for
Cruciate Ligament Rupture
Eithne Comerford
Introduction
Biologists use the term ‘morphology’ to
describe the size, shape, and structure of an
organism or one of its parts. The morphology
and function of the cruciate ligaments has
been discussed in Chapter 1. This chapter will
describe the morphology of the bones involved
in stifle joint articulation in dogs, and highlight
comparative aspects of knee joint morphology
in non-contact anterior cruciate ligament (ACL)
injury in human beings.
Stifle joint morphology may play a causative
role in canine cruciate ligament degeneration
and rupture (CR). Conformational variation of
canine pelvic limbs such as a straight stifle
joint, narrow intercondylar notch, steep tibial plateau slope and increased distal femoral
torsion, may contribute to cruciate ligament
microinjury, which in turn has been hypothesized to cause progressive ligament rupture and
arthritis (Aiken et al. 1995; Comerford et al. 2006;
Duerr et al. 2007; Mostafa et al. 2014).
Distal femur
The distal femoral intercondylar notch (ICN)
contains both the cranial cruciate ligament
(CrCL) and the caudal cruciate ligament, as
they twist around each other from their femoral
attachment to their tibial attachment sites.
The distal femoral ICN is narrowed in dogs
and human beings with CR/ACL rupture and
arthritis because of increased osteophyte formation (Aiken et al. 1995; Wada et al. 1996; Lewis
et al. 2008; Chen et al. 2016). Stenotic or narrowed ICNs have been implicated as a risk factor in a recent meta-analysis of human ACL
injuries (Zeng et al. 2013).
A stenotic ICN causes impingement by the
medial aspect of the lateral femoral condyle
or the intercondylar roof on the CrCL/ACL
(Aiken et al. 1995). If a normal-sized ACL passes
through a narrowed ICN, the reduced space
could impede the normal function of the ACL,
causing impingement and therefore damage
to the ACL (Muneta et al. 1997). One study
suggested that ACL impingement may occur
at the anterior and posterior roof of the notch
during tibia external rotation and abduction,
resulting in ligament microinjury (Dienst et al.
2007). This study also found a significant correlation between ACL cross-sectional area to
notch surface area, with a smaller notch being
associated with a smaller mid-substance crosssectional area of the ACL. Some patients with
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
73
VetBooks.ir
74
Etiopathogenesis of Cruciate Ligament Rupture
congenital stenosis who sustained an ACL tear
by non-contact means were found to be young,
with small ICN width index measurements
(Souryal et al. 1988). It is also thought that knee
laxity may contribute to ICN narrowing and
then result in further ACL impingement and
damage (Wada et al. 1996).
To date, notch width (NW) or notch width
index (NWI) have been the parameters used to
determine the width of the human and canine
ICN. The shape of the notch is also thought
to be a critical factor in the role of the ICN in
ACL injury. ICN shapes have been described
as bell- or inverted U-shaped, A-shaped, or Wshaped (wave/crest-shaped) (Anderson et al.
2001; Chen et al. 2016). In dogs, the ICN is
bell-shaped (Fitch et al. 1995). Normal ICNs
tend to be inverted U-shaped, whereas narrower notches tend to more A- or W-shaped
(Anderson et al. 2001). The notch shape may also
change during life (Hirtler et al. 2016). Recent
studies have suggested that A-shaped notches
can predispose to ACL injury (Al-Saeed et al.
2013). It has also been suggested that determination of the notch shape index (NSI) (Tillman
et al. 2002; Geng et al. 2016) may be a more useful measurement, as it is a relative measure of
the notch width in a medial/lateral direction
to the notch height in the anterior/posterior
direction. A low NSI will cause the ACL to be
pushed into a smaller anterior outlet of the ICN,
with the joint in extension (Figure 9.1) (Tillman et al. 2002). In a multivariate model of
knee joint geometry, gender-related differences
were found with regard to intercondylar notch
size and shape, with women having a narrower
notch and men having a smaller ACL volume
being predisposed to ACL injury (Sturnick et al.
2015).
Differences in the ICN and its width have
been investigated in normal and CrCL-deficient
stifle joints, as well as ‘at-risk’ stifle joints from
dog breeds with differing predispositions to
CR (Comerford et al. 2006; Lewis et al. 2008;
Mostafa et al. 2009; Ragetly et al. 2011). An
ex vivo study found that dogs at high-risk
for CR (Labrador and Golden Retrievers) had
smaller ICNs than dogs at a low-risk (Greyhounds) (Comerford et al. 2006). This study
hypothesized that smaller ICNs may cause ligament impingement with associated cartilaginous changes within the extracellular matrix
F
A
B
E
C
D
Figure 9.1 Measurements of the canine intercondylar
notch (ICN) (adapted from Fitch et al. 1995). A, cranial
notch width; B, central notch width; C, caudal notch
width; D, condylar notch width; E, ICN height; F, femoral
condyle height. The cranial notch width index (NWI) is
A/D, the central NWI is B/D, and the caudal NWI is C/D,
the notch shape index (NSI) is B/E and ICN height index
is E/F). Source: Comerford et al. 2006. Reproduced with
permission from Elsevier.
(ECM), leading to CrCL inflammation and
degeneration.
Cranial NWIs were significantly greater
in the low-risk breeds (e.g., Greyhounds),
compared to high-risk breeds (Retrievers)
(Comerford et al. 2006). However, there was no
significant difference in the NSI between highand low-risk dog breeds (Figure 9.2). As part
of this study, the stifle joints of the three dog
breeds were placed in full extension and the
areas of the CrCLs impinged by the ICN were
marked and removed. Analyses of biochemical parameters such as collagen content and
crosslinks, matrix metalloproteinases (MMPs),
tissue inhibitors of metalloproteinases (TIMPs)
and sulfated and total glycosaminosglycans
(GAGs) were then performed as previously
described (Comerford et al. 2004). The expression of pro and active MMP2 was significantly
increased in CrCLs of the high-risk breeds,
compared to the low-risk breed, suggesting
increased collagen remodeling (Figure 9.3).
There were significantly more sulfated GAGs
in the impinged areas of the high-risk CrCLs,
compared to those of the low-risk breeds
p < 0.001
0.05
(A)
0.2
Greyhound G. Retriever
Labrador
Central
**
p < 0.02
50
**
25
0
(A)
0.0
(B)
0.3
Greyhound
G. Retriever
Caudal
Labrador
p < 0.05
ActiveMMP-2
20
0.0
Greyhound
G. Retriever
Labrador
Figure 9.2 Intercondylar notch (ICN) width indices (ICN
width indices (cranial (A), central (B) and caudal (C) in
Greyhound (n = 60), Golden Retriever (n = 23), and
Labrador Retriever (n = 26) femurs). ∗∗ Denotes stated
statistical significance to the other two groups. Source:
Comerford et al. 2006. Reproduced with permission from
Elsevier.
(Figure 9.4). Interestingly, the bodyweight of
the Labrador Retrievers was correlated with a
decrease in the central NWI (P = 0.004, r = 0.50),
whilst age did not correlate with any of the ICN
parameters. It is possible that an increased load
on the Labrador Retriever stifle joints alters the
joint mechanics, and that this may contribute
to ICN remodeling and narrowing. NSI was
not a factor in the predisposed dogs. Taken
together, these data suggest that impingement
by the ICN on the CrCLs of the high-risk breeds
may result in reduced structural integrity of
the ligament, predisposing the ligament to
**
10
0
Greyhound
G. Retriever
L. Retriever
Figure 9.3 The levels of proMMP-2 (A) and active
MMP-2 (B) (% of standard) in the impinged parts of
Greyhound (n = 10), Golden Retriever (n = 8), and
Labrador Retriever (n = 10) cranial cruciate ligaments.
∗∗ Denotes stated statistical significance to the other two
groups. SEM, standard error of the mean. Source:
Comerford et al. 2006. Reproduced with permission from
Elsevier.
p < 0.001
1.5
% Sulphated GAG of total
wet weight (mg) +/– SEM
0.1
p < 0.001
30
(B)
0.2
G. Retriever L. Retriever
40
**
(C)
Greyhound
50
0.1
75
p < 0.003
ProMMP-2
75
% MMP-2 std + SEM
0.10
0.00
ICN width index
(mm/mm)
Cranial
**
% MMP2 std + SEM
ICN width index
(mm/mm)
0.15
ICN width index
(mm/mm)
VetBooks.ir
Morphological Risk Factors for Cruciate Ligament Rupture
1.0
**
0.5
0.0
Greyhound
G. Retriever
L. Retriever
Figure 9.4 Levels of sulfated GAG (% total weight) in
the impinged parts of Greyhound (n = 10), Golden
Retriever (n = 8) and Labrador Retriever (n = 10) cranial
cruciate ligaments. ∗∗ Denotes stated statistical
significance to the other two groups. Source: Comerford
et al. 2006. Reproduced with permission from Elsevier.
VetBooks.ir
76
Etiopathogenesis of Cruciate Ligament Rupture
increased laxity and eventual joint degeneration. However, a recent study which examined
the morphometric characteristics of the pelvic
limbs of Labrador Retrievers with and without
CR (Mostafa et al. 2009) found ICN stenosis not
to contribute to the risk of CR, though ligament
changes were not examined in this study.
The contribution of other aspects of femoral
conformation such as femoral varus and anteversion angles have been described (Ragetly et al.
2011). The latter authors found that an increased
femoral anteversion angle (FAA) (Figure 9.5)
and body fat composition was greater in predisposed pelvic limbs from Labrador Retrievers. In
a recent study the measurement of FAA, using
Figure 9.5 The femoral anteversion angle (FAA) equals
the value of the tangent of ‘a’ divided by ‘b’. The long
axis of the femoral shaft is drawn on the lateral (A) and
craniocaudal (B) femoral views between two points
centered in the proximal femoral shaft. These two points
were identified by bisecting the two femoral cortices,
respectively, at one-fourth (25% line) and one-half (50%
line) of the total femoral length. (A) The distance ‘a’ from
the center of the femoral head to the extended axis of the
femoral shaft was measured on the lateral view of the
femur. (B) The distance ‘b’ from the center of the femoral
head to the extended axis of the femoral shaft was
measured on the craniocaudal view of the femur. Source:
Ragetly et al. 2011. Reproduced with permission from
John Wiley & Sons, Inc.
computed tomography (CT), has been found
to be more accurate than using a single lateral
radiograph (Mostafa et al. 2014).
Tibia
The stifle joint is subjected to external ground
reaction forces at weight-bearing and internal forces generated by muscular contraction.
These forces not only compress the femoral and
tibial articular surfaces, but also generate a cranially directed shear force in the tibia known as
cranial tibial thrust (CTT). CTT is present in the
stifle as the tibial plateau is not perpendicular to
a line drawn between the center of motion of the
stifle and hock joints, but is directed caudodistally (Slocum & Devine 1983). Numerous studies have been conducted to evaluate the association of the tibial plateau angle (TPA) and CR
(Read & Robins 1982; Macias et al. 2002; Duerr
et al. 2007). Although anatomic differences in
the shape of the proximal tibia have been documented in dogs with CR, its role in the rupture mechanism is unclear (Wilke et al. 2002;
Guastella et al. 2008). The mean TPA in dogs
varies between 23◦ and 25◦ , while a wide range
of TPA has been reported (13–34◦ ) in normal
dogs and can vary according to breed (Aertsens et al. 2015). A study conducted by Wilke
and others revealed that the functional TPA is
approximately parallel to the ground in most
dogs (Wilke et al. 2002). Although pathological increases in TPA (>55◦ ) have been correlated with CR (Read & Robins 1982; Macias et al.
2002), whether a general association between
TPA and CR exists in dogs remains controversial. A recent study found that an excessive
TPA may contribute to CR, as demonstrated in
experimental Beagles where TPAs >40◦ resulted
in chondroid changes in the ligament ECM
which could lead eventually to non-contact ligament degeneration (Ichinohe et al. 2015).
Studies have shown that the TPAs are not
significantly different in Labrador Retrievers
with and without CR, and also in a comparison
between Greyhounds and Labrador Retrievers
(Wilke et al. 2002; Reif & Probst 2003). Interestingly, German Shepherd dogs have an increased
TPA when compared to dogs of high-risk breeds
such as the Rottweiler (Guastella et al. 2008),
but have a low risk of CR. The true effect
VetBooks.ir
Morphological Risk Factors for Cruciate Ligament Rupture
of TPA on CrCL stresses in vivo is currently
unknown, as muscular force, body size, obesity,
rapid weight gain, relative inactivity, and exercise can all modify the amount of stress sustained by the CrCL, in addition to the TPA (Colborne et al. 2005). The TPA was more likely to be
predictive of CR in predisposed pelvic limbs, in
combination with morphometric characteristics
such as the FAA (as described above) and body
fat composition (Ragetly et al. 2011). Muscular
imbalance may also be a risk factor in the development of CR in at-risk breeds, where atrophy
of the quadriceps muscle may lead to an overdominance of the gastrocnemius increasing cranial tibial thrust in predisposed pelvic limbs
(Mostafa et al. 2010).
Development of the tibial tuberosity and
the shape (convexity) of tibial condyles may
also be relevant in the pathogenesis of CR
(Guerrero et al. 2007). Smaller tibial tuberosity
widths are thought to increase CTT and promote CrCL degeneration, thus leading to rupture in a younger population of dogs (Inauen
et al. 2009). In a multivariate analysis performed
by Mostafa and others in Labrador Retrievers,
cranial angulation of the proximal portion of the
tibia, excessive steepness of the tibial plateau,
and distal femoral torsion appeared more likely
to be associated with CR than femoral angulation, tibial torsion, intercondylar notch stenosis
and increased inclination of the patellar tendon
(Mostafa et al. 2009).
In human beings, controversy also exists over
whether posterior tibial slope is an anatomic
risk factor for ACL injuries. Meister and others
failed to demonstrate any relationship between
non-contact ACL injuries and the posterior tibia
slope (Meister et al. 1998). However, in more
recent studies, tibial slope has been found to be
a risk factor for ACL rupture (Sonnery-Cottet
et al. 2011; Sturnick et al. 2015).
Patella/quadriceps mechanism
and Q-angle
Conformational abnormalities of the distal
femur, such as genu varum and malalignment of the quadriceps mechanism associated
with medial patellar luxation (MPL), can cause
increased internal stress on the CrCL (Duval
et al. 1999). In human beings, the quadriceps
77
(Q-angle) may contribute to an increased risk of
ACL injury (Shambaugh et al. 1991), although its
role in non-contact ACL injuries is unclear. The
Q-angle is the angle formed by a line directed
from the insertion of the m. rectus femoris on
the ilium to the middle to the trochlear groove
and a second line from the tibial tuberosity to
the trochlear groove mirroring the course of the
patella tendon. In normal dogs, the Q-angle is
reported to be 10.5◦ medially and can increase
with different grades of MPL (Mortari et al.
2009), increasing up to 36.6◦ for a grade III MPL.
The average Q-angle in dogs with isolated CR
was reported to be 19.3◦ in this study, because
of loss of CrCL restraint on internal rotation of
the tibia (Kaiser et al. 2001). Ragetly and others
did not find any effect of Q-angle in their multivariate approach to predict CR risk in predisposed Labrador Retriever pelvic limbs (Ragetly
et al. 2011).
The angles between the patellar tendon
and the tibial plateau have also been measured in humans (Nisell 1985) and in healthy
dogs (Dennler et al. 2006) as a function of
stifle joint flexion. Dogs with partially torn
CrCLs, anatomically, have marginally larger
angles between the patellar tendon and tibial
plateau compared with joints with intact CrCLs
(Schwandt et al. 2006).
Fabella
A recent study found that 70% of West Highland White Terriers had a mediodistal position of their medial fabella, compared to other
small- and large-breed dogs. This finding was
not associated with MPL or CR, and is considered to be a normal anatomic finding for this
breed (Stork et al. 2009).
Conclusion
Stifle joint morphology, in particular the distal
femoral ICN, femoral anteversion, the TPA and
muscular imbalance, may play a contributing
role in CrCL degeneration and CR in the dog.
The ICN has been shown to be smaller in dog
breeds with an increased predisposition to CR,
resulting in an altered ECM turnover. Morphometric characteristics of the anatomy of the stifle
VetBooks.ir
78
Etiopathogenesis of Cruciate Ligament Rupture
joint associated with increased risk of CR have
recently been well described in the Labrador
Retriever. However, the role of these factors in
vivo, along with neuromuscular forces, has yet
to be elucidated.
References
Aertsens A, Rincon Alvarez J, Poncet CM, et al. Comparison of the tibia plateau angle between small
and large dogs with cranial cruciate ligament disease. Vet Comp Orthop Traumatol 2015;28:385–390.
Aiken S, Kass PH, Toombs JP. Intercondylar notch
width in dogs with and without cranial cruciate ligament injuries. Vet Comp Orthop Traumatol 1995;
8:128–132.
Al-Saeed O, Brown M, Athyal R, et al. Association of femoral intercondylar notch morphology,
width index and the risk of anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc
2013;21:678–682.
Anderson AF, Dome DC, Gautam S, et al. Correlation
of anthropometric measurements, strength, anterior cruciate ligament size, and intercondylar notch
characteristics to sex differences in anterior cruciate
ligament tear rates. Am J Sports Med 2001;29:58–66.
Chen C, Ma Y, Geng B, et al. Intercondylar notch
stenosis of knee osteoarthritis and relationship
between stenosis and osteoarthritis complicated
with anterior cruciate ligament injury: A study in
MRI. Medicine (Baltimore) 2016;95:e3439.
Colborne GR, Innes JF, Comerford EJ, et al. Distribution of power across the hind limb joints in
Labrador Retrievers and Greyhounds. Am J Vet Res
2005;66:1563–1571.
Comerford EJ, Innes JF, Tarlton JF, et al. Investigation
of the composition, turnover, and thermal properties of ruptured cranial cruciate ligaments of dogs.
Am J Vet Res 2004;65:1136–1141.
Comerford EJ, Tarlton JF, Avery NC, et al. Distal
femoral intercondylar notch dimensions and their
relationship to composition and metabolism of the
canine anterior cruciate ligament. Osteoarthritis
Cartilage 2006;14:273–278.
Dennler R, Kipfer NM, Tepic S, et al. Inclination of the
patellar ligament in relation to flexion angle in stifle
joints of dogs without degenerative joint disease.
Am J Vet Res 2006;67:1849–1854.
Dienst M, Schneider G, Altmeyer K, et al. Correlation of intercondylar notch cross sections to the
ACL size: a high resolution MR tomographic in vivo
analysis. Arch Orthop Trauma Surg 2007;127:253–
260.
Duerr FM, Duncan CG, Savicky RS, et al. Risk factors for excessive tibial plateau angle in large-breed
dogs with cranial cruciate ligament disease. J Am
Vet Med Assoc 2007;231:1688–1691.
Duval JM, Budsberg SC, Flo GL, et al. Breed, sex, and
body weight as risk factors for rupture of the cranial cruciate ligament in young dogs. J Am Vet Med
Assoc 1999;215:811–814.
Fitch RB, Montgomery RD, Milton JL, et al. The
intercondylar fossa of the normal canine stifle an
anatomic and radiographic study. Vet Surg 1995;
24:148–155.
Geng B, Wang J, Ma JL, et al. Narrow intercondylar notch and anterior cruciate ligament injury in
female nonathletes with knee osteoarthritis aged
41–65 years in plateau region. Chin Med J (Engl)
2016;129:2540–2545.
Guastella DB, Fox DB, Cook JL. Tibial plateau angle
in four common canine breeds with cranial cruciate ligament rupture, and its relationship to meniscal tears. Vet Comp Orthop Traumatol 2008;21:125–
128.
Guerrero TG, Geyer H, Hassig M, et al. Effect of conformation of the distal portion of the femur and
proximal portion of the tibia on the pathogenesis
of cranial cruciate ligament disease in dogs. Am J
Vet Res 2007;68:1332–1337.
Hirtler L, Rohrich S, Kainberger F. The femoral intercondylar notch during life: An anatomic redefinition with patterns predisposing to cruciate
ligament impingement. Am J Roentgenol 2016:
1–10.
Ichinohe T, Kanno N, Harada Y, et al. Histological
and immunohistological analysis of degenerative
changes in the cranial cruciate ligament in a canine
model of excessive tibial plateau angle. Vet Comp
Orthop Traumatol 2015;28:240–249.
Inauen R, Koch D, Bass M, et al. Tibial tuberosity conformation as a risk factor for cranial cruciate ligament rupture in the dog. Vet Comp Orthop Traumatol 2009;22:16–20.
Kaiser S, Cornely D, Golder W, et al. The correlation of
canine patellar luxation and the anteversion angle
as measured using magnetic resonance images. Vet
Radiol Ultrasound 2001;42:113–118.
Lewis BA, Allen DA, Henrikson TD, et al. Computed
tomographic evaluation of the canine intercondylar notch in normal and cruciate deficient stifles. Vet
Comp Orthop Traumatol 2008;21:119–124.
Macias C, McKee WM, May C. Caudal proximal tibial
deformity and cranial cruciate ligament rupture in
small-breed dogs. J Small Anim Pract 2002;43:433–
438.
Meister K, Talley MC, Horodyski MB, et al. Caudal
slope of the tibia and its relationship to noncontact
injuries to the ACL. Am J Knee Surg 1998;11:217–
219.
Mortari AC, Rahal SC, Vulcano LC, et al. Use of
radiographic measurements in the evaluation of
dogs with medial patellar luxation. Can Vet J 2009;
50:1064–1068.
Mostafa AA, Griffon DJ, Thomas MW, et al. Morphometric characteristics of the pelvic limbs of
VetBooks.ir
Morphological Risk Factors for Cruciate Ligament Rupture
Labrador Retrievers with and without cranial cruciate ligament deficiency. Am J Vet Res 2009;70:
498–507.
Mostafa AA, Griffon DJ, Thomas MW, et al. Morphometric characteristics of the pelvic limb musculature of Labrador Retrievers with and without cranial cruciate ligament deficiency. Vet Surg
2010;39:380–389.
Mostafa AA, Griffon DJ, Thomas MW, et al. Radiographic evaluation of femoral torsion and correlation with computed tomographic techniques
in Labrador Retrievers with and without cranial
cruciate ligament disease. Vet Surg 2014;43:534–
541.
Muneta T, Takakuda K, Yamamoto H. Intercondylar
notch width and its relation to the configuration
and cross-sectional area of the anterior cruciate ligament. A cadaveric knee study. Am J Sports Med
1997;25:69–72.
Nisell R. Mechanics of the knee. A study of joint and
muscle load with clinical applications. Acta Orthop
Scand Suppl 1985;216:1–42.
Ragetly CA, Evans R, Mostafa AA, et al. Multivariate analysis of morphometric characteristics
to evaluate risk factors for cranial cruciate ligament deficiency in Labrador Retrievers. Vet Surg
2011;40:327–333.
Read RA, Robins GM. Deformity of the proximal tibia
in dogs. Vet Rec 1982;111:295–298.
Reif U, Probst CW. Comparison of tibial plateau
angles in normal and cranial cruciate deficient stifles of Labrador Retrievers. Vet Surg 2003;32:385–
389.
Schwandt CS, Bohorquez-Vanelli A, Tepic S, et al.
Angle between the patellar ligament and tibial
plateau in dogs with partial rupture of the cranial cruciate ligament. Am J Vet Res 2006;67:1855–
1860.
79
Shambaugh JP, Klein A, Herbert JH. Structural measures as predictors of injury basketball players.
Med Sci Sports Exerc 1991;23:522–527.
Slocum B, Devine T. Cranial tibial thrust: a primary
force in the canine stifle. J Am Vet Med Assoc
1983;183:456–459.
Sonnery-Cottet B, Archbold P, Cucurulo T, et al. The
influence of the tibial slope and the size of the intercondylar notch on rupture of the anterior cruciate
ligament. J Bone Joint Surg Br 2011;93:1475–1478.
Souryal TO, Moore HA, Evans JP. Bilaterality in
anterior cruciate ligament injuries: associated
intercondylar notch stenosis. Am J Sports Med
1988;16:449–454.
Stork CK, Petite AF, Norrie RA, et al. Variation in
position of the medial fabella in West Highland
white terriers and other dogs. J Small Anim Pract
2009;50:236–240.
Sturnick DR, Vacek PM, DeSarno MJ, et al. Combined
anatomic factors predicting risk of anterior cruciate
ligament injury for males and females. Am J Sports
Med 2015;43:839–847.
Tillman MD, Smith KR, Bauer JA, et al. Differences
in three intercondylar notch geometry indices
between males and females: a cadaver study. Knee
2002;9:41–46.
Wada M, Imura S, Baba H, et al. Knee laxity in patients
with osteoarthritis and rheumatoid arthritis. Br J
Rheumatol 1996;35:560–563.
Wilke VL, Conzemius MG, Besancon MF, et al. Comparison of tibial plateau angle between clinically
normal Greyhounds and Labrador Retrievers with
and without rupture of the cranial cruciate ligament. J Am Vet Med Assoc 2002;221:1426–1429.
Zeng C, Gao SG, Wei J, et al. The influence of the intercondylar notch dimensions on injury of the anterior cruciate ligament: a meta-analysis. Knee Surg
Sports Traumatol Arthrosc 2013;21:804–815.
VetBooks.ir
VetBooks.ir
10
Role of Nitric Oxide
Production and Matrix
Protease Activity in Cruciate
Ligament Degeneration
David E. Spreng and Simone Forterre
Nitric oxide: An overview
Nitric oxide (NO) is an important mediator in
physiologic and pathophysiologic pathways in
the body. As a nonpolar, highly reactive gas,
NO diffuses freely through cell membranes and
reacts with transition metals, binds to reactive cysteine thiol, or forms reactive oxygen
molecules. Initially, it has been identified as
the small-molecular-weight mediator released
from endothelial cells that promotes the relaxation of adjacent vascular smooth muscle.
This explains its earlier acronym ‘endotheliumderived relaxing factor.’ The generation of NO
occurs when nitric oxide synthase (NOS) catalyzes the conversion of L-arginine to NO and
L-citrulline in a two-step process (Figure 10.1;
Marletta 1993). Under aerobic conditions, NO
is not stable and is promptly oxidized to higher
nitrogen oxides called reactive nitrogen or nitrogen oxide intermediates such as peroxynitrite
(ONOO– ).
Three isoforms of NOS with characteristic
tissue distribution have been described: the
constitutive endothelial (eNOS) and neuronal
(nNOS) isoforms, and the inducible isoform
(iNOS). The activities of isoforms differ in that
the constitutive isoforms are Ca2+ -dependent
and produce relatively low levels of NO.
Physiological low amounts of NO released by
eNOS in vascular endothelial cells regulate
blood vessel tone, platelet aggregation, or
cell diapedesis. In the neuronal system, NO
derived from nNOS has been identified as a
neurotransmitter of certain non-adrenergic,
non-cholinergic nerve fibers in various organs
such as cerebral arteries, myocardium, and
pancreas in the dog. In contrast, the iNOS
forms a tight complex with calmodulin independent from intracellular calcium levels, and
once activated produces large amounts of NO
over extended periods of time (Weinberg et al.
2007). Pro-inflammatory cytokines known to
induce iNOS include interleukin-1 beta (IL-1β),
tumor necrosis factor alpha (TNFα) and interferon gamma (IFNγ), whereas transforming
growth factor beta (TGFβ), IL-4, IL-10 or even
glucocorticoids can inhibit the expression of
iNOS (Kroncke et al. 1995).
iNOS is expressed in nearly all eukaryotic
cells, including monocytes/macrophages,
hepatocytes, synovial cells, and chondrocytes
(Kroncke et al. 1995). Depending on the amount
of NO released and the NOS involved, effects of
NO vary at sites of inflammation. NO in higher
concentrations regulates the T-cell balance by
Th1 downregulation and Th2 upregulation,
inhibits viral replication in macrophages,
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
81
VetBooks.ir
82
Etiopathogenesis of Cruciate Ligament Rupture
L-arginine
O2, NADPH
iNOS, cNOS
H2O, NADP+
N-hydroxy-L-arginine
O2, 1/2 equiv NADPH
iNOS, cNOS
H2O, 1/2 equiv NADP+
L-citrulline + NO
Figure 10.1 Production of nitric oxide via the oxidation
of L-arginine by a family of nitric oxide synthase (NOS)
enzymes.
suppresses different cellular protein synthesis
in various cell types, and produces marked
cytotoxicity by inhibiting mitochondrial respiration or inducing DNA alterations. Reaction
of NO with the superoxide anion (O2 .– ),
another product of activated macrophages,
may yield peroxynitrite (ONOO– ) which mediates oxidative DNA damage and subsequently
programmed cell death described for several
cell types, including chondrocytes (Del Carlo &
Loeser 2002).
The list of diseases where iNOS is currently
thought to be involved is large and rapidly
increasing. In multiple organ failure following
septic shock, type I diabetes or ulcerative colitis, massive NO formation due to iNOS activation was characterized. Another chronic local
inflammatory process with iNOS participation
occurs in the arthritic joint (Del Carlo & Loeser
2008).
Nitric oxide activity in articular tissues
Apart from iNOS, the isoforms cNOS and
nNOS which produce lower amounts of NO,
have also been detected in different healthy and
osteoarthritic joint tissues (Amin et al. 1995; Pelletier et al. 2000; Di Mauro et al. 2006). However,
nNOS was more frequently expressed in normal than in osteoarthritis (OA) chondrocytes
(Rosa et al. 2008). Within joints, NO is mainly
produced by superficial cartilage chondrocytes
and by synoviocytes or macrophages in the
inflamed synovial membrane; all cells in which
iNOS expression is upregulated during OA
(Amin et al. 1995; Häuselmann et al. 1998).
The importance of iNOS expression and the
subsequent increase of NO in the pathogenesis
of OA is endorsed by experiments in vivo
demonstrating that specific inhibition of iNOS
results in decreased production of cytokines,
matrix metalloproteinases (MMPs) and peroxynitrite (Pelletier et al. 1999). Furthermore,
ex vivo studies demonstrated that the canine
cranial cruciate ligament (CrCL) actively produces NO mainly derived from the inducible
NOS pathway (Spreng et al. 2000), suggesting
that ligament fibroblasts are actively involved
in extracellular matrix (ECM) homeostasis.
Additionally, the activation of CrCL with a proinflammatory mixture of lipopolysaccharide
(LPS)/IL-1/TNF leads to increased NO production and iNOS activity, indicating that ligament
fibroblasts indeed produce substantial amounts
of NO under a specific stimulus (Louis et al.
2006).
Upon
exposure
to
pro-inflammatory
cytokines, including IL-1β, IL-17, TNFα,
IFNγ, and LPS, as well as to shear stress, iNOS
expression is upregulated, resulting in an
increased NO production that perpetuates the
release of inflammatory cytokines and other
catabolic processes.
As assessment of the unstable NO is
extremely difficult, NO production must
be calculated by measuring its stable end
products nitrite or nitrate. In ligament tissue,
especially in partially or totally ruptured CrCL,
the assessment of NO production is difficult.
Specimens of naturally diseased CrCL are
usually retrieved from canine patients during
surgical repair, leading to the problem that
highly traumatized tissue is examined without
knowing if a measured production of NO and
NO metabolites is triggered by the original
CrCL pathology, or is only a consequence of
the mechanical trauma of ligament disruption.
Interestingly, normal CrCL produces more NO
compared to torn CrCL, normal cartilage or
normal medial collateral ligaments of the stifle
in dogs (Spreng et al. 2000)
83
VetBooks.ir
Role of Nitric Oxide Production and Matrix Protease Activity in Cruciate Ligament Degeneration
Figure 10.2
The catabolic actions of NO and matrix metalloproteinases (MMPs) on CrCL matrix homeostasis.
Role of NO and reactive oxygen
species in the joint
NO is believed to be mainly a catabolic player in
joint physiology (see Figure 10.2). NO is a predominant mediator in the progression of OA by
inhibiting proteoglycan and collagen synthesis,
and promoting activation of metalloproteinases
or chondrocyte apoptosis which could further
contribute to ECM reduction in OA (Taskiran
et al. 1994; Goggs et al. 2003; Nakagawa et al.
2010). In pathological situations such as OA,
additional reactive molecules, so-called reactive
oxygen species (ROS), are abnormally produced
and contribute directly or indirectly to cartilage
degradation, MMP activation and cell death
induction (Lepetsos & Papavassiliou 2016). ROS
are free radicals containing oxygen molecules
including hydroxyl radical, hydrogen peroxide, superoxide anion and nitric oxide, and
are generated mainly by the mitochondria.
Peroxynitrite, a redox derivative of NO, has
been implicated in pro-inflammatory and proapoptotic effects by triggering the oxidative
damage of cellular proteins, oxidizing lipids,
and DNA in human articular cartilage (Pacher
et al. 2007). Chondrocyte death is regarded as a
major factor in OA pathogenesis. NO has been
reported to be the primary inducer of chondrocyte apoptosis mediated by a caspase- and
mitochondria-dependent pathway (Maneiro
et al. 2005), while other studies have shown
that endogenous NO alone does not induce
cell death; rather, the generation of additional
ROS is also required (Del Carlo & Loeser 2002;
Liang et al. 2014). Studies of human chondrocytes showed that peroxynitrite induced
apoptosis via a caspase-independent pathway
(Whiteman et al. 2004). NO-induced apoptosis
of chondrocytes depends on crosstalk between
the iNOS and cyclooxygenase 2 (COX-2)
systems, which is linked to the activation of
mitogen-activated protein kinase kinase 1 and
2 (MAP2K1/2) and p38 mitogen-activated
protein kinase pathways. Apoptosis has also
been detected in healthy and ruptured canine
CrCLs, with a moderate but significant correlation to NO (Gyger et al. 2007). Analyzing the
VetBooks.ir
84
Etiopathogenesis of Cruciate Ligament Rupture
distribution of apoptotic cells in different
segments of partially torn CrCLs suggests that
apoptosis in ligament fibroblasts is present
before mechanical disruption of the ligament
(Krayer et al. 2008).
Recent evidence has shown that ROS
may have an opposing activity in cytokinestimulated chondrocytes, suggesting that the
role of NO in OA may be more complex than
originally believed. Chondrocytes respond to
NO or ROS differently depending on the intensity, duration of the signaling, and the cellular
redox status. For example, in a zymosaninduced arthritis model, NO and peroxynitrite
induced inflammation and proteoglycan loss.
While the addition of a selective iNOS inhibitor
ameliorated only synovial inflammation, uric
acid (a peroxynitrite scavenger) was able to
decrease inflammation and proteoglycan loss,
suggesting that targeting peroxynitrite might
be more effective for protection against OA
(Bezerra et al. 2004).
It has also been shown that NO mediates the
expression of pro-inflammatory cytokines such
as IL-18 and IL-1 converting enzyme (Boileau
et al. 2002). Pro-inflammatory mediators such as
NO, IL-1, TNF, and prostaglandins are all overproduced in chondrocytes from patients with
OA (Weinberg et al. 2007).
MMP: An overview
The matrix metalloproteinases (MMPs) are a
group of structurally and functionally related
enzymes responsible for the proteolytic degradation of ECM and basal membrane components. Broad functions in defense, injury,
inflammation and normal tissue remodeling
have been attributed to MMPs (Manicone &
McGuire 2008). The role of MMPs in matrix
degradation and remodeling is considered to
be most important in the context of cruciate
ligament rupture (CR) and stifle arthritis. Due
to their potential detrimental effects, MMPs
are highly regulated at different levels. At the
level of transcription, MMP expression is controlled by multiple cytokines and growth factors. Moreover, MMPs are secreted as inactive
proMMPs (also called latent MMP or zymogen),
which then require activation that is initiated
by plasmin or membrane-type MMP. A third
level of regulation includes the local production of specific tissue inhibitors of metalloproteinases (TIMPs) (Ries & Petrides 1995; Nagase
et al. 2006). TIMP concentrations generally far
exceed the concentrations of MMPs in tissue,
thereby limiting their proteolytic activity in the
pericellular environment.
MMPs in the articular environment are
produced by synovial cells, osteoblasts, chondrocytes and ligament fibroblasts, as well as by
monocyte/macrophages or neutrophils. MMPs
capable of degrading the macromolecules of the
ECM comprise three subclasses with respect
to their substrate specificity: collagenases,
gelatinases, and stromelysins. The collagenases
(MMP-1, -8, and 13) are responsible for the first
degradation step of collagen by cleaving the
interstitial collagens I, II, and III. Collagen II
is the main collagen type of hyaline cartilage,
while collagen I forms the principal tensileresistant fiber of ligaments. The denatured
collagen, or gelatin, is further degraded by the
gelatinases (MMP-2, and -9). Among these,
MMP-13 has been frequently reported to be
the most important player in OA cartilage due
to its ability to degrade collagens more effectively (Murphy & Nagase 2008). Stromelysins
(MMP-3, -10, and 11) have a broader specificity,
including collagen type III, IV, V, VII, IX, XI,
as well as proteoglycans, gelatin, laminin
and fibronectin, and can also activate other
MMPs. MMP-2 and MMP-9 also cleave gelatin,
fibronectin and elastin beside collagen type IV
and V (Manicone & McGuire 2008).
Although details in signaling and control
mechanisms involved in MMP regulation
remain to be elucidated, recent findings have
been useful in developing an understanding of
the complex regulation of MMP synthesis and
activity.
The role of MMPs in the stifle joint
MMPs play a key role in the progression of various joint diseases and influence joint inflammation and matrix degradation. Most actions
of MMPs in joints are catabolic in nature (Figure 10.2). They are associated with increased
ECM degeneration of cartilage or ligaments,
and serve as significant cofactors in inflammatory reactions (Foos et al. 2001; Muir et al.
VetBooks.ir
Role of Nitric Oxide Production and Matrix Protease Activity in Cruciate Ligament Degeneration
2005; Doom et al. 2008). However, some MMPs
have opposite roles in the development of specific diseases. For example, MMP-2 and MMP9 (Gelatinase A and B) have very similar substrate specificities for matrix proteins, but have
opposite non-matrix-related actions: MMP-2 is
important for the degradation of inflammatory
factors, whereas MMP-9 is an important product of macrophages and neutrophils. Experimentally, MMP-2 deficiency leads to exacerbated arthritis, whereas a deficiency of MMP-9
reduces arthritis (Itoh et al. 2002).
Various studies have detected MMPs in CrCL
tissue during aging, degeneration, or in torn
CrCLs. Results of a study on cellular and ECM
changes in the human anterior cruciate ligament (ACL) showed that constitutive MMP
expression (MMP-1, -3, and -13) declines with
aging, while a marked upregulation occurs in
degenerated ACL, mainly in chondrocyte-like
cells but not in fibroblast-like cells (Hasegawa
et al. 2013). It was suggested that decreased
MMP expression with aging may reflect a
reduced capacity to remodel and maintain the
tissue, whereas an increase in ACLs from OA
knees may be caused by phenotypic changes
and contribute to degeneration. These findings are supported by examination of MMP
gene expression in ruptured and intact CrCLs
from dogs separated into different age groups.
MMP-13 and both gelatinases were significantly
increased in ruptured CrCLs only, whereas
the collagen I degrading enzymes MMP-1 and
MMP-3 were present in torn and in intact aged
CrCLs (Muir et al. 2005). The similar pattern of
metalloprotease expression in torn and aging
human and canine cruciate ligaments suggests
that changes in collagenolytic enzymes influence the development of subtle joint laxity over
time, and subsequently induces the progression
of CR (Foos et al. 2001; Muir et al. 2005).
Degradative enzymes have the potential to
diffuse from the ligament into the synovial
fluid, particularly if there are defects in the synovial lining and exposure of ligament to the
joint environment. Thus, many studies have
evaluated MMP activity in synovial fluid of
dogs with CR. In the synovial fluid of dogs with
acute CR, MMP-2 and MMP-9 activities are significantly elevated compared to synovial fluid
of unaffected or contralateral joints (Rabillard
et al. 2012; Boland et al. 2014; Murakami et al.
85
2016). The activity of MMP-13, however, was
similar and MMP-3 was not detected in synovial fluid in either healthy or affected joints.
Moreover, activity levels were not influenced by
surgical stabilization and postoperative doxycycline treatment (Rabillard et al. 2012).
MMP measurement in synovial fluid is only
of limited value in understanding pathophysiologic pathways because it is not possible to
differentiate the origin of the MMP production
when measured in synovial fluid (Fujita et al.
2006; Salinardi et al. 2006). Beside CrCL tissue,
elevated MMPs originate from other joint
tissues, particularly inflamed synovium or
cartilage.
Influence of NO and MMPs on CrCL
structure
The pathogenesis of canine CR involves
the complex processes that change a normal,
healthy ligament into an altered, nonfunctional,
and potentially torn ligament. Alterations have
been evaluated in both the ligament fibroblasts and the ECM, and characterized from the
molecular to the macroscopic level, yet the exact
role still remains to be verified. One of the main
reasons for this is the difficulty in studying the
early phase of the disease process that leads
to CR.
There is good evidence that NO and MMPs
modulate the consequences of CR, for example OA (Abramson 2008). On the other hand,
almost all scientific information on NO and
MMP involvement in the early and subclinical
stages of the CR condition is only descriptive
and fragmented, and does not allow any definite conclusions to be made on the exact pathway that leads to CrCL fiber rupture. Some of
these data concerning direct actions of NO and
MMP on the ligament are described below.
External stimuli induce NO and MMP in
ligaments
Recent findings of a study using a novel canine
model revealed that synovial debridement
of the CrCL has detrimental effects on clinical signs such as pain, and also on effusion,
function, and histology (Bozynski et al. 2015).
VetBooks.ir
86
Etiopathogenesis of Cruciate Ligament Rupture
Synoviectomy of the rabbit CrCL induces a significant increase in collagenase activity within
the ligament, indicating that the synovial sheath
is a critically important structure for joint health
(Amiel et al. 1990). The released collagenase
after synoviectomy may reflect the reaction of
the CrCL to synovial fluid mediators released
from inflamed synovium. Canine CrCL explant
cultures, as well as ligament fibroblast monolayer cultures activated with an inflammatory
stimulus, produce significantly more NO and
MMP compared to non-stimulated cultures
over a period of 48 hours (Riitano et al. 2002).
The same stimulus induces a significantly
higher iNOS expression in CrCL compared to
medial collateral ligaments and femoral head
ligaments (Louis et al. 2006). Different patterns
of NO activity may reflect the different underlying abilities to react, and the different susceptibilities to pathological processes, between the
ligaments.
High NO levels inhibit collagen
synthesis in ligament fibroblasts
CrCL has been shown to produce more NO
compared to other ligaments (Cao et al. 2000;
Spreng et al. 2000). Experiments performed by
Cao and colleagues showed that NO production
was increased due to iNOS induction, particularly in CrCL cells, and inhibited normal collagen synthesis. High NO concentrations could,
therefore, be a reason for the insufficient healing capacities of ruptured CrCL in humans
and in dogs. Moreover, high NO concentrations in canine CrCL may contribute to matrix
homeostasis disturbance, leading to an intrinsic
weakness of the ligament.
NO combined with peroxynitrite induces
apoptosis in the ligament
In vitro experiments have demonstrated that
different NO donors induce apoptosis in CrCL
cells (Murakami et al. 2005; Forterre et al. 2011).
In addition, fibroblasts from the CrCL were
more susceptible to NO-induced apoptosis than
cells from the caudal cruciate ligament or from
the medial collateral ligament. CrCL apoptosis is influenced by inhibition of caspase3 (Murakami et al. 2005), and is attenuated
by treatment with ROS scavengers or a tyrosine kinase inhibitor (Forterre et al. 2012). On
the other hand, oral treatment with L-NIL, a
specific iNOS inhibitor, did not have a direct
influence on the amount of apoptotic ligament
fibroblasts in dogs with CR (Hofer et al. 2009).
Consequently, NO alone is not responsible for
increased levels of apoptosis in the CrCL. This
corresponds to other reports on chondrocytes
indicating that only the combination of NO and
ROS induces apoptosis (Del Carlo & Loeser
2002). Increased NO production could be an
early step in development of CR, and may contribute to the induction of cell death followed
by catabolic derangement of the homeostasis of
the ligament.
Conclusions
All of the above described observations correspond with the theory that an initial event leads
to inflammation of the cruciate ligament complex (Hayashi et al. 2004). Ligament fibroblasts
develop a dysregulation of matrix homeostasis as a reaction to the inflammatory stimulus,
including an upregulation of matrix-degrading
enzymes, a downregulation of matrix production, and peroxynitrite-induced premature ligament fibroblast death (see Figure 10.2). The
role of NO, however, is less simple. By extrapolating data from in vitro cartilage experiments
it seems that inhibition of NOS generation is
able to decrease inflammation, but alone has
little effect on protecting the joint from cartilage loss. On the other hand, peroxynitrite
inhibition reduces intra-articular inflammation
and loss of articular cartilage (Bezerra et al.
2004). Other studies, however, have shown the
opposite: OA dogs treated with a specific iNOS
inhibitor showed a reduction in osteophyte formation, a decrease in the severity of histological
cartilage lesions, and a reduced levels of apoptosis in cartilage compared to untreated dogs
(Pelletier et al. 2000). Adding to the complexity of the known catabolic effects of NO, the
latter has also been shown to promote cartilage deposition, thereby highlighting a protective role of NO in tenocytes and human chronic
OA (Xia et al. 2006; Hancock & Riegger-Krugh
2008). These conflicting results suggest that the
role of NO in OA needs to be further elucidated.
VetBooks.ir
Role of Nitric Oxide Production and Matrix Protease Activity in Cruciate Ligament Degeneration
References
Abramson SB. Nitric oxide in inflammation and pain
associated with osteoarthritis. Arthritis Res Ther
2008;10:S2.
Amiel D, Billings E, Jr, Harwood FL. Collagenase activity in anterior cruciate ligament: protective role of the synovial sheath. J Appl Physiol
1990;69:902–906.
Amin AR, Di Cesare PE, Vyas P, et al. The expression
and regulation of nitric oxide synthase in human
osteoarthritis-affected chondrocytes: evidence for
up-regulated neuronal nitric oxide synthase. J Exp
Med 1995;182:2097–2102.
Bezerra MM, Brain SD, Greenacre S, et al. Reactive nitrogen species scavenging, rather than nitric
oxide inhibition, protects from articular cartilage
damage in rat zymosan-induced arthritis. Br J Pharmacol 2004;141:172–182.
Boileau C, Martel-Pelletier J, Moldovan F, et al. The
in situ up-regulation of chondrocyte interleukin1-converting enzyme and interleukin-18 levels
in experimental osteoarthritis is mediated by
nitric oxide. Arthritis Rheum 2002;46:2637–
2647.
Boland L, Danger R, Cabon Q, et al. MMP-2 as an
early synovial biomarker for cranial cruciate ligament disease in dogs. Vet Comp Orthop Traumatol
2014;27:210–215.
Bozynski CC, Kuroki K, Stannard JP, et al. Evaluation of partial transection versus synovial debridement of the ACL as novel canine models for management of ACL injuries. J Knee Surg 2015;28:404–
410.
Cao M, Stefanovic-Racic M, Georgescu HI, et al. Does
nitric oxide help explain the differential healing
capacity of the anterior cruciate, posterior cruciate,
and medial collateral ligaments? Am J Sports Med
2000;28:176–182.
Del Carlo M, Jr, Loeser RF. Nitric oxide-mediated
chondrocyte cell death requires the generation
of additional reactive oxygen species. Arthritis
Rheum 2002;46:394–403.
Del Carlo M, Jr, Loeser RF. Cell death in osteoarthritis. Curr Rheumatol Rep 2008;10:37–42.
Di Mauro D, Bitto L, D’Andrea L, et al. Behaviour
of nitric oxide synthase isoforms in inflammatory human joint diseases: an immunohistochemical study. Ital J Anat Embryol. 2006;111:111–123.
Doom M, de Bruin T, de Rooster H, et al.
Immunopathological mechanisms in dogs with
rupture of the cranial cruciate ligament. Vet
Immunol Immunopathol 2008;125:143–161.
Foos MJ, Hickox JR, Mansour PG, et al. Expression of
matrix metalloprotease and tissue inhibitor of metalloprotease genes in human anterior cruciate ligament. J Orthop Res 2001;19:642–649.
Forterre S, Zurbriggen A, Spreng D. In vitro effect
of different mediators of apoptosis on canine cranial and caudal cruciate ligament fibroblasts and
87
its reversibility by pancaspase inhibitor zVAD.fmk.
Vet Immunol Immunopathol 2011;139:264–270.
Forterre S, Zurbriggen A, Spreng D. Nitric oxide
induces cell death in canine cruciate ligament cells
by activation of tyrosine kinase and reactive oxygen species. BMC Vet Res 2012;8:40.
Fujita Y, Hara Y, Nezu Y, et al. Proinflammatory cytokine activities, matrix metalloproteinase3 activity, and sulfated glycosaminoglycan content in synovial fluid of dogs with naturally
acquired cranial cruciate ligament rupture. Vet
Surg 2006;35:369–376.
Goggs R, Carter SD, Schulze-Tanzil G, et al. Apoptosis and the loss of chondrocyte survival signals contribute to articular cartilage degradation in
osteoarthritis. Vet J 2003;166:140–158.
Gyger O, Botteron C, Doherr M, et al. Detection and
distribution of apoptotic cell death in normal and
diseased canine cranial cruciate ligaments. Vet J
2007;174:371–377.
Hancock CM, Riegger-Krugh C. Modulation of pain
in osteoarthritis: the role of nitric oxide. Clin J Pain
2008;24:353–365.
Hayashi K, Manley PA, Muir P. Cranial cruciate ligament pathophysiology in dogs with cruciate disease: a review. J Am Anim Hosp Assoc 2004;40:385–
390.
Hasegawa A, Nakahara H, Kinoshita M, et al. Cellular and extracellular matrix changes in anterior
cruciate ligaments during human knee aging and
osteoarthritis. Arthritis Res Ther 2013;15:R29.
Häuselmann HJ, Stefanovic-Racic M, Michel BA, et al.
Differences in nitric oxide production by superficial and deep human articular chondrocytes: implications for proteoglycan turnover in inflammatory
joint diseases. J Immunol 1998;160:1444–1448.
Hofer D, Forterre S, Schweighauser A, et al. Selective iNOS-inhibition does not influence apoptosis
in ruptured canine cranial cruciate ligaments. Vet
Comp Orthop Traumatol 2009;22:198–203.
Itoh T, Matsuda H, Tanioka M, et al. The role of matrix
metalloproteinase-2 and matrix metalloproteinase9 in antibody-induced arthritis. J Immunol
2002;169:2643–2647.
Krayer M, Rytz U, Oevermann A, et al. Apoptosis
of ligamentous cells of the cranial cruciate ligament from stable stifle joints of dogs with partial
cranial cruciate ligament rupture. Am J Vet Res
2008;69:625–630.
Kroncke KD, Fehsel K, Kolb-Bachofen V. Inducible
nitric oxide synthase and its product nitric oxide, a
small molecule with complex biological activities.
Biol Chem Hoppe Seyler 1995;376:327–343.
Lepetsos P, Papavassiliou AG. ROS/oxidative stress
signaling in osteoarthritis. Biochim Biophys Acta
2016;1862:576–591.
Liang Q, Wang XP, Chen TS. Resveratrol protects rabbit articular chondrocyte against sodium
nitroprusside-induced apoptosis via scavenging
ROS. Apoptosis 2014;19:1354–1363.
VetBooks.ir
88
Etiopathogenesis of Cruciate Ligament Rupture
Louis E, Remer KA, Doherr MG, et al. Nitric oxide
and metalloproteinases in canine articular ligaments: a comparison between the cranial cruciate,
the medial genual collateral and the femoral head
ligament. Vet J 2006;172:466–472.
Maneiro E, Lopez-Armada MJ, de Andres MC, et al.
Effect of nitric oxide on mitochondrial respiratory activity of human articular chondrocytes. Ann
Rheum Dis 2005;64:388–395.
Manicone AM, McGuire JK. Matrix metalloproteinases as modulators of inflammation. Semin Cell
Dev Biol 2008;19:34–41.
Marletta MA. Nitric oxide synthase structure and
mechanism. J Biol Chem 1993;268:12231–12234.
Muir P, Danova NA, Argyle DJ, et al. Collagenolytic
protease expression in cranial cruciate ligament
and stifle synovial fluid in dogs with cranial
cruciate ligament rupture. Vet Surg 2005;34:482–
490.
Murakami H, Shinomiya N, Kikuchi T, et al. Differential sensitivity to NO-induced apoptosis between
anterior cruciate and medial collateral ligament
cells. J Orthop Sci 2005;10:84–90.
Murakami K, Maeda S, Yonezawa T, et al. Synovial
fluid matrix metalloproteinase-2 and -9 activities in
dogs suffering from joint disorders. J Vet Med Sci
2016;78:1051–1054.
Murphy G, Nagase H. Reappraising metalloproteinases in rheumatoid arthritis and osteoarthritis:
destruction or repair? Nat Clin Pract Rheumatol
2008;4:128–135.
Nagase H, Visse R, Murphy G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc Res 2006;69:562–573.
Nakagawa S, Arai Y, Mazda O, et al. N-acetylcysteine
prevents nitric oxide-induced chondrocyte apoptosis and cartilage degeneration in an experimental
model of osteoarthritis. J Orthop Res 2010;28:156–
163.
Pacher P, Beckman JS, Liaudet L. Nitric oxide and
peroxynitrite in health and disease. Physiol Rev
2007;87:315–424.
Pelletier J, Jovanovic D, Fernandes JC, et al. Reduction in the structural changes of experimental osteoarthritis by a nitric oxide inhibitor.
Osteoarthritis Cartilage 1999;7:416–418.
Pelletier JP, Jovanovic DV, Lascau-Coman V, et al.
Selective inhibition of inducible nitric oxide
synthase reduces progression of experimental
osteoarthritis in vivo: possible link with the reduction in chondrocyte apoptosis and caspase 3 level.
Arthritis Rheum 2000;43:1290–1299.
Rabillard M, Danger R, Doran IP, et al. Matrix
metalloproteinase activity in stifle synovial fluid
of cranial cruciate ligament deficient dogs and
effect of postoperative doxycycline treatment. Vet
J 2012;193:271–273.
Ries C, Petrides PE. Cytokine regulation of matrix
metalloproteinase activity and its regulatory dysfunction in disease. Biol Chem Hoppe Seyler
1995;376:345–355.
Riitano MC, Pfister H, Engelhardt P, et al. Effects of
stimulus with proinflammatory mediators on nitric
oxide production and matrix metalloproteinase
activity in explants of cranial cruciate ligaments
obtained from dogs. Am J Vet Res 2002;63:1423–
1428.
Rosa SC, Judas F, Lopes MC, et al. Nitric oxide synthase isoforms and NF-kappaB activity in normal
and osteoarthritic human chondrocytes: regulation
by inducible nitric oxide. Nitric Oxide 2008;19:276–
283.
Salinardi BJ, Roush JK, Schermerhorn T, et al. Matrix
metalloproteinase and tissue inhibitor of metalloproteinase in serum and synovial fluid of
osteoarthritic dogs. Vet Comp Orthop Traumatol
2006;19:49–55.
Spreng D, Sigrist N, Jungi T, et al. Nitric oxide metabolite production in the cranial cruciate ligament, synovial membrane, and articular cartilage of dogs
with cranial cruciate ligament rupture. Am J Vet
Res 2000;61:530–536.
Taskiran D, Stefanovic-Racic M, Georgescu H, et al.
Nitric oxide mediates suppression of cartilage proteoglycan synthesis by interleukin-1. Biochem Biophys Res Commun 1994;200:142–148.
Weinberg JB, Fermor B, Guilak F. Nitric oxide synthase and cyclooxygenase interactions in cartilage and meniscus: relationships to joint physiology, arthritis, and tissue repair. Subcell Biochem
2007;42:31–62.
Whiteman M, Armstrong JS, Cheung NS, et al. Peroxynitrite mediates calcium-dependent mitochondrial dysfunction and cell death via activation of
calpains. FASEB J 2004;18:1395–1397.
Xia W, Szomor Z, Wang Y, et al. Nitric oxide enhances
collagen synthesis in cultured human tendon cells.
J Orthop Res 2006;24:159–172.
VetBooks.ir
11
Role of Antibodies to Collagen
Type I and II
Hilde de Rooster and Eithne Comerford
Introduction
One of the major limitations in many investigations on the etiopathogenesis of cruciate
rupture (CR) in dogs is that most studies have
focused on the affected stifle joint after rupture;
the end-stage of the condition. Only a few
studies have been carried out on humoral and
cellular immunopathological mechanisms in
predisposed dogs before clinical rupture of the
contralateral cranial cruciate ligament (CrCL)
(de Bruin et al. 2007a,b).
Antigenicity of collagen
The CrCL has a microstructure of collagen bundles of multiple types, but mostly type I. The
menisci are also mainly composed of collagen
type I, whereas the articular cartilage is mainly
composed of collagen type II (van Sickle et al.
1993).
The cruciate ligaments are covered by a fold
of synovial membrane and, although they have
an intra-articular position, they are extrasynovial (Alm & Strömberg 1974; Arnoczky et al.
1979). Scanning electron microscopy studies ascertained the presence of many small
holes in the enveloping membrane, allowing
infiltration of the cruciate ligaments by synovial
fluid (Kobayashi et al. 2006). Local inflammatory processes and/or trauma may result in the
exposure of macromolecules, such as collagen,
that trigger immune-mediated inflammatory
responses (Figure 11.1). Once autoantibodies have been produced, newly released
collagen type I can enhance joint inflammation
by forming immune complexes with these antibodies resulting in activation of complement
and phagocytes (Bari et al. 1989; Carter et al.
1999).
Prevalence of antibodies to collagen
types I and II
Anti-collagen type I and II antibodies have been
detected in dogs affected with CR (Niebauer
& Menzel 1982; Niebauer et al. 1987; Bari et al.
1989; de Rooster et al. 2000). Antibodies are
present in both sera and synovial fluid aspirated from the affected stifle joint, with a higher
incidence in the synovial fluid (Niebauer &
Menzel 1982; Niebauer et al. 1987; Bari et al.
1989), thus indicating local antibody production. This finding is supported by histological studies on synovial tissue from stifle joints
of dogs with CR (Tirgari 1977; Galloway &
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
89
VetBooks.ir
90
Etiopathogenesis of Cruciate Ligament Rupture
Femur
Synovial tissue
NT
CaCL
CAg
CrCL
1
Mq
3
4
B
1
Joint space
1
2
5
6
Ab
Immune complex
Tibia
Lester 1995; Lawrence et al. 1998; Hewicker et al.
1999). The main cell types detected in the synovial tissue are macrophages, T lymphocytes,
B lymphocytes and plasma cells belonging predominantly to the IgG isotype (Tirgari 1977;
Galloway & Lester 1995; Lawrence et al. 1998;
Hewicker et al. 1999; Lemburg et al. 2004). Furthermore, a significantly higher amount of IgG
and IgM has been detected in the synovial tissue of stifle joints of dogs with CR compared
to normal stifle joints (Lawrence et al. 1998). In
addition, lymphoplasmacytic synovitis seems
common in dogs with CR, with up to 67%
of patients having distinct lymphoplasmacytic
nodules within the synovial tissue (Galloway &
Lester 1995; Erne et al. 2009).
Studies on cellular immune mechanisms suggest that there is an inflammatory process in the
contralateral joints of predisposed dogs preceding detectable joint instability (de Bruin et al.
2007a). Anti-collagen type I antibodies have
been measured sequentially in the synovial
fluid aspirated from multiple joints. In predisposed dogs, higher anti-collagen type I titers
were found in the stifle joints that eventually
sustained CR, compared to the titers in a remote
joint (de Bruin et al. 2007a).
Relevance of antibodies to collagen
types I and II
It remains uncertain whether antibodies play
an active role in the initiation of CR. Prospective
studies on dogs which initially presented with
unilateral CR did not provide evidence for this,
Figure 11.1 Schematic representation of
immune-mediated inflammatory responses in dogs
with cranial cruciate ligament (CrCL) rupture. Step 1,
impaired CrCL with release of collagen type I (CAg);
Step 2, collagen uptake by macrophage (Mq); Step 3,
antigen presentation to naive T cell (NT); Step 4, B
cell (B) activation/differentiation with antibody
production (Ab); Step 5, release of antibodies in
synovial tissue; Step 6, release of antibodies in the
synovial fluid and formation of immune complexes
with collagen type I. CaCL, caudal cruciate ligament.
as not all dogs with high antibodies developed contralateral CR (de Bruin et al. 2007a).
Nevertheless, it is possible that anti-collagen
antibodies perpetuate chronic joint inflammation in some dogs with cruciate degeneration
or fiber rupture, even if collagen is not the primary arthritogenic agent. The finding of higher
anti-collagen type I titers in the stifle joints
that did not yet have a clinically detectable
CR at the time of measurement, compared to
the titers in a remote joint, suggests that there
was an inflammatory process with production of collagen-specific antibodies in these
contralateral stifle joints (de Bruin et al. 2007a).
Histologic studies on synovial tissue from
stifle joints of dogs with CR detected plasma
cells belonging predominantly to the IgG isotype (Tirgari 1977; Galloway & Lester 1995;
Lawrence et al. 1998; Hewicker et al. 1999;
Lemburg et al. 2004) and lymphoplasmacytic
nodules (Galloway & Lester 1995; Erne et al.
2009). However, to date no synovial tissue cells
from dogs with CR have been cultured to discover if they effectively produce antibodies and,
if so, against which antigens.
Anti-collagen type I and II antibodies have
also been detected in the synovial fluid of stifle
joints with arthritis secondary to arthropathies
other than CR (Niebauer et al. 1987; Bari et al.
1989), which suggests that these antibodies are
not specific for the type of joint disorder (de
Rooster et al. 2000). However, in dogs with
complete CR, unexpectedly low or undetectable
anticollagen type I antibodies titers were found
in the synovial fluid of the affected stifle (de
Bruin et al. 2007a). This either suggests that the
VetBooks.ir
Role of Antibodies to Collagen Type I and II
autoimmune response stops after the rupture,
or that antibodies cannot be detected since they
are all present in immune complexes of these
antibodies and collagen. The latter situation
seems most likely. There is recent in vitro documentation supporting the idea that CrCL remnants exposed to the intrasynovial environment
have the potential to trigger further degradation
(Breshears et al. 2010).
References
Alm A, Strömberg B. Vascular anatomy of the patellar
and cruciate ligaments. A microangiographic and
histologic investigation in the dog. Acta Chir Scand
Suppl 1974;445:25–35.
Arnoczky SP, Rubin RM, Marshall JL. Microvasculature of the cruciate ligaments and its response to
injury. An experimental study in dogs. J Bone Joint
Surg 1979;61A:1221–1229.
Bari AS, Carter SD, Bell SC, et al. Anti-type II collagen antibody in naturally occurring canine joint
diseases. Br J Rheumatol 1989;28:480–486.
Breshears LA, Cook JL, Stoker AM, et al. Detection and evaluation of matrix metalloproteinases
involved in cruciate ligament disease in dogs using
multiplex bead technology. Vet Surg 2010;39:306–
314.
Carter SD, Barnes A, Gilmore WH. Canine rheumatoid arthritis and inflammatory cytokines. Vet
Immunol Immunopathol 1999;69:201–214.
de Bruin T, de Rooster H, van Bree H, et al. Evaluation
of anticollagen type I antibody titers in synovial
fluid of both stifle joints and the left shoulder joint
of dogs with unilateral cranial cruciate disease. Am
J Vet Res 2007a;68:283–289.
de Bruin T, de Rooster H, van Bree H, et al. Lymphocyte proliferation to collagen type I in dogs.
J Vet Med A Physiol Pathol Clin Med 2007b;54:292–
296.
de Rooster H, Cox E, van Bree H. Prevalence and relevance of antibodies to type-I and -II collagen in
91
synovial fluid of dogs with cranial cruciate ligament damage. Am J Vet Res 2000;61:1456–1461.
Erne JB, Goring RL, Kennedy FA, et al. Prevalence
of lymphoplasmacytic synovitis in dogs with naturally occurring cranial cruciate ligament rupture.
J Am Vet Med Assoc 2009;235:386–390.
Galloway RH, Lester SJ. Histopathological evaluation
of canine stifle joint synovial membrane collected at
the time of repair of cranial cruciate ligament rupture. J Am Anim Hosp Assoc 1995;31:289–294.
Hewicker TM, Carter SD, Bennett D. Immunocytochemical demonstration of lymphocyte subsets
and MHC class II antigen expression in synovial
membranes from dogs with rheumatoid arthritis and degenerative joint disease. Vet Immunol
Immunopathol 1999;67:341–357.
Kobayashi S, Baba H, Uchida K, et al. Microvascular system of anterior cruciate ligament in dogs.
J Orthop Res 2006;24:1509–1520.
Lawrence D, Bao S, Canfield PJ, et al. Elevation of
immunoglobulin deposition in the synovial membrane of dogs with cranial cruciate ligament rupture. Vet Immunol Immunopathol 1998;65:89–96.
Lemburg AK, Meyer-Lindenberg A, HewickerTrautwein M. Immunohistochemical characterization of inflammatory cell populations and adhesion
molecule expression in synovial membranes from
dogs with spontaneous cranial cruciate ligament
rupture. Vet Immunol Immunopathol 2004;97:231–
240.
Niebauer GW, Menzel EJ. Immunological changes
in canine cruciate ligament rupture. Res Vet Sci
1982;32:235–241.
Niebauer GW, Wolf B, Bashey RI, et al. Antibodies to
canine collagen types I and II in dogs with spontaneous cruciate ligament rupture and osteoarthritis.
Arthritis Rheum 1987;30:319–327.
Tirgari M. Changes in the canine stifle joint following
rupture of the anterior cruciate ligament. J Small
Anim Pract 1977;19:17–26.
van Sickle DC, Delleman DH, Brown EM. Connective and supportive tissues. In: Textbook of Veterinary
Histology, Dellmann H, van Sickle DC, Brown EM,
eds. Philadelphia PA, Lea & Febiger. 1993, pp. 29–
53.
VetBooks.ir
VetBooks.ir
12
Synovitis Precedes Stifle
Instability Associated with
Cruciate Ligament Rupture
Jason A. Bleedorn
Introduction
Joint inflammation is an expected and central
feature of cruciate ligament rupture (CR) in
dogs. Inflammation involves all joint tissues
and, in particular, the synovium. Synovitis leads
to joint pain and promotes joint degradation.
However, the underlying trigger for the development of synovitis, and its contribution to disease progression, remain unclear. This chapter will describe the characteristics of synovial
inflammation in dogs with CR and its impact on
cruciate ligament and joint degeneration.
Knowledge of joint inflammation in dogs
with CR has grown substantially during the
past decade. CR represents the end-stage of a
complex disease condition and, in some cases,
a long course of disease. Many of the investigations in the field have focused on the end-stage
of the disease, representing complete mechanical or organ failure. However, clinical, radiographic and arthroscopic evidence of stifle synovitis and arthritis can be found early in the
course of the disease (Bleedorn et al. 2011).
Recent studies have used the contralateral stifle
joint as a model for studying incipient CR. The
use of arthroscopy in dogs has also increased
awareness of profound changes in the synovial membrane and allows for objective assess-
ment. These are important steps for advancing
the understanding of early changes in the joint
before the development of stifle instability associated with complete CR.
Normal synovium
The synovial membrane is a specialized collagenous tissue lining the interior and all structures within a synovial joint, except articular
cartilage. It can be identified macroscopically as
a thin (0.5–5 mm thickness), translucent, connective tissue layer with numerous villous projections (Figure 12.1) (Iwanaga et al. 2000). It
is similar to vascular or peritoneal endothelium, but lacks a continuous basement membrane (Iwanaga et al. 2000). The synovium has
two distinct layers: an inner synovial intima
containing a rich vascular, nervous, and lymphatic network, and an outer, supportive layer
that is continuous with the fibrous joint capsule
(Sutton et al. 2009). Sensory nerve endings are
abundant and located within or adjacent to the
fibrous capsular layer (Schenk et al. 1996). Synoviocytes are loosely arranged within the membrane and have an integral function in maintaining joint health (Iwanaga et al. 2000). Two
main morphologic and functional types exist: (i)
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
93
Etiopathogenesis of Cruciate Ligament Rupture
VetBooks.ir
94
CdCL
SM
LFC
CrCL
Figure 12.1 Arthroscopy image from a normal stifle
joint of a young female hound. In this lateral
compartment view, a white synovial lining lacking
vascular ingrowth or proliferation is evident. SM, synovial
membrane; LFC, lateral femoral condyle.
macrophages (type A) that are immunoreactive
and mainly phagocytic; and (ii) fibroblast-like
(type B) cells that produce collagens, fibronectin
and hyaluronan (Iwanaga et al. 2000). Collectively, the synovial membrane provides many
key functions, including the secretion of synovial fluid to lubricate and nourish joint tissues,
the clearance of intra-articular debris, and the
regulation of immunological events.
In the normal joint, cruciate ligaments are
covered by a synovial reflection, so although
being intra-articular they are extrasynovial
(Figure 12.2) (Arnoczky & Marshall 1977).
The surrounding membrane contains many
small fenestrations that allow exchange of
synovial fluid and provide nutrients to the ligaments (Kobayashi et al. 2006). Abundant vessels from the synovium and fat pad penetrate
the ligament as the predominant blood supply (Arnoczky and Marshall 1977; Kobayashi
et al. 2006). Compounds injected into the joint
space rapidly pass through the synovial membrane and enter the capillary lumen of the
cruciate ligaments. However, intravenous injections do not reach the ligament perivascular
space (Kobayashi et al. 2006). The existence
of a blood–cruciate barrier function has been
Figure 12.2 Arthroscopic image of the intercondylar
notch from a normal stifle joint of a young female hound.
Both cruciate ligaments are visible with a thin overlying
synovial reflection. Several filamentous synovial
projections are present with the adjacent infrapatellar fat
pad. CrCL, cranial cruciate ligament; CdCL, caudal
cruciate ligament.
postulated to be analogous to the blood–
brain barrier (Kobayashi et al. 2006), and may
be important in the pathophysiology of CR.
Although debated, it is likely that joint inflammation has an adverse effect on synovial barrier function and metabolism of the cruciate
ligaments.
Synovitis
Synovitis is characterized by infiltration of the
synovial membrane with inflammatory cells,
resulting in vascularization and hyperplasia of
the synovium (Sutton et al. 2009). In dogs with
CR and osteoarthritis (OA), the cellular distribution is typically a mononuclear infiltrate of B
and T lymphocytes, macrophages, and plasma
cells (Figure 12.3) (Sutton et al. 2009). Synovial fluid contains byproducts of this inflammatory response. Although total nucleated cell
counts are often normal or mildly increased
(<5000 cells μl–1 ), this does not accurately reflect
the true magnitude of joint inflammation.
Many studies have demonstrated evidence
of immune dysregulation in the synovial
VetBooks.ir
Synovitis Precedes Stifle Instability Associated with Cruciate Ligament Rupture
(A)
95
(B)
300μm
100μm
Figure 12.3 Biopsy specimens from dog with complete cranial cruciate ligament rupture. (A) There is marked cellular
infiltration and lymphoid nodule formation resulting in expansion of the synovial intimal margin. (B) Higher magnification
of the area designated by the box in panel (A) demonstrates a focal region of predominantly mononuclear cell
infiltration. Frozen section with hematoxylin and eosin stain. Low magnification, scale bar = 300 μm; high magnification,
scale bar = 100 μm. Source: Bleedorn et al. 2011. Reproduced with permission from John Wiley & Sons, Inc.
tissues of dogs with CR. The synovial fluid
contains immune complexes and antibodies
to collagen types I and II (Neibauer & Menzel
1982; de Rooster et al. 2000; de Bruin et al. 2007).
The inflamed synovial membrane contains
mononuclear infiltrate and, at times, nodular
lymphoplasmacytic aggregates (Galloway
& Lester 1995). Activated B and T lymphocytes and major histocompatibility complex
class II antigen-positive cells with a dendritic
morphology are also typically found. These
cell populations are similar to those found in
erosive immune-mediated polyarthritis, albeit
at lower levels (Lemburg et al. 2004; Muir
et al. 2005; Muir et al. 2011). Collectively, these
changes reflect the substantial inflammatory
changes that develop in stifle synovial tissues
of dogs with CR.
Synovitis is believed to contribute to the
development of pain, joint inflammation and
the progression of OA (Sutton et al. 2009).
Pro-inflammatory cytokines synthesized in the
synovium potentiate the cascade of biologically
active substances that contribute to degradation of the joint (Doom et al. 2008). Synovial
macrophages, the main promoters of disease
activity in human rheumatoid arthritis, may
have a similar role in OA (Bondeson et al. 2006).
Synovial macrophage numbers are increased
in the joint capsule of dogs with CR, and are
associated with the severity of OA (Klocke
et al. 2005). Furthermore, macrophage-like cells
in the synovium produce matrix-degradative
enzymes (Muir et al. 2005). It is likely this
hostile environment results in the progression
of OA and may have deleterious effects on
cranial cruciate ligament (CrCL) homeostasis.
Use of the canine stifle as a translational
model for OA research provides useful information regarding the pathogenesis of CR.
Experimental CrCL transection leads to joint
instability, synovitis, and osteophyte formation (Gardner et al. 1984; Lipowitz et al. 1985;
Myers et al. 1990). Similarly, the induction of an
immune synovitis results in a significant reduction in CrCL strength and leads to structural
failure and mid-substance rupture (Goldberg
et al. 1982). Decades ago, Arnoczky and others eloquently showed that the synovium
provides a vigorous and extensive vascular
response to iatrogenic cruciate injury, which is
decreased with synovial resection (Arnoczky
et al. 1979). Recent evidence in a canine model
demonstrated that synovial debridement alone
leads to joint effusion, pain, lameness, and
compromised clinical function, comparable
to partial cruciate resection (Bozynski et al.
2015). Stifle radiographic arthritis and cruciate
VetBooks.ir
96
Etiopathogenesis of Cruciate Ligament Rupture
histologic scores were also higher with synovial
debridement than in sham controls, but less
severe than in dogs with a partial cruciate
transection (Bozynski et al. 2015). Although
these models may not accurately represent the
clinical scenario of degenerative non-contact
CR, they reinforce the intimate association
between synovitis and CrCL health.
Synovial assessment
Objective evaluation of the synovial membrane is not routine in clinical veterinary practice or research, despite the increased use of
arthroscopy and the importance of synovitis
in joint disease. The value of synovial tissue
assessment has been documented in humans
with OA, rheumatoid arthritis, and other joint
conditions (Guermazi et al. 2011; Hayashi et al.
2011). Ultrasound and contrast-enhanced magnetic resonance imaging (MRI) have been used
extensively to evaluate synovial membrane
pathology and joint effusion severity in the
human knee, but lack clinical validation in
dogs (Tarhan & Unlu 2003; Guermazi et al.
2011). These non-invasive modalities correlate
well with arthroscopic and histologic grading
(Karim et al. 2004; de Lange-Brokaar et al. 2014).
However, direct macroscopic evaluation of the
synovial membrane using arthroscopy remains
the ‘gold standard’ for the assessment of articular cartilage and synovium in human joints
(Ayral 1996; Ayral et al. 1996). Arthroscopy also
allows for the collection of synovial tissue for
microscopic assessment and, importantly, correlates well with histologic characteristics of
disease severity (Lindblad & Hedfors 1985).
Arthroscopic features of synovitis are well
described in the human knee and defined
by three baseline parameters: intensity, extent,
and location (Ayral 1996; Ayral et al. 1996).
Af Klint developed an arthroscopic scoring
system that includes the assessment of synovial hypertrophy, vascularity, and global synovitis (af Klint et al. 2009). This method is
simple, efficient, and reliable across different
joint diseases in the clinical setting. The terms
early, late, active, or chronic synovitis are often
used to further characterize joint assessment
in people in an attempt to understand mechanisms of initiation of synovitis.
Early comparative advances have been made
to provide objective measures of synovial
inflammation in dogs. Arthroscopic features
of synovitis in dogs were identified (Bleedorn
et al. 2011) and later refined (Little et al. 2014),
using the aforementioned arthroscopic scoring
system from human knee synovitis (af Klint
et al. 2009). Identical features can be scored
with high intra- and inter-observer reliability in
the canine stifle joint (Figure 12.4) (Little et al.
2014). Although some regional variation within
the joint exists, it is unclear if this relates to
local areas of cartilage damage as in human OA
(Lindblad & Hedfors 1985). The arthroscopic
features identified correlate well with histologic
assessment in dogs (Bleedorn et al. 2011; Little et al. 2014). The need for a standardized
system for joint evaluation was a key objective of the Osteoarthritis Research Society International (OARSI) histopathology initiative in
canine research studies (Cook et al. 2010). Key
questions arise with the establishment of criteria for synovial grading. First, what are the
initial, dominant characteristics of CR? Second,
how do synovial thickening or vascular patterns relate to disease mechanisms? Finally, can
these criteria be used to classify populations by
severity or time course?
Synovitis in early cruciate rupture
The synovium in stable stifle joints with early
clinical or radiographic evidence of arthritis is
inflamed (Bleedorn et al. 2011; Little et al. 2014).
Radiographic arthritis correlates with arthroscopic observations of synovitis but generally
underestimates the severity (Bleedorn et al.
2011). In a recent case series, synovitis was
present without arthroscopically apparent fraying of the CrCL in dogs with lameness and stifle arthritis. Superficial fraying of the CrCL and,
occasionally, the caudal cruciate ligament, was
seen together with synovitis in the remaining
dogs (Bleedorn et al. 2011; Little et al. 2014).
The synovial reflection surrounding the cruciate ligaments in dogs is no longer intact in
early CR, particularly once fiber bundle damage has occurred. Interestingly, dogs with more
severe synovitis in the unstable stifle had more
severe changes in the stable contralateral joint,
suggesting that disease in joint pairs is related,
1
1
1
2
2
2
3
3
3
4
4
4
Figure 12.4 Arthroscopic appearance of stifle synovium in dogs with cruciate ligament rupture. Examples of the spectrum of arthroscopic hypertrophy (upper row),
vascularity (middle row), and synovitis (lower row) scoring in various regions of the canine stifle joint. Arthroscopic scoring ranged from 1–4. Source: Little et al. 2014;
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0097329. Used under CC BY 4.0, https://creativecommons.org/licenses/by/4.0/.
S
y
n
o
v
i
t
i
s
V
a
s
c
u
l
a
r
i
t
y
H
y
p
e
r
t
r
o
p
h
y
VetBooks.ir
Synovitis Precedes Stifle Instability Associated with Cruciate Ligament Rupture
97
VetBooks.ir
98
Etiopathogenesis of Cruciate Ligament Rupture
whereby the stable stifles represent an earlier
phase of the disease process (Bleedorn et al.
2011). Further studies are required to understand the specific features that are present early
in the disease process and what mechanisms are
responsible for this change.
A substantial proportion of affected dogs
have partial CR with a stable stifle joint. Surgical treatment for dogs with CR has historically
focused on the elimination of joint instability,
rather than the mitigation of joint inflammation. For example, Hulse and others observed
the preservation of intact CrCL fibers during
second-look arthroscopy in 17 dogs with stable
partial tears treated by tibial plateau leveling
osteotomy (TPLO), which implied some protective effect of TPLO in these cases (Hulse et al.
2010). Cartilage damage was less severe with
an intact, functional CrCL (Hulse et al. 2010). It
would have been interesting to compare serial
synovitis scores to identify a potential relationship with treatment outcomes in this study. Ultimately, arthritis progression is expected with
varying degrees of associated lameness despite
stifle stabilization in dogs with CR (Girling et al.
2006; Au et al. 2010). Whether this represents
the effects of chronic persistent synovitis or
some subtle mechanical cause is unknown.
Although mechanical instability exists in
CR stifles, a thorough understanding of the
associated joint pathology is important when
considering treatment options for individual
patients.
Conclusions
Stifle synovitis is an established feature of CR in
dogs. Synovitis occurs early during the course
of the disease, is profound, and plays a role in
the progression of joint disease and eventual
CrCL and caudal cruciate ligament fiber rupture. Many similarities exist between CR, OA,
and immune-mediated or rheumatoid arthritis
that help to inform an understanding of the CR
disease mechanism. Synovial membrane evaluation may facilitate identification of early features associated with CR, assessment of disease severity, and allow for outcome assessment following disease-modifying treatment.
The underlying trigger for the development of
synovitis and its mechanistic contribution to
disease progression should be a focus of future
work.
References
af Klint E, Catrina A, Matt P, et al. Evaluation of
arthroscopy and macroscopic scoring. Arthritis Res
Ther 2009;11:1–13.
Arnoczky SP, Marshall JL. The cruciate ligaments
of the canine stifle: An anatomical and functional
analysis. Am J Vet Res 1977;38:1807–1814.
Arnoczky SP, Rubin RM, Marshall JL. Microvasculature of the cruciate ligaments and its response
to injury. J Bone Joint Surg Am 1979;61:1221–
1229.
Au KK, Gordon-Evans WJ, Dunning D, et al. Comparison of short- and long-term function and radiographic osteoarthrosis in dogs after postoperative
physical rehabilitation and tibial plateau leveling
osteotomy or lateral fabellar suture stabilization.
Vet Surg 2010;39:173–180.
Ayral X. Diagnostic and quantitative arthroscopy:
quantitative arthroscopy. Baillières Clin Rheumatol 1996;10:477–494.
Ayral X, Mayoux-Benhamou A, Dougados M.
Proposed scoring system for assessing synovial
membrane abnormalities at arthroscopy in knee
osteoarthritis. Br J Rheumatol 1996;35:14–17.
Bleedorn JA, Greuel EN, Manley PA, et al. Synovitis
in dogs with stable stifle joints and incipient cranial
cruciate ligament rupture: A cross-sectional study.
Vet Surg 2011;40:531–543.
Bondeson J, Wainwright SD, Lauder S, et al. The
role of synovial macrophages and macrophageproduced cytokines in driving aggrecanases,
matrix metalloproteinases, and other destructive
and inflammatory responses in osteoarthritis.
Arthritis Res Ther 2006;8:R187.
Bozynski C, Kuroki K, Stannard J, et al. Evaluation of
partial transection versus synovial debridement of
the ACL as novel canine models for management
of ACL injuries. J Knee Surg 2015;28:404–410.
Cook JL, Kuroki K, Visco D, et al. The OARSI
histopathology initiative. Osteoarthritis Cartilage
2010;18:S66–S79.
de Bruin T, van Bree H, Cox E. Evaluation of anticollagen type I antibody titers in synovial fluid of
both stifle joints and the left shoulder joint of dogs
with unilateral cranial cruciate disease. Am J Vet
Res 2007;68:283–389.
de Lange-Brokaar BJE, Ioan-Facsinay A, Yusuf E,
et al. Degree of synovitis on MRI by comprehensive
whole knee semi-quantitative scoring method correlates with histologic and macroscopic features of
synovial tissue in knee osteoarthritis. Osteoarthritis Cartilage 2014;22:1606–1613.
de Rooster H, Cox E, van Bree H. Prevalence and relevance of antibodies to type-I and -II collagen in
VetBooks.ir
Synovitis Precedes Stifle Instability Associated with Cruciate Ligament Rupture
synovial fluid of dogs with cranial cruciate ligament damage. Am J Vet Res 2000;61:1456–1461.
Doom M, de Bruin T, de Rooster H, et al.
Immunopathological mechanisms in dogs with
rupture of the cranial cruciate ligament. Vet
Immunol Immunopathol 2008;125:143–161.
Galloway RH, Lester SJ. Histopathological evaluation of canine stifle joint synovial membrane collected at the time of repair of cranial cruciate ligament rupture. J Am Anim Hosp Assoc 1995;31:289–
294.
Gardner DL, Bradley WA, O’Conner P, et al. Synovitis after surgical division of the anterior cruciate
ligament of the dog. Clin Exp Rheumatol 1984;2:
11–15.
Girling SL, Bell SC, Whitelock RG, et al. Use of
biochemical markers of osteoarthritis to investigate the potential disease-modifying effect of tibial plateau levelling osteotomy. J Small Anim Pract
2006;47:708–714.
Goldberg VM, Burstein A, Dawson M. The influence
of an experimental immune synovitis on the failure mode and strength of the rabbit anterior cruciate ligament. J Bone Joint Surg Br 1982;64:900–
906.
Guermazi A, Roemer FW, Hayashi D, et al. Assessment of synovitis with contrast-enhanced MRI
using a whole-joint semiquantitative scoring system in people with, or at high risk of, knee
osteoarthritis: the MOST study. Ann Rheum Dis
2011;70:805–811.
Hayashi D, Roemer FW, Katur A, et al. Imaging of
synovitis in osteoarthritis: Current status and outlook. Semin Arthritis Rheum 2011;41:116–130.
Hulse D, Beale BS, Kerwin S. Second-look arthroscopic findings after tibial plateau leveling
osteotomy. Vet Surg 2010;39:350–354.
Iwanaga T, Shikichi M, Katamura H, et al. Morphology and functional roles of synoviocytes in the
joint. Arch Histol Cytol 2000;63:17–31.
Karim Z, Wakefield RJ, Quinn M, et al. Validation and reproducibility of ultrasonography in the
detection of synovitis in the knee: A comparison
with arthroscopy and clinical examination. Arthritis Rheum 2004;50:387–394.
Klocke NW, Snyder PW, Widmer WR, et al. Detection of synovial macrophages in the joint capsule
of dogs with naturally occurring rupture of the cranial cruciate ligament. Am J Vet Res 2005;66:493–
499.
99
Kobayashi S, Baba H, Uchida K, et al. Microvascular system of anterior cruciate ligament in dogs. J
Orthop Res 2006;24:1509–1520.
Lemburg AK, Meyer-Lindenberg A, HewickerTrautwein M. Immunohistochemical characterization of inflammatory cell populations and adhesion
molecule expression in synovial membranes from
dogs with spontaneous cranial cruciate ligament
rupture. Vet Immunol Immunopathol 2004;97:231–
240.
Lindblad S, Hedfors E. Intraarticular variation in synovitis: Local macroscopic and microscopic signs of
inflammatory activity are significantly correlated.
Arthritis Rheum 1985;28:977–86.
Lipowitz AJ, Wong PL, Stevens JB. Synovial membrane changes after experimental transection of the
cranial cruciate ligament in dogs. Am J Vet Res
1985;46:1166–1170.
Little JP, Bleedorn JA, Sutherland BJ, et al. Arthroscopic assessment of stifle synovitis in dogs with
cranial cruciate ligament rupture. PLoS One 2014;
9:e97329.
Muir P, Kelly JL, Marvel SJ, et al. Lymphocyte populations in joint tissues from dogs with inflammatory
stifle arthritis and associated degenerative cranial
cruciate ligament rupture. Vet Surg 2011;40:753–
761.
Muir P, Schamberger GM, Manley PA, et al. Localization of cathepsin K and tartrate-resistant acid phosphatase in synovium and cranial cruciate ligament
in dogs with cruciate disease. Vet Surg 2005;34:239–
246.
Myers SL, Brandt KD, O’Connor BL, et al. Synovitis
and osteoarthritic changes in canine articular cartilage after anterior cruciate ligament transection.
Arthritis Rheum 1990;33:1406–1415.
Neibauer GW, Menzel EJ. Immunological changes
in canine cruciate ligament rupture. Res Vet Sci
1982;32:235–241.
Schenk I, Spaethe A, Halata Z. The structure of sensory nerve endings in the knee joint capsule of the
dog. Ann Anat 1996;178:515–521.
Sutton S, Clutterbuck A, Harris P, et al. The contribution of the synovium, synovial derived inflammatory cytokines and neuropeptides to the pathogenesis of osteoarthritis. Vet J 2009;179:10–24.
Tarhan S, Unlu Z. Magnetic resonance imaging
and ultrasonographic evaluation of the patients
with knee osteoarthritis: a comparative study. Clin
Rheumatol 2003; 22:181–188.
VetBooks.ir
VetBooks.ir
13
Role of Synovial Immune
Responses in Stifle Synovitis
Peter Muir
Introduction
The historical paradigm for the cruciate ligament rupture (CR) mechanism has been that
ligament rupture is largely a consequence of
trauma, with arthritis developing secondary to
joint instability. However, a growing body of
evidence suggests that this relationship is incorrect, and that in dogs with naturally occurring
CR, synovitis and arthritis typically precede the
development of complete ligament rupture and
associated stifle instability. In dogs with CR,
epidemiological studies suggest that if subtle
radiographic change is present in the contralateral stifle, the risk of contralateral rupture at 16
months is as high as 65% (Doverspike et al. 1993;
Chuang et al. 2014). Whilst it is clear that cranial
cruciate ligament (CrCL) transection and associated stifle instability contributes to the development of synovitis (Lipowitz et al. 1985), the
growing use of arthroscopy for stifle evaluation
in the dog, and the use of tibial plateau leveling osteotomy surgery to treat dogs with partial
CR and a stable stifle, has led to a greater appreciation that synovitis is present in stable stifles
of affected dogs (Bleedorn et al. 2011). The cruciate ligaments are intra-articular, but extrasynovial, and are covered in synovium. Experimentally, persistent synovitis induces a substantial
degradation of CrCL tensile strength (Goldberg
et al. 1982). The deleterious effects of chronic
joint inflammation on the tissue matrix of the
cruciate ligaments is likely due to disruption
of the blood–cruciate barrier in the ligament
microvasculature, such that cruciate ligament
metabolism is closely related to changes in synovial fluid (Kobayashi et al. 2006).
A logical extension of this shift in thinking
is to focus on understanding the disease mechanism that leads to the development of stifle synovitis in dogs. Current evidence suggests that synovial immune responses promote
progressive degradation of intra-articular structures over time, including the cruciate ligaments (Doom et al. 2008).
Inflammatory cell populations within
the stifle joint
Synovitis involves the intima of the CrCL
epiligament. The inflammatory cell population is typically a mixed mononuclear one,
and includes activated tartrate-resistant acid
phosphatase-positive (TRAP) macrophages
(Figure 13.1), T and B lymphocytes (Figure 13.2), plasma cells, and major histocompatibility complex (MHC) class II-positive
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
101
(B)
VetBooks.ir
(A)
Figure 13.1 Photomicrographs of frozen sections of (A) synovium and (B) ruptured cranial cruciate ligament (CrCL)
from a 5-year-old dog with cruciate ligament rupture. (A) In this specimen, aggregates of mononuclear cells are present
in the synovial intima (white arrows), including activated macrophages stained red for tartrate-resistant acid phosphatase
(TRAP) (black arrows). (B) In ruptured CrCL from the same dog, aggregates of TRAP+ activated macrophages can also be
seen infiltrating the CrCL. TRAP histochemical stain, with Mayer’s hematoxylin counterstain; scale bar = 100 μm. Panel
(A) source: Muir et al. 2005. Reproduced with permission from John Wiley & Sons, Inc.
Synovial tissue
Femur
Stimulation
Inhibition
AMq
TGF-β
NT
MO
IFN-γ
Ag presentation
CaCl
CD4+T
IL-10
PDGF
bFGF
TGF-β
IL-4
DC
IFN-γ
CAg
IFN-γ
IL-1Ra, sIL-1R,
sTNF-αR
IGFs
B
IL-8
F
Proteinase
inhibitors
IL-1,TNF-α
PC
IL-10 IL-8
Matrix
synthesis
Ab
IL-1Ra, sIL-1R,
sTNF-αR
Proteinase
Cartilage degradation
IL-6
C
Tibia
Joint space
S
Proliferation
and formation of
joint fibrosis
Figure 13.2 Schematic representation of the possible cytokine cascade in dogs with cruciate ligament rupture (begin at
antigen presentation in the synovial tissue; red lines: stimulation; black lines: inhibition; red boxes: pro-inflammatory;
yellow boxes: anti-inflammatory). Antigen-stimulated dendritic cells present antigens to naive T lymphocytes. Activated
CD4+ T lymphocytes can then stimulate different cells (macrophages, monocytes, B lymphocytes, fibroblasts and
synoviocytes) by cytokine release to produce antibodies, osteophytes, ligament degeneration and synovial tissue
proliferation (red lines). Next to the pro-inflammatory reactions, anti-inflammatory responses are seen (black lines). Ab,
antibodies; Ag, antigen; AMq, activated macrophage; B, B lymphocyte; bFGF, basic fibroblast growth factor; C,
chondrocyte; CaCL, caudal cruciate ligament; CAg, collagen antigen; CD4+ T, CD4+ T lymphocyte; DC, dendritic cell;
IFN-γ, interferon gamma; IGFs, insulin-like growth factors; IL, interleukin; IL-1Ra, interleukin 1 receptor antagonist; F,
fibroblast; Mo, monocyte; NT, naı̈ve T lymphocyte; PC, plasma cell; PDGF, platelet-derived growth factor; S,
synoviocyte; sIL-1R, soluble IL-1 receptor; sTNF-αR, soluble TNF-α receptor; TGF-β, transforming growth factor beta;
TNF-α, tumor necrosis factor alpha. Source: Doom et al. 2008. Reproduced with permission from Elsevier.
VetBooks.ir
Role of Synovial Immune Responses in Stifle Synovitis
103
dendritic cells (Faldyna et al. 2004; Lemburg
et al. 2004; Klocke et al. 2005; Muir et al. 2005;
Muir et al. 2007a; Muir et al. 2009; Muir et al.
2011). The proportion of T lymphocytes within
synovial tissues is increased in dogs with CR
compared with samples from healthy dogs
(Faldyna et al. 2004). Expression of the T-cell
antigen receptor complex is also increased in
synovium and synovial fluid in affected dogs
(Muir et al. 2009). While lymphocytes play a
key role in antigen-specific immunity, activated
macrophages and their inflammatory products
play a key role in innate immunity and the
pathogenesis of tissue inflammation.
et al. 2007b). A polymicrobial population of
bacteria, many of which that are not recognized joint pathogens, is typically present, particularly Gram-negative organisms (Muir et al.
2010). Similar microbial populations are found
in human arthritic joints (Kempsell et al. 2000). It
seems most likely that the translocation of small
amounts of bacterial material to the stifle synovium from the circulation may act to maintain
synovial inflammation, but not necessarily initiate disease (Bhandal et al. 2013).
Antigen-specific immune responses
within joint tissues
Although antigen-specific immune responses
within the stifle have a role in the development
of synovial inflammation in dogs with CR,
innate immune responses within the stifle
synovium are also likely important. Patternrecognition receptors (PRR) are expressed
by leukocytes and epithelial cells, and are
used by the innate immune system to detect the
presence of infection (Akira et al. 2006). The activation of PRR contributes to disease pathology
in inflammatory and autoimmune conditions
(e.g., Bryant & Fitzgerald 2009). The activation
of PRR, such as toll-like receptor (TLR) and
nucleotide-binding oligomerization domain
(NOD) -containing proteins leads to the activation of nuclear factor kappa B (NFκβ) and
upregulation of immune response genes and
pro-inflammatory cytokines. Innate immune
responses to PRR also regulate subsequent
adaptive immune responses via dendritic cell
signaling (Iwasaki & Medzhitov 2015). Defective PRR function has been implicated in various chronic inflammatory conditions, such as
Crohn’s disease in human beings and perianal
fistulae in dogs (House et al. 2008). Analysis of
synovial fluid cells from dogs with CR suggests
that expression of TRAP is increased relative to
that in healthy dogs and dogs with osteoarthritis (Figure 13.3A) (Muir et al. 2007a). Higher
expression of TLR-2 in arthritic joints was also
been found (Figure 13.3B) (Muir et al. 2007a).
Increased expression of complement component 3, CXCL8, which is primarily expressed by
macrophages, and intercellular cell adhesion
molecule-1 (ICAM-1), is also found in the
synovium of dogs with CR (El-Hadi et al. 2012;
The upregulation of T lymphocytes within
joints is a key pro-inflammatory feature of
arthritis, and also occurs in joint diseases that
have traditionally been considered to be associated with minimal inflammation (Sakkas &
Platsoukas 2007). The identification of large
populations of lymphocytes within synovial tissues of dogs with CR suggests that the disturbance of antigen-specific immune responses is
an important component of the disease mechanism. A MHC class II genetic risk has been
identified in many immune-mediated joint diseases in human beings. Although immunogenetic risk for inflammatory arthritis exists in
dogs (Ollier et al. 2001), MHC class II immunogenetic risk with canine CR was not confirmed
in a recent study (Clements et al. 2011). However, MHC class I immunogenetic association
has not been investigated in dogs with CR to
date.
At the present time, the explanatory mechanism for chronic stifle synovitis in dogs with
CR remains a critical but unanswered question.
Several studies have explored the hypothesis
that neo-epitopes of type I and type II collagen may be important in this regard (Niebauer
et al. 1987; de Bruin et al. 2007a,b) (see Chapter 11). Collectively, these studies have not confirmed that neo-epitopes of collagen are the primary immunological trigger in dogs with CR,
and further investigations are needed.
The translocation of bacterial material into
the stifle joint is a common event in dogs (Muir
Innate immune responses within joint
tissues
Etiopathogenesis of Cruciate Ligament Rupture
(A)
TRAP Expression
(18S rRNA normalized)
(A)
p < 0.05
1000
p < 0.005
5 μm
100
10
1
0.1
0.01
(B)
300
Relative TLR-2 Expression
(18S rRNA normalized)
VetBooks.ir
104
250
#Stifle oligoarthritis Healthy
(n = 27)
(n = 8)
Other arthritis
(n = 9)
(B)
500 nm
200
150
p = 0.08
100
50
0
#Stifle oligoarthritis Healthy
(n = 21)
(n = 9)
Other arthritis
(n = 9)
Figure 13.3 (A) Relative expression of tartrate-resistant
acid phosphatase (TRAP), and (B) toll-like receptor 2
(TLR-2) in synovial fluid cells collected from dogs with
stifle (oligo) arthritis and cruciate ligament rupture,
healthy dogs, and dogs with other forms of arthritis
characterized by cartilage loss (osteoarthritis). Gene
expression was normalized to peripheral blood
mononuclear cells (PBMC) as an internal control using
the −ΔΔCt method. 18S rRNA was used as the
house-keeping gene. # indicates a significant difference
from internal PBMC controls (P < 0.05). Boxes represent
median and the 25th and 75th percentiles. Whiskers
represent 10th and 90th percentiles. Outliers are also
plotted. Significant differences between groups are as
indicated. Source: Muir et al. 2007a. Reproduced with
permission from Elsevier.
Figure 13.4 Sub-rupture loading of tendon and
ligament collagen creates strain-induced discrete
plasticity damage with kinked collagen fibrils (Veres et al.
2013). In an in vitro study, macrophage-like U937 cells
found on collagen fibrils with strain-induced discrete
plasticity were morphologically distinct from those found
on undamaged fibrils. The cells showed a greater
uniformity, being mostly of the ruffled type (∗ in panel A).
Rather than maintaining a rounded shape, as on the
undamaged fibrils, many of the ruffled cells had acquired
a dome-shape, increasing their contact area with the
damaged fibrils (arrows in panel A). (B) Magnified view of
the boxed location in panel (A) showing structure of the
discrete plasticity fibril array that formed the substrate for
these cells. Source: Veres et al. 2015. Reproduced with
permission from John Wiley & Sons, Inc.
Garner et al. 2013). Collectively, these observations suggest that macrophage activation and
neutrophil trafficking are important factors in
the development of chronic stifle synovitis in
dogs with CR.
Collagen in ruptured CrCL tissue appears
damaged, with loss of crimp in collagen
fibers (Hayashi et al. 2003). Interestingly,
recent research has shown that repeated subrupture overload of ligament/tendon induces
nanoscale discrete plasticity damage to collagen
fibrils (Veres et al. 2013). U937 macrophage-like
cells recognize collagen fibrils with straininduced plasticity damage, bind to damaged
areas for collagen degradation, alter their functional morphology (Figure 13.4), and secrete
matrix, which is hypothesized to be fibronectin
in vitro (Veres et al. 2015). Further studies are
needed to understand how macrophages and
fibroblasts interact with mechanically damaged collagen when ligament homeostasis is
disturbed in dogs with CR.
VetBooks.ir
Role of Synovial Immune Responses in Stifle Synovitis
In conclusion, both antigen-specific and
innate immune responses within the stifle synovium overlying the cruciate ligament complex
appear important to the development of synovitis and joint degeneration over time. In this
regard, the overlying synovium has an important barrier function (Bozynski et al. 2015) that
is poorly understood. A functional connection
between ligament loading and disturbances to
ligament homeostasis, that includes the development of inflammation in the synovium overlying the cruciate ligaments, may occur through
macrophages, since macrophages respond to
specific motifs in mechanically damaged collagen. T lymphocytes and macrophages likely
represent important therapeutic targets in dogs
with CR. If disturbances to ligament homeostasis, matrix remodeling and the development
of synovitis can be successfully managed with
medical therapy, then such a treatment may
block the development of CR and associated
joint instability in affected dogs.
References
Akira S, Uematus S, Takeuchi O. Pathogen recognition and innate immunity. Cell 2006;124:783–
801.
Bhandal J, Hayashi K, Kim S-Y, et al. Detection of bacterial DNA by PCR in dogs with stifle pathology.
Vet Surg 2013;42:814–818.
Bleedorn JA, Greuel EN, Manley PA, et al. Synovitis
in dogs with stable stifle joints and incipient cranial
cruciate ligament rupture: A cross-sectional study.
Vet Surg 2011;40,531–543.
Boyzynski CC, Kuroki K, Stannard JP, et al. Evaluation of partial transection versus synovial debridement of the ACL as novel canine models for management of ACL injuries. J Knee Surg 2015;28:404–
410.
de Bruin T, de Rooster H, van Bree H, et al. Evaluation of anticollagen type I antibody titers in synovial fluid of both stifles and the left shoulder of
dogs with unilateral cranial cruciate disease. Am J
Vet Res 2007a;68:283–289.
de Bruin T, de Rooster H, van Bree H, et al. Lymphocyte proliferation to collagen type I in dogs. J Vet
Med A 2007b;54:292–296.
Bryant C, Fitzgerald KA. Molecular mechanisms
involved in inflammasome activation. Trends Cell
Biol 2009;19:455–464.
Chuang C, Ramaker MA, Kaur S, et al. Radiographic
risk factors for contralateral rupture in dogs with
unilateral cranial cruciate ligament rupture. PLoS
One 2014;9: e106389.
105
Clements DN, Kennedy LJ, Short AD, et al. Risk
of canine cruciate ligament rupture is not associated with the major histocompatibility complex.
Vet Comp Orthop Traumatol 2011;24:262–265.
Doom M, de Bruin T, de Rooster H, et al.
Immunopathological mechanisms in dogs with
rupture of the cranial cruciate ligament. Vet
Immunol Immunopathol 2008;125:143–161.
Doverspike M, Vasseur PB, Walls CM. Contralateral cranial cruciate ligament rupture: Incidence
in 114 dogs. J Am Anim Hosp Assoc 1993;29:167–
170.
El-Hadi M, Charavaryamath C, Aebischer A, et al.
Expression of interleukin 8 and intercellular cell
adhesion molecule-1 in the synovial membrane
and cranial cruciate ligament of dogs after rupture
of the ligament. Can J Vet Res 2012;76:8–15.
Faldyna M, Zatloukal J, Leva L, et al. Lymphocyte subsets in stifle joint synovial fluid of dogs with spontaneous rupture of the cranial cruciate ligament.
Acta Vet Brno 2004;73:79–84.
Garner BC, Kuroki K, Stoker AM, et al. Expression of
proteins in serum, synovial fluid, synovial membrane, and articular cartilage samples obtained
from dogs with stifle joint osteoarthritis secondary
to cranial cruciate ligament disease and dogs without stifle arthritis. Am J Vet Res 2013;74:386–
394.
Goldberg VM, Burstein A, Dawson M. The influence
of an experimental immune synovitis on the failure
mode and strength of the rabbit anterior cruciate
ligament. J Bone Joint Surg 1982;64A:900–906.
Hayashi K, Frank JD, Dubinsky C, et al. Histologic
changes in ruptured canine cranial cruciate ligament. Vet Surg 2003;32:269–277.
House AK, Gregory SP, Catchpole B. Patternrecognition receptor mRNA expression and function in canine monocyte/macrophages and relevance to canine anal furunculosis. Vet Immunol
Immunopathol 2008;124:230–240.
Iwasaki A, Medzhitov R. Control of adaptive immunity by the innate immune system. Nat Immunol
2015;16:343–353.
Kempsell KE, Cox CJ, Hurle M, et al. Reverse
transcriptase-PCR analysis of bacterial rRNA
for detection and characterization of bacterial
species in arthritis synovial tissue. Infect Immun
2000;68:6012–6026.
Klocke NW, Snyder PW, Widmer WR, et al. Detection of synovial macrophages in the joint capsule of
dogs with naturally occurring rupture of the cranial
cruciate ligament. Am J Vet Res 2005;66:493–499.
Kobayashi S, Baba H, Uchida K, K, et al. Microvascular system of the anterior cruciate ligament in dogs.
J. Orthop Res 2006;24:1509–1520.
Lemburg AK, Meyer-Linenberg A, HewickerTrautwein M. Immunohistochemical characterization of inflammatory cell populations and adhesion
molecule expression in synovial membranes from
dogs with spontaneous cranial cruciate ligament
VetBooks.ir
106
Etiopathogenesis of Cruciate Ligament Rupture
rupture. Vet Immunol Immunopathol 2004;97:231–
240.
Lipowitz AJ, Wong PL, Stevens JB. Synovial membrane changes after experimental transection of the
cranial cruciate ligament in dogs. Am J Vet Res
1985;46:1166–1170.
Muir P, Schamberger GM, Manley PA, et al. Localization of cathepsin K and tartrate-resistant acid phosphatase in synovium and cranial cruciate ligament
in dogs with cruciate disease. Vet Surg 2005;34:239–
246.
Muir P, Kelly JL, Marvel SJ, et al. Lymphocyte populations in joint tissues from dogs with inflammatory
stifle arthritis and associated degenerative cranial
cruciate ligament rupture. Vet Surg 2011;40,753–
761.
Muir P, Schaefer SL, Manley PA, et al. Expression of
immune response genes in the stifle joint of dogs
with oligoarthritis and degenerative cranial cruciate ligament rupture. Vet Immunol Immunopathol
2007a;119:214–221.
Muir P, Oldenhoff WE, Hudson AP, et al. Detection of
DNA from a range of bacterial species in the knee
joints of dogs with inflammatory knee arthritis and
associated degenerative anterior cruciate ligament
rupture. Microb Pathog 2007b;42:47–55.
Muir P, Schaefer SL, Manley PA, et al. T Lymphocyte antigen receptor expression in dogs with
inflammatory stifle arthritis and degenerative cranial cruciate ligament rupture. Vet Surg 2009;38:
E40.
Muir P, Rox R, Wu Q, et al. Seasonal variation in
detection of bacterial DNA in the stifle joints of
dogs with inflammatory arthritis and degenerative cranial cruciate ligament rupture. Vet Microbiol 2010;141:127–133.
Niebauer GW, Wolf B, Bashey RI, et al. Antibodies to
canine collagen types I and II in dogs with spontaneous cruciate ligament rupture and osteoarthritis.
Arthritis Rheum 1987;30:319–327.
Ollier WER, Kennedy LJ, Thomson W, et al. Dog MHC
alleles containing the human RA shared epitope
confer susceptibility to canine rheumatoid arthritis.
Immunogenetics 2001;53:669–673.
Sakkas LI, Platsoucas CD. The role of T cells in
the pathogenesis of osteoarthritis. Arthritis Rheum
2007;56:409–424.
Veres SP, Harrison JM, Lee JM. Repeated subrupture overload causes progression of nanoscaled discrete plasticity damage in tendon collagen fibrils.
J Orthop Res 2013;31:731–737.
Veres SP, Brennan-Pierce EP, Lee JM. Macrophagelike U937 cells recognize collagen fibrials with
strain-induced
discrete
plasticity
damage.
J Biomed Mater Res A 2015;103:397–408.
VetBooks.ir
Section III
Clinical Features
Introduction
Over the past 25 years, veterinarians have
become increasingly aware that it is difficult
to relate the typical clinical features of cruciate
ligament rupture (CR) in dogs with the concept
that stifle osteoarthritis (OA) is simply a consequence of ligament rupture and stifle instability.
Moderate to severe OA is often found at initial
presentation in dogs with CR. Advances in
diagnostic imaging, including the development of methods for stress radiography of the
stifle, have helped to more thoroughly determine the extent of cranial cruciate ligament
fiber rupture during patient evaluation. It is
important to relate any knowledge of ligament
biomechanics to assessment of the cruciate
ligaments clinically in dogs with stifle OA. By
definition, unstable joints have experienced
complete ligament rupture. Since publication
of the First Edition of this book, several studies
have shown that radiographic changes in
partial CR stifles are quite predictive of risk for
complete CR. Collectively, these studies have
also defined a clinical model for the evaluation
of disease-modifying therapy for the early
phase of the disease. Recent research findings
have shed new light on which components of
stifle pathology in affected dogs contribute to
joint pain and lameness. This section provides
a detailed discussion of the clinical features
of CR.
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell. 107
VetBooks.ir
VetBooks.ir
14
Epidemiology of Cruciate
Ligament Rupture
Lauren A. Baker and Peter Muir
Introduction
Cruciate ligament rupture (CR) is one of the
most common causes of pelvic limb lameness
in dogs (Witsberger et al. 2008). The condition
is a chronic, progressive disease that results
in eventual rupture of the cranial cruciate ligament (CrCL) (Bleedorn et al. 2011; Comerford et al. 2011; Muir et al. 2011). A great deal
of time and effort has been spent characterizing the epidemiological aspects of canine CR.
Through these investigations, it has been determined that CR is a complex disease process
with multiple contributing genetic and environmental risk factors. Furthermore, it is clear
that there is no single combination of risk factors that will invariably lead to CrCL degeneration and eventual ligament rupture. Every
dog should be considered an individual with a
certain amount of inborn genetic risk on which
environmental variables act to influence development of the disease. The following paragraphs include a summary of investigations of
risk factors known to contribute to CR. A thorough understanding of these risk factors can aid
in the identification of dogs with increased sus-
ceptibility to the condition, and thereby guide
patient management.
Age
As CR is a chronic degenerative process, it follows that it is a condition of primarily middleaged dogs (Whitehair et al. 1993; Reif & Probst
2003; Witsberger et al. 2008). A study examining medical records data of over one million
dogs reported that dogs aged 1–4 years were
significantly less likely than dogs in other age
groups to experience CR (Witsberger et al. 2008).
While the peak age of onset for CR has been
reported at 7–10 years (Whitehair et al. 1993),
a more recent study of 166 Labrador Retrievers
reported a peak age of onset of approximately
4 years. Notably, only 6% of these dogs had an
age of onset over 8 years, and there were no
dogs over 10 years of age. This suggests that
older dogs are also at a decreased risk for CR
(Reif & Probst 2003). Notably, there is an interaction with age and other risk factors. For example, large-breed dogs tend to present at younger
ages than small breeds (Duval et al. 1999). Dogs
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
109
VetBooks.ir
110
Clinical Features
that experience bilateral CrCL rupture tend to
be younger than dogs with unilateral ruptures
(Cabrera et al. 2008; Grierson et al. 2011).
Gender
It is unclear whether gender differences have
an effect on the incidence of CR. Multiple studies have reported an increased prevalence of CR
in spayed females compared to other gender
groups (Whitehair et al. 1993; Lampman et al.
2003; Powers et al. 2005; Adams et al. 2011),
while others have reported no significant differences (Witsberger et al. 2008) or an increased
risk in males (Grierson et al. 2011). The majority of study results agree that neutered dogs of
either gender are at increased odds of developing CR compared to intact dogs (Whitehair
et al. 1993; Duval et al. 1999; Lampman et al.
2003; Slauterbeck et al. 2004; Duerr et al. 2007;
Witsberger et al. 2008; de la Riva et al. 2013).
A recent study of 360 Golden Retrievers (de
la Riva et al. 2013) reported that early neutering (<1 year) significantly increased the likelihood of CR. In fact, there was no occurrence of
CR in studied dogs that were intact (n = 122).
Occurrence in early neutered males and females
was reported at 5.1% and 7.7%, respectively. The
effect of early neutering persisted after adjusting for differences in body condition score (de
la Riva et al. 2013). This is an important observation, as weight gain is often cited as an explanation for the increased incidence of orthopaedic
disease among neutered dogs (Whitehair et al.
1993; Duval et al. 1999; Buote et al. 2009). If not
through weight gain, how does early neutering affect the CrCL? It has been suggested that
an absence of gonadal hormones leads to atypical growth plate closure and thus altered conformation (de la Riva et al. 2013). Indeed, early
neutering has been reported to be a significant
risk factor for the development of excessive tibial plateau angles in large-breed dogs (Duerr
et al. 2007). Additionally, an absence of gonadal
hormones may affect the size, shape, or material properties of the CrCL itself (Slauterbeck
et al. 2004). A study investigating the effect of
gonadectomy on CrCL collagen homeostasis in
rabbits found that collagen concentrations were
lower and fiber diameters greater in the absence
of gonadal hormones, which may predispose
them to rupture (Light et al. 2012). Research confirming a direct role for gonadal hormones on
the canine CrCL matrix architecture is not currently available.
Obesity
An association between higher body weight
and increased risk of CR has been reported
(Whitehair et al. 1993; Duval et al. 1999). While
this is an important finding, evaluating weight
alone does not distinguish between large-size
dogs and dogs that are truly overweight. Other
work has attempted to evaluate body condition
more objectively. A study of 755 dogs reported
that those with overweight or obese body condition scores were twice as likely to be diagnosed
with CR compared to dogs of normal weight
(Lampman et al. 2003). A similar study evaluated body weight as a percentage of recommended breed weight and found that dogs in
the obese category were nearly fourfold more
likely to sustain a CR compared to dogs of normal weight (Adams et al. 2011). Mechanical, as
well as metabolic, factors explain the increased
risk associated with obesity. From a mechanical
standpoint, obese animals experience increased
loading in their limbs, which in turn may overstress the CrCL and predispose it to rupture
(Whitehair et al. 1993; Adams et al. 2011). Additionally, there has been interest in the endocrine
function of adipose tissue and its role in CR
pathophysiology. Pro-inflammatory adipokines
released by adipose tissue may contribute to the
degenerative process underlying CR (Pallu et al.
2010; Adams et al. 2011; Comerford et al. 2011;
Koskinen et al. 2011).
Conformation
The anatomy of the stifle joint has been evaluated extensively for risk factors that may
be associated with the development of CR.
Anatomic features investigated include intercondylar notch dimensions (Comerford et al.
2006; Lewis et al. 2008), overall limb alignment
(Dismukes et al. 2008; Mostafa et al. 2009), and
proximal tibial conformation (Selmi & Padilha
Filho 2001; Macias et al. 2002; Reif & Probst
2003; Dennler et al. 2006; Osmond et al. 2006;
VetBooks.ir
Epidemiology of Cruciate Ligament Rupture
111
Table 14.1 Potential risk factors for cruciate ligament rupture in dogs based on current evidence.
Category
Potential risk factors
Age
4–8 years
Reproductive status
Neutered (before 1 year may increase further)
Breed
Newfoundland
Rottweiler
Labrador Retriever
Bulldog
Boxer
Chow Chow
American Staffordshire Terrier
Weight
>22 kg
Body condition
Overweight or obese
Intended function
Unknown
Stifle anatomy
Narrow intercondylar notch
Excessive tibial plateau angle (degree varies among
reports, >28◦ , >32◦ , >35◦ )
Relatively small proximal tibial craniocaudal width
Cranial angulation of the proximal tibia
Distal femoral torsion
Schwandt et al. 2006; Guerrero et al. 2007; Cabrera et al. 2008; Inauen et al. 2009; Ragetly et al.
2011; Fuller et al. 2014b; Haynes et al. 2015).
Anatomic factors that are associated with a predisposition to CR include a narrow intercondylar notch, excessive or pathologic (i.e., outside
the 95% confidence intervals for the population)
tibial plateau angle, a relatively small proximal tibial width, cranial angulation of the proximal tibia, and distal femoral torsion (Table 14.1).
While a great number of studies have focused
on the effects of tibial plateau angle and patellar
tendon angle, no study has definitively shown
either of these as significant risk factors for CR
in dogs. Theories and ex vivo research have
suggested that increased CrCL strain and an
increased shear component of total joint force
when each of these angles is considered high
based on reference ranges in dogs (Warzee
et al. 2001; Reif & Probst 2003; Kowaleski et al.
2005; Shahar & Milgram 2006; Apelt et al. 2007;
Duerr et al. 2007; Kim et al. 2008; Kipfer et al.
2008; Haynes et al. 2015). One study reported
that a multiple logistic regression model using
the combination of tibial plateau angle and
femoral anteversion angle was able to discriminate between case and control limbs with an
area under the ROC curve of 96% (Ragetly
et al. 2011). This suggested that a multivariate
approach may provide further insight into the
effect of tibial morphology as a risk factor. Other
studies have reported no significant effect of
proximal tibial morphology on the risk of CrCL
rupture (Wilke et al. 2002; Reif & Probst 2003;
Guastella et al. 2008; Fuller et al. 2014a). The
wide spectrum of results supporting or negating the effect of conformational variables on
the risk of CR provides further support for the
overall complexity of the condition. While bony
conformation may contribute to CR in some
way, there remains no definitive evidence that
it is a primary causal factor.
Bilateral CrCL rupture
Perhaps one of the greatest risk factors for
developing a CR is having already been diagnosed with the condition. The incidence of
bilateral ruptures diagnosed on initial clinical
presentation is in the range of 11% to 17% (de
Bruin et al. 2007; Cabrera et al. 2008; Buote et al.
2009). The incidence of contralateral rupture
after initial diagnosis is between 22% and
54% (de Bruin et al. 2007; Cabrera et al. 2008;
Buote et al. 2009; Grierson et al. 2011; Fuller
VetBooks.ir
112
Clinical Features
et al. 2014b). Dogs diagnosed with unilateral
CR often have signs of moderate to severe
osteoarthritis (OA) in the stable contralateral
stifle (de Bruin et al. 2007; Grierson et al. 2011;
Muir et al. 2011; Fuller et al. 2014a; Chuang et al.
2014). The median time to contralateral CR has
been reported in the range of 405 to 1688 days
(Grierson et al. 2011; Muir et al. 2011; Fuller et al.
2014a). Stifle synovitis is likely an early event
that contributes to the progression of CR (Erne
et al. 2009; Bleedorn et al. 2011; Muir et al. 2011;
Little et al. 2014). The radiographic assessment
of OA present in stable stifle joints is correlated
with arthroscopic assessment of synovitis (Bleedorn et al. 2011). Therefore, dogs at greater risk
for bilateral rupture can be identified through
radiographic assessment. The presence of
radiographic synovial effusion and osteophytosis in the stable contralateral stifle at the time
of diagnosis is a significant risk factor for the
development of contralateral CR (Chuang et al.
2014; Fuller et al. 2014a), with more severe radiographic change associated with decreased time
to contralateral rupture (Chuang et al. 2014).
These results support the practice of obtaining
bilateral stifle radiographs when evaluating a
dog for unilateral CR. The evaluation of both
joints for OA is valuable for patient management, as well as client education, and represents the ‘gold standard’ of care in small animal
practice.
Genetics
The aforementioned risk factors primarily affect
CR disease progression. The only risk factor
that seems to affect the initiation of CR is
genetic effects from breed. It has long been recognized that certain breeds (e.g., Newfoundlands, Rottweilers, and Labrador Retrievers) are
predisposed to CR while others, such as the
Greyhound, are almost never diagnosed with
the condition (Whitehair et al. 1993; Witsberger
et al. 2008). Many recent studies have been performed to characterize the genetic basis of CR
(Wilke et al. 2009; Baird et al. 2014; Baker et al.
2017). The heritability of CR is moderate, with
estimates calculated for the Boxer, Newfoundland, and Labrador Retriever ranging from 0.26
to 0.48 (Nielen et al. 2003; Wilke et al. 2006; Baker
et al. 2017). Genome-wide association studies
have been carried out in the Newfoundland and
the Labrador Retriever (Baird et al. 2014; Baker
et al. 2017), the results of which suggest that
canine CR is a highly polygenic complex trait.
Genetic risk is variable for each individual, and
this risk sets the stage for environmental influence, the progression of disease, and eventual
rupture. A full discussion on the genetics of CR
is presented in Chapter 7.
References
Adams P, Bolus R, Middleton S, et al. Influence of signalment on developing cranial cruciate rupture in
dogs in the UK. J Small Anim Pract 2011;52:347–
352.
Apelt D, Kowaleski MP, Boudrieau RJ. Effect of tibial tuberosity advancement on cranial tibial subluxation in canine cranial cruciate-deficient stifle
joints: an in vitro experimental study. Vet Surg
2007;36:170–177.
Baird AEG, Carter SD, Innes JF, et al. Genome-wide
association study identifies genomic regions of
association for cruciate ligament rupture in Newfoundland dogs. Anim Genet 2014;45:542–549.
Baker LA, Kirkpatrick B, Rosa GJM, et al. Genomewide association analysis in dogs implicates 99 loci
as risk variants for Anterior Cruciate Ligament
Rupture. PLoS One 2017;12:e0173810.
Bleedorn JA, Greuel EN, Manley PA, et al. Synovitis in
dogs with stable stifle joints and incipient cranial
cruciate ligament rupture: a cross-sectional study.
Vet Surg 2011;40:531–543.
Buote N, Fusco J, Radasch R. Age, tibial plateau angle,
sex, and weight as risk factors for contralateral rupture of the cranial cruciate ligament in Labradors.
Vet Surg 2009;38:481–489.
Cabrera SY, Owen TJ, Mueller, MG. Comparison
of tibial plateau angles in dogs with unilateral
versus bilateral cranial cruciate ligament rupture: 150 cases (2000–2006). J Am Vet Med Assoc
2008;232:889–892.
Chuang C, Ramaker MA, Kaur S, et al. Radiographic
risk factors for contralateral rupture in dogs with
unilateral cranial cruciate ligament rupture. PLoS
One 2014:9:e106389.
Comerford EJ, Tarlton JF, Avery NC, et al. Distal
femoral intercondylar notch dimensions and their
relationship to composition and metabolism of the
canine anterior cruciate ligament. Osteoarthritis
Cartilage 2006;14:273–278.
Comerford EJ, Smith K, Hayashi K. Update on
the aetiopathogenesis of canine cranial cruciate
ligament disease. Vet Comp Orthop Traumatol
2011;24:91–98.
de Bruin T, de Rooster H, van Bree H, et al.
Radiographic assessment of the progression of
VetBooks.ir
Epidemiology of Cruciate Ligament Rupture
osteoarthrosis in the contralateral stifle joint of
dogs with a ruptured cranial cruciate ligament. Vet
Rec 2007;161:745–750.
de la Riva GT, Hart BL, Farver TB, et al. Neutering dogs: effects on joint disorders and cancers in
Golden Retrievers. PLoS One 2013;8:e55937.
Dennler R, Kipfer NM, Tepic S, et al. Inclination of the
patellar ligament in relation to flexion angle in stifle
joints of dogs without degenerative joint disease.
Am J Vet Res 2006;67:1849–1854.
Dismukes DI, Fox DB, Tomlinson JL, et al. Determination of pelvic limb alignment in the large-breed
dog: a cadaveric radiographic study in the frontal
plane. Vet Surg 2008;37:674–682.
Duerr FM, Duncan CG, Savicky RS, et al. Risk factors for excessive tibial plateau angle in large-breed
dogs with cranial cruciate ligament disease. J Am
Vet Med Assoc 2007;231:1688–1691.
Duval JM, Budsberg SC, Flo GL, et al. Breed, sex, and
body weight as risk factors for rupture of the cranial cruciate ligament in young dogs. J Am Vet Med
Assoc 1999;215:811–814.
Erne JB, Goring RL, Kennedy FA, et al. Prevalence
of lymphoplasmacytic synovitis in dogs with naturally occurring cranial cruciate ligament rupture.
J Am Vet Med Assoc 2009;235:386–390.
Fuller MC, Hayashi K, Bruecker KA, et al. Evaluation
of the radiographic infrapatellar fat pad sign of the
contralateral stifle joint as a risk factor for subsequent contralateral cranial cruciate ligament rupture in dogs with unilateral rupture: 96 cases (2006–
2007). J Am Vet Med Assoc 2014a;244;328–338.
Fuller MC, Kapatkin AS, Bruecker KA, et al. Comparison of the tibial mechanical joint orientation angles
in dogs with cranial cruciate ligament rupture. Can
Vet J 2014b;55:757–764.
Grierson J, Asher L, Grainger K. An investigation into
risk factors for bilateral canine cruciate ligament
rupture. Vet Comp Orthop Traumatol 2011;24:192–
196.
Guastella DB, Fox DB, Cook JL. Tibial plateau angle
in four common canine breeds with cranial cruciate ligament rupture, and its relationship to meniscal tears. Vet Comp Orthop Traumatol 2008;21:125–
128.
Guerrero TG, Geyer H, Hässig M, et al. Effect of conformation of the distal portion of the femur and
proximal portion of the tibia on the pathogenesis
of cranial cruciate ligament disease in dogs. Am J
Vet Res 2007;68:1332–1337.
Haynes KH, Biskup J, Freeman A, et al. Effect of tibial
plateau angle on cranial cruciate ligament strain: an
ex vivo study in the dog. Vet Surg 2015;44:46–49.
Inauen R, Koch D, Bass M, et al. Tibial tuberosity conformation as a risk factor for cranial cruciate ligament rupture in the dog. Vet Comp Orthop Traumatol 2009;22:16–20.
Kim SE, Pozzi A, Kowaleski MP, et al. Tibial
osteotomies for cranial cruciate ligament insufficiency in dogs. Vet Surg 2008;37:111–125.
113
Kipfer NM, Tepic S, Damur DM, et al. Effect of tibial tuberosity advancement on femorotibial shear
in cranial cruciate-deficient stifles. An in vitro study.
Vet Comp Orthop Traumatol 2008;21:385–290.
Koskinen A, Juslin S, Nieminen R, et al. Adiponectin
associates with markers of cartilage degradation
in osteoarthritis and induces production of proinflammatory and catabolic factors through mitogenactivated protein kinase pathways. Arthritis Res
Ther 2011;13:R184.
Kowaleski MP, Apelt D, Mattoon JS, et al. The effect
of tibial plateau leveling osteotomy position on cranial tibial subluxation: an in vitro study. Vet Surg
2005;34:332–336.
Lampman TJ, Lund EM, Lipowitz AJ. Cranial cruciate disease: current status of diagnosis, surgery,
and risk for disease. Vet Comp Orthop Traumatol
2003;16:122–126.
Lewis BA, Allen DA, Henrikson TD, et al. Computed
tomographic evaluation of the canine intercondylar notch in normal and cruciate deficient stifles. Vet
Comp Orthop Traumatol 2008;21:119–124.
Light VA, Montgomery RD, Akingbemi BT. Sex hormone regulation of collagen concentrations in cranial cruciate ligaments of sexually immature male
rabbits. Am J Vet Res 2012;73:1186–1193.
Little JP, Bleedorn JA, Sutherland BJ, et al. Arthroscopic assessment of stifle synovitis in dogs
with cranial cruciate ligament rupture. PLoS One
2014;9:e97329.
Macias C, McKee WM, May C. Caudal proximal tibial
deformity and cranial cruciate ligament rupture in
small-breed dogs. J Small Anim Pract 2002;43:433–
438.
Mostafa AA, Griffon DJ, Thomas MW, et al. Morphometric characteristics of the pelvic limbs of
Labrador Retrievers with and without cranial cruciate ligament rupture. Am J Vet Res 2009;70:498–
507.
Muir P, Schwartz Z, Malek S, et al. Contralateral
cruciate survival in dogs with unilateral noncontact cranial cruciate ligament rupture. PLoS
One 2011;6:e25331.
Nielen AL, Knol BW, van Hagen MA et al. Genetic
and epidemiological investigation of a birth cohort
of boxers. Tijdschr Diergeneeskd 2003:128;586–590.
Osmond CS, Marcellin-Little DJ, Harrysson OL, et al.
Morphometric assessment of the proximal portion of the tibia in dogs with and without cranial
cruciate ligament rupture. Vet Radiol Ultrasound
2006;47:136–141.
Pallu S, Francin PJ, Guillaume C, et al. Obesity
affects the chondrocyte responsiveness to leptin
in patients with osteoarthritis. Arthritis Res Ther
2010;12:R112.
Powers MY, Martinez SA, Lincoln JD, et al. Prevalence
of cranial cruciate ligament rupture in a population of dogs with lameness previously attributed to
hip dysplasia: 369 cases (1994–2003). J Am Vet Med
Assoc 2005;227:1109–1111.
VetBooks.ir
114
Clinical Features
Ragetly CA, Evans R, Mostafa AA, et al. Multivariate analysis of morphometric characteristics
to evaluate risk factors for cranial cruciate ligament deficiency in Labrador Retrievers. Vet Surg
2011;40:327–333.
Reif U, Probst CW. Comparison of tibial plateau
angles in normal and cranial cruciate deficient
stifles of Labrador Retrievers. Vet Surg 2003;32:385–
389.
Schwandt CS, Bohorquez-Vanelli A, Tepic S, et al.
Angle between the patellar ligament and tibial
plateau in dogs with partial rupture of the cranial cruciate ligament. Am J Vet Res 2006;67:1855–
1860.
Selmi AL, Padilha Filho JG. Rupture of the cranial
cruciate ligament associated with deformity of the
proximal tibia in five dogs. J Small Anim Pract
2001;42:390–393.
Shahar R, Milgram J. Biomechanics of tibial plateau
leveling of the canine cruciate-deficient stifle
joint: a theoretical model. Vet Surg 2006;35:144–
149.
Slauterbeck JR, Pankratz K, Xu KT, et al. Canine
ovariohysterectomy and orchiectomy increases the
prevalence of ACL injury. Clin Orthop Relat Res
2004;429:301–305.
Warzee CC, Dejardin LM, Arnoczky SP, et al. Effect
of tibial plateau leveling on cranial and caudal
tibial thrusts in canine cranial cruciate-deficient
stifles: an in vitro experimental study. Vet Surg
2001;30:278–286.
Whitehair JG, Vasseur PB, Willits NH. Epidemiology
of cranial cruciate ligament rupture in dogs. J Am
Vet Med Assoc 1993;203:1016–1019.
Wilke VL, Conzemius MG, Besancon MF, et al.
Comparison of tibial plateau angle between clinically normal Greyhounds and Labrador Retrievers with and without rupture of the cranial cruciate ligament. J Am Vet Med Assoc 2002;221:1426–
1429.
Wilke VL, Conzemius MG, Kinghorn BP, et al. Inheritance of rupture of the cranial cruciate ligament in
Newfoundlands. J Am Vet Med Assoc 2006;228:61–
64.
Wilke VL, Zhang S, Evans RB, et al. Identification of
chromosomal regions associated with cranial cruciate ligament rupture in a population of Newfoundlands. Am J Vet Res 2009;70:1013–1017.
Witsberger TH, Villamil JA, Schultz LG, et al. Prevalence of and risk factors for hip dysplasia and cranial cruciate ligament deficiency in dogs. J Am Vet
Med Assoc 2008;232:1818–1824.
VetBooks.ir
15
History and Clinical Signs of
Cruciate Ligament Rupture
Peter Muir
Introduction
Cruciate ligament rupture (CR) has been recognized since the early part of the twentieth
century. Although this condition was initially
considered a traumatic injury, during the past
25 years it has become widely accepted that
it is a complex trait disease with both genetic
and environmental contributions to the risk of
disease, with development of stifle instability
because of progressive fiber tearing in the cruciate ligament complex (Bennett et al. 1988). It is
important to exclude CR before making recommendations about the management of hip dysplasia in dogs because of the high prevalence of
CR and associated stifle arthritis in dogs with
pelvic limb lameness and hip dysplasia (Powers et al. 2005).
History
Although owners will often provide a history
suggestive of trauma, careful analysis typically
reveals that the onset of lameness was either
insidious, or that lameness was observed to
develop by the owner after an incident of minor
trauma associated with normal daily activity. In a proportion of patients, owners will
provide a clear history of major trauma, such as
injury in a motor vehicle accident, suggesting
that a traumatic rupture of the cranial cruciate
ligament (CrCL) has occurred. This is rare, and
further investigation of such patients will often
reveal an avulsion fracture of a cruciate ligament attachment site. Epidemiologically, this
proportion is not clearly documented, although
in medium- to large-breed dogs this incidence
appears less than 1% of patients; a very large
majority of dogs do not have a history of trauma
or contact injury. Currently, CR is considered a
progressive, acquired, degenerative condition.
Lameness in affected dogs is usually weightbearing and is typically worse after exercise.
The duration of lameness described by owners is highly variable. Occasionally, owners may
report an audible ‘clicking’ during walking.
It is also common for dogs to be presented
for treatment because of subtle pelvic lameness, which is usually continuously present and
fairly unresponsive to medical therapy with
nonsteroidal anti-inflammatory drugs. Observant owners may notice that bilateral lameness
is present, with the dog exhibiting a stiff pelvic
limb gait with weight-shifting to the thoracic
limbs. Lameness may also appear to shift from
one pelvic limb to the ipsilateral limb in patients
with bilateral CR. Such patients typically have
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
115
VetBooks.ir
116
Clinical Features
stifle arthritis, but a stable stifle with a partial
CR on further investigation.
Clinical signs
On physical examination, affected dogs usually
exhibit unilateral or bilateral weight-bearing
pelvic limb lameness. If the lameness is bilateral, dogs will often lean forward and alter their
stance to unload the pelvic limbs (Figure 15.1).
Occasionally, a non weight-bearing lameness
may be evident. In dogs with unilateral lameness, external rotation of the affected limb may
be evident when walking. Similarly, during
sitting, affected dogs will often position the
affected limb so that limb is externally rotated
and stifle flexion is reduced, compared with a
normal symmetric sitting posture. This is sometimes referred to as the ‘sit test’. In this posture,
the calcaneus is not directly underneath the
tuber ischii, because the stifle is not fully flexed.
On general examination, atrophy of pelvic limb
musculature in the affected limb(s) is usually
evident. Occasionally, an audible clicking may
be heard during walking or during stifle manipulation, and is usually indicative of meniscal
damage, most commonly a bucket-handle tear.
Careful physical examination is important as
neurological disease may initially be suspected
in dogs that have difficulty rising from a sitting
to a standing position because of bilateral CR.
During examination of the stifle, effusion is
typically found, with the lateral and medial
margins of the patella tendon feeling indistinct
on palpation. Subtle effusion can be hard to
Figure 15.1 Photograph of a female Rottweiler with
bilateral pelvic limb lameness and bilateral cruciate
ligament rupture. Notice that she is leaning forward to
unload the pelvic limbs.
detect on physical examination, but is an important clinical sign. Stifle radiography is a more
sensitive diagnostic test for stifle effusion than
physical examination. As CR is so prevalent,
if there is any uncertainty about this aspect
of stifle examination, bilateral orthogonal stifle radiographs should be made in dogs with
pelvic limb lameness and examined for effusion
and arthritic degeneration. Radiographs also
underestimate pathological change, so an obvious stifle synovitis may be present, with only
subtle radiographic change. Even very mild stifle synovial effusion should be considered an
important sign of partial CR (Chuang et al. 2014)
(see also Chapter 16).
Palpation of the medial side of the stifle will
often reveal a firm thickening, indicative of
periarticular fibrosis (Figure 15.2) or ‘medial
buttress.’ This pathological change is almost
always indicative of CR. Crepitation and resentment to range of motion manipulation may be
found on flexion and extension of the stifle. CR
may also lead to excessive internal rotation of
the tibia relative to the femur, which may be
apparent on physical examination. In dogs with
partial CR and a stable stifle, internal rotation of
the tibia relative to the femur or stifle hyperextension will usually elicit resentment as load is
applied to the CrCL with these joint manipulations (see also Chapter 16).
Medial and lateral stress to the stifle should
also be applied during physical examination to
assess the stability of the collateral ligaments
Figure 15.2 Photograph of the medial aspect of the
right stifle. Prominent periarticular fibrosis of the stifle is
evident. It is important to check for firm swelling of the
medial aspect of the stifle or ‘medial buttress.’ This sign is
typical of chronic cruciate ligament rupture.
117
VetBooks.ir
History and Clinical Signs of Cruciate Ligament Rupture
Figure 15.3 Photograph of the left pelvic limb of a
Siberian Husky. When checking for cranial drawer
motion in the stifle, it is important to place the fingertips
on the tibial crest, the fibular head, the patella, and the
lateral fabella to avoid interpreting compression of soft
tissue or internal rotation as cranial drawer motion.
of the stifle, as collateral ligament rupture combined with cruciate ligament rupture can be a
consequence of traumatic injury to the stifle.
Cranial-caudal instability between the
tibia and femur may be identified by use of
the cranial drawer test or the cranial tibial
thrust test (Figures 15.3 and 15.4, respectively)
(Henderson & Milton 1978; Muir 1997). During application of these tests to the stifle, it
is important to place the examining fingers
directly on the bony prominences of the stifle,
to avoid interpreting movement of the skin and
overlying soft tissues as translation of the tibia
relative to the femur. It is often helpful to repeat
these tests after sedation or general anesthesia
of the patient to ensure that subtle instability
has not been missed on physical examination. This is particularly important in dogs
with chronic stifle arthritis. Here, periarticular
fibrosis may reduce, but not eliminate, cranial
translation of the tibia relative to the femur. It
is also important in nervous dogs with tense
muscles, where stifle instability may be less
apparent.
The cranial drawer and cranial tibial thrust
tests are best performed with the dog in lateral
recumbency and the stifle in partial flexion at a
Figure 15.4 Photograph of the left pelvic limb of a
Siberian Husky. With the stifle extended, an index finger
is placed on the tibial crest to determine whether cranial
displacement of the tibia occurs when the hock is flexed.
If cranial translation of the tibia relative to the femur is
identified, this is a positive cranial tibial thrust test and is
indicative of cranial cruciate ligament rupture.
normal standing angle. Testing should be performed in both flexion and extension, although
instability at any stifle flexion angle likely
reflects complete CR (Heffron & Campbell
1978).
Detection of stifle instability and cranial
translation of the tibia relative to the femur is
indicative of complete biomechanical disruption of the CrCL. In young puppies, a small
degree of cranial translation of the tibia relative to the femur of a few millimeters is normal
and is indicative of mild laxity in the ligament.
Here, the small amount of tibio-femoral translation during the cranial drawer maneuver will
come to an abrupt stop. In contrast, in dogs with
partial CR (Grade II sprain), the small degree
of tibio-femoral translation will end in a soft or
spongy stop (see also Chapter 16).
During physical examination, the stifle
should also be palpated carefully for caudal drawer motion. Here, the cranial drawer
test will elicit an abrupt stop with minimal
VetBooks.ir
118
Clinical Features
translation, whereas caudal drawer motion will
be elicited. Isolated rupture of the caudal cruciate ligament (CaCL) is rare. A small proportion
of dogs affected with the CR condition and
diagnosed with CrCL rupture will also have
CaCL rupture. In CR dogs with rupture of both
cruciate ligaments, it can be particularly difficult to recognize that both cruciate ligaments
are ruptured during physical examination of
the stifle (Might et al. 2013).
Conclusions
Detection of cranial drawer and cranial tibial
thrust on physical examination remains a key
part of patient investigation in dogs with CR.
However, the detection of stifle instability can
often be difficult to distinguish from mild laxity, which might be normal in puppies, or a soft
stop to the cranial drawer test (Grade II sprain).
The cranial drawer test alone or in combination with the cranial tibial thrust test poorly
differentiates cranial and caudal cruciate rupture in model studies (Might et al. 2013). Therefore, clinical findings from these tests should be
interpreted with caution and the diagnosis of
CR should also consider other physical examination findings and observations from other
diagnostic testing, particularly orthogonal stifle radiographs. These limitations will likely
change in the future as knowledge of stifle
kinematics improves, as discussed elsewhere in
the book. Development of better teaching models for veterinary students may also enhance
clinical diagnosis of CR over time (Troy & Berg
2015). In future investigations, development of
a stifle arthrometer that objectively measures
subtle translation of the tibia relative to the
femur may aid early identification of dogs with
partial CR.
References
Bennett D, Tennant B, Lewis DG, et al. A reappraisal
of anterior cruciate ligament disease in the dog.
J Small Anim Pract 1988;29:275–297.
Chuang C, Ramaker MA, Kaur S, et al. Radiographic
risk factors for contralateral rupture in dogs with
unilateral cranial cruciate ligament rupture. PLoS
One 2014;9:e106389.
Heffron LE, Campbell JR. Morphology, histology, and
functional anatomy of the canine cranial cruciate
ligament. Vet Rec 1978;102:280–283.
Henderson RA, Milton JL. The tibial compression
mechanism: A diagnostic aid in stifle injuries. J Am
Anim Hosp Assoc 1978;14:474–479.
Might KR, Bachelez A, Martinez SA, et al. Evaluation
of the drawer test and the tibial compression test
for differentiating between cranial and caudal stifle subluxation associated with cruciate ligament
instability. Vet Surg 2013;42:392–397.
Muir P. Physical examination of lame dogs. Compend
Cont Ed Pract Vet 1997;19:1149–1161.
Powers MY, Martinez SA, Lincoln JD, et al. Prevalence
of cranial cruciate ligament rupture in a population of dogs with lameness previously attributed to
hip dysplasia: 369 cases (1994–2003). J Am Vet Med
Assoc 2005;227:1109–1111.
Troy JR, Bergh MS. Development and efficacy of a
canine pelvic limb model used to teach the cranial drawer and tibial compression tests in the stifle
joint. J Vet Med Educ 2015;42:127–132.
VetBooks.ir
16
Partial Rupture of the Cranial
Cruciate Ligament
Peter Muir
Introduction
Ligament sprains are classified as Grade I
through III, depending on the severity of the
matrix damage. Ligament sprains are defined
biomechanically. Grade I sprains do not affect
joint instability and are associated with subfailure damage to the ligament tissue (Provenzano et al. 2002). Grade II sprains are associated
with moderate fiber damage and a stretch to the
point of detectable instability. Grade III sprains
are associated with severe disruption of ligament fibers and obvious joint laxity (Provenzano et al. 2002). Consequently, dogs with a
stable stifle have partial cruciate ligament rupture (CR) and dogs with an unstable stifle
have complete CR. Historically, CR has been
classified as partial or complete, based on an
anatomic definition in some reports. In human
beings, the assessment and grading of partial
anterior cruciate ligament injuries is controversial, as these lesions may involve a variable
amount of the cross-section of the ligament during arthroscopic evaluation (Hong et al. 2003).
Partial cranial cruciate ligament rupture
In the dog, the cranial cruciate ligament
(CrCL) has cranio-medial and caudo-lateral
components containing bundles of longitudinally orientated collagen fibers (Heffron
& Campbell 1978). The cranio-medial component is taut in both flexion and extension,
whereas the caudo-lateral component is only
taut in extension (Arnoczky & Marshall 1977).
Biomechanically, ex vivo sectioning of either the
cranio-medial component or the caudo-lateral
component of the CrCL induces the development of mild joint instability in partial flexion,
with ≤3 mm of cranial drawer motion that is little influenced by stifle flexion angle (Heffron &
Campbell 1978). This small amount of cranial
drawer motion would be difficult to detect
on physical examination (Table 16.1) (Heffron & Campbell 1978). Collectively, these
observations suggest that clinicians can infer
that the majority of the CrCL has been disrupted biomechanically when cranial drawer
instability is detected by physical examination
(Heffron & Campbell 1978). In the human
patient, joint translation can also be measured
using an arthrometer (Bach et al. 1990). In
dogs, the development of weight-bearing
standing radiography (Kim et al. 2011) or
recumbent stress radiography (Bleedorn et al.
2011) have helped quantify cranial tibial subluxation in affected dogs. Future development
of an arthrometer for the dog stifle that can
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
119
VetBooks.ir
120
Clinical Features
Table 16.1 Results of partial and total sectioning of the canine cranial cruciate ligament (CrCL).
Degree of stifle flexion from maximal extension
Cranio-medial component cut (n = 5)
0◦
20◦
40◦
60◦
1.5 (0,2)
2 (2,3)
1 (1,2.5)
1 (0,1)
Caudo-lateral component cut (n = 5)
0 (0,1.5)
1 (1,1)
0.5 (0,1)
0 (0,0)
Whole CrCL cut (n = 10)
7.7 ± 3.4
13.0 ± 1.4
10.4 ± 2.0
7.6 ± 1.6
Note: Results represent cranial translation of the tibia relative to the femur in millimeters. For the whole CrCL cut, data
represent mean ± standard deviation. For the other two experiments, data represent median (range). Source: Heffron &
Campbell 1978. Reproduced with permission from the British Veterinary Association.
objectively measure cranial tibial translation
may further aid in the early diagnosis of canine
partial CR.
Clinically, diagnosis of partial rupture of
the CrCL (Grade I sprain) should be limited
to dogs that are determined to have a stable
stifle with no cranial drawer or cranial tibial
thrust. The detection of cranial drawer motion
in only partial flexion is not a reliable indicator
of disruption to only the cranio-medial component of the CrCL (Scavelli et al. 1990). During
cranial drawer testing of the stifle, a soft stop
to the test can be detected with minimal to
no cranial translation of the tibia. This clinical
finding reflects more severe matrix damage to
the CrCL (Grade II sprain). Although it has
been previously questioned whether a lack
of cranial drawer motion during the physical
examination of dogs with partial CrCL rupture
(A)
(B)
may be a consequence of periarticular fibrosis
(Scavelli et al. 1990), some degree of clinical
instability is typically found in dogs with
chronic CR (Tashman et al. 2004).
Radiographically, stifle synovial effusion and
osteophyte formation are important signs that
support the diagnosis of partial CR. Even subtle radiographic change should be considered
clinically important (Chuang et al. 2014). CrCL
fiber damage can be inferred from degenerative
changes radiographically (Sample et al. 2017).
The increasing use of arthroscopy to examine
the stifle joint of dogs with mild arthritis and
a clinically stable stifle suggests that superficial
fraying of the CrCL and the caudal cruciate ligament (see also Chapter 17), superficial and deep
splits in the ligament tissue, and fiber rupture
are typically seen in the early phase of the condition (Figure 16.1) (Bleedorn et al. 2011).
(C)
Figure 16.1 Arthroscopic images of the intercondylar notch region of the distal femur of three dogs with partial cranial
cruciate ligament (CrCL) rupture. No cranial drawer or cranial tibial thrust was evident on physical examination. All of
the dogs had complete contralateral cruciate ligament rupture and an unstable stifle. Disruption of fibers or fiber bundles
is evident in the CrCL (arrows) (A,B). Splits in the fiber bundles often become more evident when examined with an
arthroscopic probe (C). Inflammation of adjacent synovium is typically evident (A). Ruptured fiber bundles often have a
pale yellow appearance (B). Thickening of the ends of torn fibers suggests a healing response that is not successful at
repair and remodeling of fiber bundles (∗ ). In this regard, the surrounding synovial fluid is known to promote fibrinolysis
of any provisional scaffold for repair of fiber damage. Right stifle (A,B), left stifle (C). CaCL, caudal cruciate ligament.
VetBooks.ir
Partial Rupture of the Cranial Cruciate Ligament
Conclusions
In conclusion, if stifle joint instability is detected
clinically, this is indicative of substantial disruption to the CrCL biomechanically, and complete
CR. In this type of patient, the remaining
ligament tissue, if present, is typically stretched
out and slack. The remaining CrCL fibers often
have an abnormal arthroscopic appearance,
have a yellow coloration, and are inflamed.
The diagnosis of partial CR should be limited
to stifles that are stable. In the future, careful
evaluation of clinical outcomes after the treatment of dogs with partial CR using surgical
stabilization, particularly tibial plateau leveling
osteotomy, is needed, as there is some evidence
that this approach may protect the CrCL from
progressive fiber tearing (Hulse et al. 2010;
Barger et al. 2016). Further studies are also
needed to develop disease-modifying therapies
aimed at blocking progressive deterioration in
the biomechanical properties of the CrCL and
eventual complete CR.
References
Arnoczky SP, Marshall JL. The cruciate ligaments
of the canine stifle: An anatomical and functional
analysis. Am J Vet Res 1977;38:1807–1814.
Bach BR, Warren RF, Flynn WM, et al. Arthrometric
evaluation of knees that have a torn anterior cruciate ligament. J Bone Joint Surg 1990;72A:1299–1306.
Barger B, Piazza A, Muir P. Treatment of stable partial
cruciate rupture (Grade I sprain) in five dogs with
121
tibial plateau levelling osteotomy. Vet Rec Case Rep
2016;4:e000315.
Bleedorn JA, Greuel E, Manley PA, et al. Synovitis in
dogs with stable stifle joints and incipient cranial
cruciate ligament rupture: A cross-sectional study.
Vet Surg 2011;40:531–543.
Chuang C, Ramaker MA, Kaur S, et al. Radiographic
risk factors for contralateral rupture in dogs with
unilateral cranial cruciate ligament rupture. PLoS
One 2014;9:e106389.
Heffron LE, Campbell JR. Morphology, histology, and
functional anatomy of the canine cranial cruciate
ligament. Vet Rec 1978;102:280–283.
Hong SH, Choi J-Y, Lee GK, et al. Grading of anterior
cruciate ligament injury. J Comput Assist Tomogr
2003;27:814–819.
Hulse D, Beale B, Kerwin S. Second look arthroscopic
findings after tibial plateau leveling osteotomy. Vet
Surg 2010;39:350–354.
Kim SE, Lewis DD, Pozzi A, et al. Radiographic quantitative assessment of cranial tibial subluxation
before and after tibial plateau leveling osteotomy
in dogs. Am J Vet Res 2011;72:420–416.
Provenzano PP, Heisey D, Hayashi K, et al. Subfailure
damage in ligament: a structural and cellular evaluation. J Appl Physiol 2002;92:362–371.
Sample SJ, Racette MA, Hans EC, et al. Radiographic
and magnetic resonance imaging predicts severity
of cruciate ligament fiber damage and synovitis in
dogs with cranial cruciate ligament rupture. PLoS
One 2017;12:e0178086.
Scavelli TD, Schrader SC, Matthiesen DR, Skorup DE.
Partial rupture of the cranial cruciate ligament in
the stifle in dogs (1982–1988). J Am Vet Med Assoc
1990;196:1135–1138.
Tashman S, Anderst W, Kolowich P, et al. Kinematics
of the ACL-deficient canine knee during gait: serial
changes over two years. J Orthop Res 2004;22:931–
941.
VetBooks.ir
VetBooks.ir
17
Caudal Cruciate Ligament
Rupture
Peter Muir
Introduction
Rupture of the caudal cruciate ligament (CaCL)
is less common than rupture of the cranial cruciate ligament (CrCL). Isolated disruption of the
CaCL is found in less than 2% of stifle surgery
patients (Harari 1993). Experimentally, transection of the CaCL does not cause an obvious
lameness, and only leads to mild internal rotation of the tibia relative to the femur (Harari
et al. 1987). Although caudal drawer motion was
detectable during a six-month study period,
minimal degeneration of the articular cartilage
with very little osteophyte formation was found
experimentally (Pournas et al. 1983; Harari et al.
1987). Meniscal damage was not found after
experimental transection of the CaCL (Pournas
et al. 1983; Harari et al. 1987). Therefore, whether
naturally occurring isolated disruption of the
CaCL causes lameness clinically in the dog is
unclear.
Rupture of the CaCL often involves avulsion
fracture of an attachment site. Affected dogs are
usually immature or adolescent patients with
history of trauma and often additional injuries
(Johnson & Olmstead 1987). Complete rupture
of the CaCL is also seen in dogs with stifle luxation, in combination with rupture of the CrCL
and the medial collateral ligament, secondary
to stifle trauma (Hulse & Shires 1986; Aron
1988). Mild damage to the CaCL is underappreciated clinically (Sumner et al. 2010). Superficial fraying, splits in the ligament matrix and
fiber rupture of the CaCL are often found in
dogs with degenerative cruciate ligament rupture (CR) in both partial and complete CR cases.
Some degree of damage to both cruciate ligaments is often found in dogs with a stable stifle during arthroscopic examination of the stifle
(Figures 17.1 and 17.2).
Clinical presentation
Mid-substance tears
Dogs with isolated mid-substance tears usually
have a history and clinical signs that are similar
to dogs affected with the typical CR condition.
A history of trauma may be described by the
owner in some patients. Although stifle instability is often appreciated on physical examination, caudal drawer motion is difficult to recognize specifically (Might et al. 2013), and may be
misinterpreted as cranial drawer motion. Consequently, it is easy to fail to diagnose CaCL
rupture clinically during patient examination.
Radiographic signs are also similar to dogs
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
123
Clinical Features
VetBooks.ir
124
MC
most likely to be made during arthroscopy or
arthrotomy of the stifle (Johnson & Olmstead
1987). In dogs with CaCL rupture, ligament
degeneration and inflammation, and rupture of
CrCL fibers is typically present in many affected
dogs. These dogs are essentially affected with
CR (Sumner et al. 2010). Menisci are typically
intact in dogs with isolated CaCL rupture (Johnson & Olmstead 1987).
Avulsion fracture
Figure 17.1 Arthroscopic image of the intercondylar
notch region of the distal femur of the right stifle of a
7-year-old neutered female mix-breed dog with a stable
stifle and very mild stifle arthritis radiographically. Mild
disruption of some of the fibers of the caudal cruciate
ligament is evident, particularly adjacent to the femoral
attachment site (arrows). MC, medial condyle.
with CR. Caudal displacement of the tibia relative to the femur may be evident on a lateral
radiograph of the stifle (Soderstrom et al. 1998).
Unless magnetic resonance imaging (MRI) of
the stifle is performed, a specific diagnosis is
MC
Dogs with an avulsion fracture of the proximal or distal attachment site of the CaCL
are usually young patients presented with a
clear history of trauma and a persistent lameness (Reinke 1982). Stifle swelling and instability is often detected on physical examination.
Avulsion fracture fragments are usually evident
radiographically, with careful examination of
high-quality radiographs. However, if an avulsion fracture fragment is identified radiographically, it may be difficult to determine which cruciate ligament it is associated with.
Multiple ligamentous injuries to the stifle
In dogs with severe stifle trauma and disruption
to multiple stifle ligaments, the CaCL is ruptured in more than 80% of patients (Aron 1988).
The presence of CaCL rupture is often masked
by stifle instability because of disruption to
other supporting structures, such as the CrCL
and the medial collateral ligament (Hulse &
Shires 1986; Aron 1988).
Treatment
Figure 17.2 Photograph of the intercondylar notch
region of the distal femur of the right stifle of a 1-year-old
neutered male Labrador with an unstable stifle, moderate
arthritis, and rupture of the cranial cruciate ligament.
Complete disruption of the cranial cruciate ligament
(arrowheads), together with partial rupture of the caudal
cruciate ligament, with disruption of ligament fascicles
was found at surgery (arrow). MC, medial condyle.
In dogs with isolated CaCL rupture the need
for surgical treatment is unclear, particularly as
experimental transection of the CaCL does not
lead to lameness. Although various extracapsular and intra-articular stabilization methods
have been proposed, objective long-term evaluation of these procedures is lacking (Harari
1993). If tibial plateau leveling osteotomy
(TPLO) surgery is planned as a treatment for
CR, it is particularly important to determine
whether caudal drawer motion may be present
before surgery, and whether substantial CaCL
VetBooks.ir
Caudal Cruciate Ligament Rupture
damage or rupture is present during surgery,
as this is a contraindication for the TPLO procedure. TPLO increases CaCL loading, and the
joint-stabilizing effect of TPLO depends on
a biomechanically intact CaCL being present
(Warzee et al. 2001; Zachos et al. 2002).
In dogs with avulsion fractures, if the fracture
fragment is sufficiently large, fracture repair
with a lag screw is recommended (Reinke 1982;
Harari 1993). In patients where the fracture fragment is small, debridement of the fragment is
indicated. Again, the need for a stifle stabilization procedure in these patients is unclear
(Harari 1993).
In dogs with multiple ligamentous injury,
surgical treatment for CrCL rupture, medial
collateral ligament rupture, and menisci injury
should be a priority. Menisci and their supporting structures should be preserved where
possible. Collateral ligament rupture should be
repaired with sutures if possible. A number
of procedures are available for stifle stabilization to protect reconstructed ligaments, including extracapsular stabilization and the use of a
transarticular external skeletal fixator.
Conclusions
In conclusion, in dogs affected with CR, fiber
damage in both the CrCL and the CaCL is often
found during arthroscopy or arthrotomy (Sumner et al. 2010). Fraying of the CaCL is underappreciated unless a probe is used specifically
to examine the ligament during surgery. Occasionally, substantial damage to the CaCL will
be identified in dogs diagnosed with CR. This
is important, as substantial disruption of the
CaCL is a contraindication for TPLO.
125
References
Aron DN. Traumatic dislocation of the stifle joint:
Treatment of 12 dogs and one cat. J Am Anim Hosp
1988;24:333–340.
Harari J, Johnson AL, Stein LE, et al. Evaluation of
experimental transection and partial excision of
the caudal cruciate ligament in dogs. Vet Surg
1987;16:151–154.
Harari J. Caudal cruciate ligament injury. Vet Clin
North Am Small Anim Pract 1993;23:821–829.
Hulse DA, Shires P. Multiple ligament injury of the
stifle joint in the dog. J Am Anim Hosp Assoc
1986;22:105–110.
Johnson AL, Olmstead ML. Caudal cruciate ligament
rupture. A retrospective analysis of 14 dogs. Vet
Surg 1987;16:202–206.
Might KR, Bachelez A, Martinez SA, et al. Evaluation
of the drawer test and the tibial compression test
for differentiating cranial and caudal stifle subluxation associated with cruciate ligament instability.
Vet Surg 2013;42:392–397.
Pournas J, Symeonides PP, Karkavelas G. The significance of the posterior cruciate ligament in the stability of the knee. An experimental study in dogs.
J Bone Joint Surg 1983;65B:204–209.
Reinke JD. Cruciate ligament avulsion injury in the
dog. J Am Anim Hosp Assoc 1982;18:257–264.
Soderstrom MJ, Rochat MC, Drost WT. Radiographic
diagnosis: avulasion fracture of the caudal cruciate ligament. Vet Radiol Ultrasound 1998;39:536–
538.
Sumner JP, Markel MD, Muir P. Caudal cruciate ligament damage in dogs with cranial cruciate ligament rupture. Vet Surg 2010;39:936–941.
Warzee CC, Dejardin LM, Arnoczly SP, et al. Effect
of tibial plateau leveling on cranial and caudal tibial thrusts in canine cranial cruciate deficient stifles.
Vet Surg 2001;30:278–286.
Zachos TA, Arnoczky SP, Lavagnino M, et al. The
effect of cranial cruciate ligament insufficiency on
caudal cruciate ligament morphology: An experimental study in dogs. Vet Surg 2002;31:596–
603.
VetBooks.ir
VetBooks.ir
18
Stress Imaging of the Stifle
Stanley E. Kim
Introduction
Plain radiography is an excellent diagnostic tool
for evaluating stifles for cruciate ligament rupture (CR) (Carobbi & Ness 2009). Stress imaging
for dogs with CR is not commonly performed,
as the most clinically significant information is
typically found when high-quality plain radiographs are evaluated, together with accurate
clinical findings such as signalment, history,
and orthopaedic examination. However, stress
imaging of the cranial cruciate ligament (CrCL)deficient stifle still does carry some value in
both clinical and research settings.
The detection of excessive cranial tibial translation is pathognomonic for CrCL insufficiency.
Instability is classically assessed by examination using two physical tests: the cranial drawer
test (Muir 1997); and the tibial compression
test (Henderson & Milton 1978). Unfortunately,
it can be difficult to elicit a positive result
with either of these tests in dogs with CR, as
laxity may be overcome by factors such as poor
execution of the maneuver by the operator,
high muscle tone, and periarticular fibrosis in
the dog (Flo & DeYoung 1978). In some dogs
with partial CR, no palpable laxity is present
because the vast majority of the CrCL remains
intact. Thus, a non-operative diagnosis of CR
often relies on other examination findings such
as periarticular thickening, stifle effusion, and
pain. The simple combination of palpating the
stifle for the presence of effusion and detecting
stifle effusion on radiographs was shown to be
a highly accurate method for diagnosing CR.
Nevertheless, stress radiography has been
advocated to improve diagnostic accuracy by
quantifying cranial tibial translation radiographically. This can be achieved by acquiring
radiographs while performing a modified tibial compression test (de Rooster et al. 1998; de
Rooster & van Bree 1999a–c). Laxity may also
be detected on radiography by using specially
designed devices that attempt to force the stifle
into drawer (Lopez et al. 2004). Standing radiography may be considered as another ‘stressradiographic’ technique, where the intrinsic
forces that are present during standing promote
cranial tibial translation in CrCL-deficient stifles (Kim et al. 2011). Finally, stress magnetic
resonance imaging (MRI) of the stifle has been
described for the purposes of evaluating meniscal integrity in CR stifles.
This chapter will outline each of these stress
imaging techniques and discuss their potential clinical and research utility. It should be
noted that coronal instability (i.e., assessment
of varus/valgus laxity), which typically occurs
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
127
VetBooks.ir
128
Clinical Features
with collateral ligament rupture, is not covered
in this chapter. Stress radiography for assessing
collateral ligament integrity may be indicated in
some cases of CR, where severe trauma results
in multi-ligament injury; a thorough discussion
of these injuries is beyond the scope of this text.
*
Measuring subluxation
For all of the described stress-imaging techniques, the detection of subluxation is made
possible by assessing the cranial-caudal alignment of the tibia relative to the femur on
lateral views of the stifle after applying a
cranial tibial translational load. When palpable
instability caused by CR is present, altered
femorotibial alignment is usually obvious upon
subjective comparisons between stressed and
non-stressed images (Figure 18.1). In one of
the original descriptions for stress radiography,
the stress test was considered positive when a
vertical line running tangential to the femoral
condyles fell behind the caudal aspect of the
tibial plateau (de Rooster et al. 1998). Other
subjective findings considered to be indicative
of subluxation included cranial displacement
of the intercondylar eminence relative to the
lateral femoral condyle (Figure 18.1), and
caudal displacement of the popliteal sesamoid
relative to the tibial plateau.
Because the accuracy of subjective assessments is likely dependent on the expertise of
the observer, numerous methods for the objective quantification of cranial tibial subluxation
have been described. For most methods, the
distance between a specified femoral landmark
and tibial landmark along a defined axis of
translation is calculated (de Rooster et al. 1998;
Plesman et al. 2012). In the first description by
de Rooster and van Bree, cranial-caudal laxity
was best assessed by using the tibial plateau
as the axis of translation, and the caudal margins of the femoral and tibial condyles. The
distance from the caudal margin of the tibial condyles to a line passing tangential to the
femoral condyles and perpendicular to the tibial plateau is measured on stressed and nonstressed radiographs, where the difference in
the distance defines the amount of laxity. Laxity
indices can also be made where the values are
normalized to a particular femoral dimension.
(A)
*
(B)
Figure 18.1 Neutral (A) and compressed (B) lateral
projection radiographs of a stifle with cruciate ligament
rupture. Note the change in position of a vertical line (red
dotted line) tangential to the caudal femoral condyles,
relative to the caudal margin of the tibial plateau. The
direction of change in position is also represented by the
black arrows. Note also the distal position of the popliteal
sesamoid (white arrow). Note the position of the
intercondylar eminence (∗ ), which is adjacent to the
cranial aspect of the femoral condyles on the compressed
view.
In a recent ex vivo study defining landmarks for
measuring cranial tibial subluxation, the tibial
intercondylar eminence and the caudal margin
of the femoral intercondylar notch had the best
repeatability (Plesman et al. 2012).
Any of the described measurements are
affected by radiographic positioning, where
even minor obliquity of the projection will significantly alter the calculated alignment. Thus,
it is imperative that perfect lateral projections of
both the femur and tibia are obtained, regardless of the method used to calculate subluxation. This can be challenging for inexperienced
operators in some cases for several reasons,
VetBooks.ir
Stress Imaging of the Stifle
including the presence of moderate rotational
stifle laxity and limb deformity. Furthermore,
these measurements are sensitive to changes
in stifle flexion angle because the femur ‘rolls’
caudally on the tibial plateau as the stifle flexes.
Flexion angle must, therefore, be kept consistent between stressed and non-stressed views.
Most techniques advocate using a flexion angle
of 90◦ .
In functional in vivo studies where subjects
are imaged during activities (e.g., standing), it
may not be possible to keep the flexion angle
consistent between stressed and non-stressed
views. This renders the techniques for quantifying subluxation described above inaccurate.
An alternate method for quantifying alignment
is available when flexion angle cannot be controlled, which involves simply measuring the
direct distance between the proximal and distal attachment sites of the CrCL (Figure 18.2);
increases in this distance under stress views are
interpreted as being indicative of cranial tibial subluxation. The measurement is also unaffected by any change in tibial geometry due
to tibial plateau leveling osteotomy. However,
there is still a susceptibility to error associated
with oblique projections.
When stressed views are compared to
non-stressed views, it is important to assess
whether there is already cranial tibial subluxation present on the non-stressed image. As
the detection of subluxation is pathognomonic
for CR, performing an additional stress view is
probably unnecessary. Furthermore, the magnitude of calculated subluxation will be lower
if the difference in alignment between the two
views is quantified, and it may thus be possible
to get a false-negative result. One potentially
helpful method of more objectively assessing
for subluxation if cranial tibial subluxation is
suspected in the non-stressed stifle is to compare femorotibial alignment to the contralateral
stifle, provided that the contralateral stifle is
normal.
Tibial compression radiography
With tibial compression radiography, the
stressed views are obtained while performing the tibial compression test. With the dog
in lateral recumbency, a standard lateral
129
Figure 18.2 Lateral projection radiograph showing the
method by which the proximal and distal attachment sites
of cranial cruciate ligament were defined. The proximal
attachment was defined as the point on the cranioproximal margin of the femoral condyles immediately
caudal to the roof of the intercondylar notch, and the
distal attachment site was defined as the point at the
cranial margin of the medial tibial condyle (doubleheaded arrow).
radiographic view of the stifle is obtained with
the stifle at 90◦ of flexion (neutral position).
While maintaining the same stifle flexion angle,
a second radiograph is performed with the
tarsal joint being maximally flexed by hand
(tibial compression position) (Figure 18.3).
Noticeable cranial movement of the tibia relative to the distal femur between stressed and
non-stressed views is considered indicative of
CrCL rupture (see Figure 18.1). In a study using
a subjective method of assessing for subluxation where the positions of the caudal femoral
condyle relative to the tibial plateau were
determined, the test was found to have 97%
sensitivity and 100% specificity for detection of
CR (de Rooster et al. 1998).
Clinical Features
VetBooks.ir
130
(A)
Figure 18.3 Paired lateral
radiographs (neutral and tibial
compression) are obtained using
positioning illustrated by the
drawings. A standard lateral
radiographic view is obtained
with the joint at 90◦ of flexion
(neutral position; A). While
maintaining the angle of flexion,
the tarsal joint is maximally
flexed by use of manual pressure,
and a second radiograph is
obtained (tibial compression
position, B). Source: Reproduced
from de Rooster et al. 1998, with
permission from the British
Veterinary Association.
(B)
Evidence for the ability of tibial compression
radiography to diagnose partial CR is conflicting. It has been suggested that performing the
tibial compression test at 90◦ of flexion will be
able to induce abnormal cranial tibial translation even in those cases with partial CrCL rupture, because the cranio-medial band is typically damaged and the intact caudo-lateral
band is lax in flexion. In a clinical study where
the change in femoro-tibial alignment between
stressed and non-stressed views was quantified,
significant differences in relative femoro-tibial
displacement were found between normal stifles, stifles with partial CR, and stifles with complete CR (de Rooster & van Bree 1999c). In a
more recent investigation, greater cranial tibial
translation was also identified in palpably stable stifles with mild CrCL fiber disruption when
compared to a control group (Zatloukal et al.
2000). However, an upper limit of normal laxity has not yet been defined. Indeed, a surprisingly wide range of laxity has been found for
joints with completely intact CrCLs. Results of
another clinical study corroborate that there is
a ‘gray-zone’ of laxity that includes both normal and diseased stifles. Furthermore, differences in the degree of fiber damage to the CrCL
and medial meniscus cannot be deduced from
the amount of relative displacement (de Rooster
& van Bree 1999c).
The inability to distinguish normal laxity
from subtly abnormal laxity is arguably one
of the major reasons why this test has not
become more widely adopted in the clinical
setting. In stifles with obvious instability, tibial compression radiography is not required as
drawer motion will be detected on examination.
In palpably stable stifles affected by CR, the
presence of stifle effusion on radiographs and
orthopaedic examination are typically accurate
indicators of disease, especially when appropriate efforts to rule out other diseases (e.g.,
immune-mediated arthritis and osteochondritis dissecans) have been performed. Thus,
tibial compression radiography is typically considered as a supplemental diagnostic test, rather
than a necessary one. Another limitation is
radiation exposure of the handler (ionizing
radiation regulations in certain countries may
preclude the use of this test). Modifications of
the technique where devices are used to induce
tibial compression have been suggested, but not
well described or validated.
Stress devices
Several devices for conducting stress radiography have been described. One such device
was developed with the aim of precisely quantifying cranio-caudal tibial translation through
the controlled application of a cranially (or caudally) directed force on the crus, while keeping the thigh region stationary (Lopez et al.
VetBooks.ir
Stress Imaging of the Stifle
2004). The device consisted of a radiolucent
platform where the thigh and crus regions are
constrained by adjustable fiberglass stays and
straps. Cranially or caudally directed forces can
be applied onto the mobile tibial component
of the device. In an experimental study, the
observed laxity on stress radiographs using the
device was significantly different between stifles with intact CrCL, partially ruptured CrCL,
and completely transected CrCL. The main
advantages of the device include the ability to
more precisely control stifle flexion angle, and
consistent delivery of a known force. The device
has been used in several studies to help assess
the performance of novel stabilizing techniques
in experimental dogs. Whereas the type of force
applied by the aforementioned device applies a
cranial drawer force, a more recently described
device aims to induce tibial compression by
positioning the limb onto a radiolucent frame
and a series of adjustable pegs (Bhandal et al.
2008). The use of such a device eliminates the
need for a handler to be exposed to radiation
during tibial compression radiography. Unfortunately, these devices are not widely or commercially available as they lack any obvious
clinical utility.
Standing radiography
Unlike in humans, the forces generated during standing alone are enough to consistently
induce substantial tibial translation in CrCLdeficient dogs (Kim et al. 2011; Kim et al. 2012).
Thus, imaging of the stifle during standing can
be considered as another form of stress imaging. A horizontally aligned radiographic beam
is centered over the stifle using a mobile X-ray
unit, with the cassette placed between the dog’s
pelvic limbs. The dog is gently restrained to
limit motion and promote a comfortable posture as the image is acquired (Figure 18.4).
Horizontal beam radiography has been used
to quantify subluxation during standing before
and after various surgical procedures. The main
advantage of standing radiography is that subluxation is caused by intrinsic forces occurring naturally rather than by an externally
applied force. This means that the abnormal
alignment observed with standing radiography
gives direct insight into the degree of in vivo
131
Figure 18.4 Photograph of the set-up used to acquire a
horizontal beam radiographic view of the stifle. A
horizontally aligned radiographic beam is centered over
the stifle using a mobile X-ray unit, with the cassette or
panel placed between the dog’s pelvic limbs. The dog is
gently restrained to limit motion and promote a
comfortable posture as the image is acquired.
dysfunction. One previous study used standing radiography to show that persistent subluxation occurs in a subset of cases after stabilization with tibial plateau leveling osteotomy
(Kim et al. 2012) and tibial tuberosity advancement (Skinner et al. 2013). The technique is
labor-intensive, and generally requires a handler to restrain the dog where there is radiation exposure. The flexion angle cannot be
controlled. Therefore, alternative measures of
subluxation such as quantifying the distance
between the proximal and distal attachment
sites of the CrCL may be required to compare
cranio-caudal alignment between different time
points or views. This technique may also be
especially prone to errors caused by oblique
projections because the axial rotational position
of the stifle may be variable.
Stress-MRI
Recently, a stress-MRI technique was described
in an ex vivo study where a custom-made
Clinical Features
VetBooks.ir
132
a b
in both the lateral and medial compartments
could be quantified (Figure 18.5) (Tremolada
et al. 2014). The magnitude of cranial tibial translation was shown to be greater in the lateral
compartment. The main goal of the study was
to demonstrate the feasibility of a stress-MRI
technique to potentially improve the ability to
identify meniscal tears using advanced imaging. While stress-MRI of the knee is a useful
clinical test for assessing menisci in humans,
further studies are required to determine if the
technique has a superior diagnostic accuracy
to standard MRI for characterizing meniscal
pathology in dogs.
Conclusions
(A)
a b
In summary, stress imaging techniques aiming to induce cranial tibial subluxation in joints
with suspected CR are well described. They
have potential clinical utility, as the ability to
detect instability with stress radiography is
superior to physical maneuvers such as the
cranial drawer test. Thus, stress imaging may
be particularly valuable for clinicians with less
experience and confidence with stifle palpation
alone. Stress imaging is also a useful tool for
providing an ability to assess stifle stability in
both clinical and experimental studies.
References
(B)
Figure 18.5 Positional changes of lateral (A) and medial
(B) femoral condyles in a cranial cruciate
ligament-deficient stifle using stress-MRI. The
superimposed outlines of the caudal femoral condyle
(solid line = neutral; dotted line = stressed) demonstrate
that stress-MRI is able to induce femorotibial subluxation.
Source: Tremolada et al. 2014. Reproduced with
permission from the American Veterinary Medical
Association.
MRI-compatible jig was used for either the tibial compression test or the cranial drawer test.
Both methods were equally effective in causing cranial tibial subluxation in CrCL-deficient
stifles. With cross-sectional imaging, translation
Bhandal J, Kuzma A, Schiller T, et al. Application
of a tibial compression device to diagnose partial or complete rupture of the cranial cruciate
ligament in 129 dogs. Proceedings of the Veterinary Orthopaedic Society Annual Meeting, 2008,
p. 65.
Carobbi B, Ness MG. Preliminary study evaluating
tests used to diagnose canine cruciate ligament failure. J Small Anim Pract 2009;50:224–226.
de Rooster H, van Bree H. Use of compression stress
radiography for the detection of partial tears of
the canine cranial cruciate ligament. J Small Anim
Pract 1999a;40:573–576.
de Rooster H, van Bree H. Popliteal sesamoid displacement associated with cruciate rupture in the
dog. J Small Anim Pract 1999b;40:316–318.
de Rooster H, van Bree H. Radiographic measurement of craniocaudal instability in stifle joints of
clinically normal dogs and dogs with injury of a
cranial cruciate ligament. Am J Vet Res 1999c;60:
1567–1570.
VetBooks.ir
Stress Imaging of the Stifle
de Rooster H, Van Ryssen B, van Bree H. Diagnosis
of cranial cruciate ligament injuries in dogs by tibial compression radiography. Vet Rec 1998;142:366–
368.
Flo GL, DeYoung D. Meniscal injuries and medial
meniscectomy in the canine stifle. J Am Anim Hosp
Assoc 1978;14:683–689.
Henderson RA, Milton JL. The tibial compression
mechanism: a diagnostic aid in stifle injuries. J Am
Anim Hosp Assoc 1978;14:474–479.
Kim SE, Lewis DD, Pozzi A, et al. Radiographic quantitative assessment of cranial tibial subluxation
before and after tibial plateau leveling osteotomy
in dogs. Am J Vet Res 2011;72:410–416.
Kim SE, Lewis DD, Pozzi A. Effect of tibial plateau
leveling osteotomy on femorotibial subluxation: in
vivo analysis during standing. Vet Surg 2012;41:
465–470.
Lopez MJ, Hagquist W, Jeffrey SL, et al. Instrumented measurement of in vivo anterior-posterior
translation in the canine knee to assess anterior
133
cruciate integrity. J Orthop Res 2004;22:949–
954.
Muir P. Physical examination of lame dogs. Compend
Cont Ed Pract Vet 1997;19:1149–1161.
Plesman R, Sharma A, Gilbert P, et al. Radiographic
landmarks for measurement of cranial tibial subluxation in the canine cruciate ligament deficient
stifle. Vet Comp Orthop Traumatol 2012;25:478–
487.
Skinner OT, Kim SE, Lewis DD, et al. In vivo
femorotibial subluxation during weight-bearing
and clinical outcome following tibial tuberosity
advancement for cranial cruciate ligament insufficiency in dogs. Vet J 2013;196:86–91.
Tremolada G, Winter MD, Kim SE, et al. Validation of
stress magnetic resonance imaging of the canine stifle joint with and without an intact cranial cruciate
ligament. Am J Vet Res 2014;75:41–47.
Zatloukal J, Necas A, Dvorak M. Measuring craniocaudal instability in stifle joints of dogs using stress
radiographs. Acta Vet Brno 2000;69:311–317.
VetBooks.ir
VetBooks.ir
19
Stifle Ultrasonography
Cristi R. Cook
The normal stifle joint
Canine stifle joint disorders have been frequently diagnosed based on physical examination findings, radiographs, and arthrography
(Reed et al. 1995; Kramer et al. 1999; Soler et al.
2007). More recently, ultrasonography, computed tomography and magnetic resonance
imaging have been used to further evaluate
the stifle joint (Gnudi & Bertoni 2001; Samii &
Long 2002; Soler et al. 2007). Musculoskeletal
ultrasound is commonly performed in humans.
Canine stifle ultrasound has become a more
common diagnostic modality to evaluate the
intra-articular structures of the stifle joint over
the last decade (Kramer et al. 1999; Gnudi &
Bertoni 2001; Samii & Long 2002; Soler et al.
2007; Arnault et al. 2009; Mattoon & Nyland
2015; Cook 2016). Notably, it is useful in evaluating the intra-articular soft tissues and the
supporting extra-articular structures.
Stifle ultrasound examination is best performed using a 10–18 MHz high-resolution,
linear transducer (Kramer et al. 1999). To minimize any artifacts, the hair along the stifle joint
should be clipped and ultrasound coupling
gel applied to the skin surface. The linear
transducer is most appropriate for imaging
superficial structures with high detail while
minimizing the artifacts from anisotropy; the
latter occurs when the fibers of the tendon or
ligament are not perpendicular to the ultrasound beam (Figure 19.1A,B). Off-angle artifact,
or anisotropy, appears as a hypoechoic area
within the tendon or ligament, but when the
same structure is oriented perpendicular to the
ultrasound beam the fibers will reappear (Reed
et al. 1995; Kramer et al. 1999). It is important to
look at potential lesions in both the longitudinal
and transverse planes to confirm the lesion is
real or artifact, while making sure the transducer face is perpendicular to the structure of
interest (Reef et al. 1998; O’Connor & Grainger
2005).
The cranial joint space is imaged with the
transducer interface along the patellar tendon.
The patellar tendon is seen in both transverse
and sagittal planes as a superficial structure
with low to moderate echogenicity and linear hyperechoic interstitial fibers (Reed et al.
1995; Kramer et al. 1999; Soler et al. 2007).
In the transverse imaging plane, the patellar
tendon is ovoid with hyperechoic, pinpoint
foci representing the interstitial fibers. The
peritendinous tissue should be a thin, hyperechoic line (Kramer et al. 1999; Soler et al. 2007)
(Figure 19.2). Deep to the patellar tendon is the
infra-patellar fat pad, which is hypoechoic to
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
135
Clinical Features
VetBooks.ir
136
(A)
(B)
Figure 19.1 Normal tendon anisotropy. (A) The tendon
fibers ‘drop out’ when the ultrasound beam is not parallel
to the tendon fibers. (B) The tendon fibers reappear when
the beam is parallel.
FP
F
T
Figure 19.2 Normal cranial joint space of the stifle. The
synovium is the very thin, hyperechoic line just cranial to
the tibial cortex. F, femur; T, tibia; FP, fat pad.
the patellar tendon and has a coarser echotexture in comparison to the tendon (Reed et al.
1995; Kramer et al. 1999; Soler et al. 2007). The
collateral ligaments are similar in appearance,
although smaller, to the patellar tendon in
their echogenicity and echotexture; this is in
contradiction to other reports which state they
are not visible, and is likely due to the advancements in technology and increasing resolution
capabilities (Kramer et al. 1999; Samii & Long
2002; Soler et al. 2007). The medial collateral
ligament is seen along the medial joint surface,
at the most distal curve of the femoral condyle.
The lateral collateral ligament can be identified
along the lateral joint, caudal to the long digital
extensor tendon (LDE) with the tibial attachment angling caudodistally toward the fibular
head (Vasseur & Arnoczky 1981). The LDE tendon is seen along the craniolateral joint space
superficial to the lateral meniscus and cranial to
the lateral collateral ligament. The thickness of
the LDE tendon will increase as the transducer
is moved distally, toward the musculotendinous junction (Reed 1995). The stifle ligaments, in general, should maintain a constant
width.
The femoral condyles and tibial plateau are
defined as hyperechoic lines with clean distal
acoustic shadowing. The cartilage is a very thin,
hypoechoic line, superficial to the hyperechoic
cortical bone. Deep intra-articular structures are
the most difficult ligaments of the stifle joint to
examine. The cranial cruciate ligament (CrCL)
at its tibial attachment is best imaged from the
cranial skin surface in the sagittal plane with
the joint positioned in full flexion. In large dogs,
the CrCL can be seen in full extension, but in
small dogs the intercondylar space is too narrow, hindering visibility (Kramer et al. 1999).
The CrCL appears as a hypoechoic structure
compared to the patellar tendon. It is lined by
the echogenic fat of the infra-patellar fat pad
and synovium, which is a discrete, thin, hyperechoic line deep to the infra-patellar fat pad.
The CrCL becomes hyperechoic when the transducer is perpendicular to the ligament fibers
(Gnudi & Bertoni 2001; Seong et al. 2005) (Figure 19.3). In one study, the hyperechoic fibers
became hypoechoic when the transducer was
angled 3◦ off from the proper perpendicular
orientation (i.e., drop-out or off-angle artifact)
(Reed et al. 1995; O’Connor & Graninger 2005).
137
VetBooks.ir
Stifle Ultrasonography
Figure 19.3 Zoomed image of the normal cranial
cruciate ligament in the full flexion technique with
proximolateral-distomedial rotation of the transducer. The
normal longitudinal fiber pattern is identified (arrows). F,
femur; T, tibia.
Improved viewing of the CrCL in the longitudinal axis has been shown with maximum
flexion of the stifle and rotation of the ultrasound probe in a proximolateral to distomedial
direction (Nayseh et al. 2015) (Figure 19.4). This
allows more of the ligament to be imaged and
allows an improved alignment (anisotropy) of
the ligament fibers. This would also improve
the likelihood of identifying subtler interstitial
tears of the ligament. The caudal cruciate ligament (CaCL) is not easily visible with any cranial imaging technique due to the large muscle mass along the caudal joint (Kramer et al.
1999). The femoral attachment of the CaCL has
been imaged in multiple studies with the use of
Figure 19.5 Normal meniscus. Note the abaxial surface
of the meniscus positioned along the femoral and tibial
cortical margins (arrows). The asterisks outline the normal
medial meniscus. F, femur; T, tibia.
a water bath, with the stifle in extension or full
flexion (Reed et al. 1995; Gnudi & Bertoni 2001;
Samii & Long 2002; Seong et al. 2005).
The medial and lateral menisci are best seen
on sagittal plane images. Each appears as a triangular, echogenic structure that is fairly homogeneous (Reed et al. 1995; Kramer et al. 1999;
Soler et al. 2007). The apex of the triangle points
axially, conforming to the femoral condyle and
tibial plateau (Figure 19.5). The cranial, central, and caudal regions of the medial meniscus are visible, whereas the different sections of
the lateral meniscus are more difficult to identify routinely and are dependent on the individual patient. The different sections of the menisci
are based on their location to the collateral ligaments (i.e., the cranial horn of the meniscus is
found cranial to the collateral ligament; the caudal horn, caudal to the ligament and the central region, adjacent to the collateral ligament).
Normally, there is a thin fluid line between the
meniscal and osseous surfaces.
The abnormal stifle joint
Figure 19.4 Normal image of the cranial cruciate
ligament (arrows) attachment along the tibial cortex
(arrowheads).
The most common abnormality of the stifle joint
is cruciate ligament rupture (CR). In acute cases,
the joint effusion can be mild to severe and
potentially have echogenic fluid if there is a significant hemarthrosis with imaging in the early
phase of the rupture. The rupture of the ligament may be identified if it is near the tibial attachment, and may not be visible if it is
Clinical Features
VetBooks.ir
138
F
(A)
T
(B)
Figure 19.6 (A) Hyperechoic, irregular tissue between the arrowheads is associated with synovial thickening. (B)
Irregular cortex of the tibia consistent with osteophyte formation (arrows). F, femur; T, tibia.
closer to the midsection or femoral attachment.
In chronic CR cases, the ultrasonographic features seen are synovial hypertrophy, minimal
effusion, unless complicated by a meniscal tear,
and an irregular bone surface due to osteophyte
formation (Figure 19.6A,B). In chronic cases, an
irregular and thickened CrCL may be seen with
retraction of the ends at the site of the tear
(Figure 19.7). Occasionally, interstitial tears of
the CrCL (i.e., intact epiligament with internal
fibers disrupted) can be identified (Figure 19.8).
Meniscal tears are a common primary injury
in the human knee, but rarely occur as a primary
Figure 19.7 Irregular cranial cruciate ligament with
irregular ends (arrow) consistent with a complete rupture.
T, tibia.
stifle injury in dogs and are usually secondary
to CR. The occurrence of secondary meniscal
tears varies between studies, ranging from 10%
to 77% (Mahn et al. 2005; Thieman et al. 2006;
Hayes et al. 2010). The risk of medial meniscal tears increases 12.9-fold with complete CR
(Hayes et al. 2010). There is an approximately
6% tear rate after surgical stabilization of the stifle (Thieman et al. 2006)
The ultrasonographic findings associated
with meniscal tears have been previously
reported as: (i) abnormal shape of the meniscus; (ii) increased fluid adjacent to the meniscus;
(iii) change in the echogenicity of the meniscus;
and (iv) displacement of the meniscus. The
most common abnormal appearance for a
meniscal tear is the flattening of the tibial side
Figure 19.8 Thickened and irregular cranial cruciate
ligament (arrowheads) with synovial hypertrophy and
fluid accumulation along the femoral trochlear notch
consistent with partial cruciate ligament rupture and
retraction of the ruptured fibers. F, femur; T, tibia.
139
VetBooks.ir
Stifle Ultrasonography
Figure 19.11 Bucket-handle tear of the medial
meniscus. Note the abaxial displacement of the abaxial
margin of the medial meniscus (arrows). F, femur; T, tibia.
Figure 19.9 Meniscal tear. There is flattening of the
tibial side of the meniscus with adjacent fluid (arrow).
of the meniscus (Figure 19.9) (Mahn et al. 2005).
Occasionally, axial splitting of the meniscus is
identified in some patients with radial tears.
Small radial tears or fraying of the meniscal
edges may be too small to see specific changes
with ultrasound, but other characteristics of
meniscal tears are usually present. The complex
meniscal tears and the macerated meniscus are
usually seen as an irregular, hyperechoic mass
of tissue with no specific shape (Figure 19.10).
Fluid accumulation is often seen adjacent to
the meniscal tear, and may be the only visible
fluid within the joint. The normal meniscal
echogenicity is relatively hyperechoic to the
surrounding muscles with a fine echotexture.
Figure 19.10 Macerated meniscus. The meniscal tissue
has a mottled appearance with an abnormal shape
(arrowhead). F, femur; T, tibia.
In the presence of a meniscal tear, the meniscus
may appear hypoechoic or mottled (Kramer
et al. 1999). Occasionally, there may be a hyperechoic appearance adjacent to the tibial side
of the meniscus. This has been confirmed
with arthroscopy as hypertrophied synovium
along the meniscus. Meniscal displacement
may be the most difficult feature to evaluate.
There is a faint, hyperechoic line between
the medial meniscus and the joint capsule
that is used as a reference for the meniscal
position. Normally, this line is adjacent to the
surface of the femoral and tibial cortices (see
Figure 19.5) (Mahn et al. 2005). Caution should
be used if there are large osteophytes adjacent
to the joint, as the meniscus can appear falsely
displaced (abaxially). With further evaluation,
the osteophytes are the cause of the apparent
displacement. Abaxial displacement has been
associated with a displaced bucket-handle
tear, following confirmation with arthroscopic
evaluation (Figure 19.11).
Patellar tendon abnormalities are most commonly associated with rupture (incomplete or
complete) or tendonitis associated with a previous surgical treatment. In acute patellar tendon
injuries, it will appear hypoechoic and thickened when compared to normal (Kramer et al.
1999). The fibers may be visible, but not parallel;
disrupted with a distinct peritenon; disrupted
fibers and peritenon; or complete rupture of the
tendon and peritendon (Figure 19.12). Chronic
patellar tendon injuries appear hyperechoic,
focally narrowed, with or without dystrophic
mineralization within the tendon or enthesophytes at the tibial crest.
Clinical Features
VetBooks.ir
140
Figure 19.12 Thickening of the distal patellar tendon
with irregular margins to the tendon (arrow) and an
interstitial tear (arrowhead) consistent with partial
rupture, secondary to a K-wire inserted through the distal
tendon during a surgical repair.
Conclusions
Ultrasound in general is cost-effective and
readily available. However, interest and training in musculoskeletal ultrasound is much
less common. An experienced musculoskeletal
ultrasonographer is important to thoroughly
evaluate the joint and make a knowledgeable
interpretation and diagnosis that corresponds
to the clinical history and examination. A thorough knowledge of the anatomy of the joint or
structures is important, as well as the normal
and abnormal ultrasonographic appearance of
these structure. When learning the ultrasonographic appearance of a new musculoskeletal
area, one is encouraged to evaluate the contralateral limb or image a normal patient for
comparison.
References
Arnault F, Cauvin E, Viguier E, et al. Diagnostic value
of ultrasonography to assess stifle lesions in dogs
after cranial cruciate ligament rupture: 13 cases. Vet
Comp Orthop Traumatol 2009;22:479–485.
Cook CR. Ultrasound imaging of the musculoskeletal system. Vet Clin North Am Small Anim Pract
2016;46:355–371.
Gnudi G, Bertoni G. Echography examination of the
stifle joint affected by cranial cruciate ligament rupture in the dog. Vet Radiol Ultrasound 2001;42:266–
270.
Hayes GM, Langley-Hobbs SJ, Jeffery ND. Risk factors for medial meniscal injury in association with
cranial cruciate ligament rupture. J Small Anim
Pract 2010;51:630–634.
Kramer M, Stengel H, Gerwing M, et al. Sonography of the canine stifle. Vet Radiol Ultrasound
1999;40:282–293.
Mahn MM, Cook JL, Cook CR, et al. Arthroscopic verification of ultrasonographic diagnosis of meniscal
pathology in dogs. Vet Surg 2005;34:318–323.
Mattoon JS, Nyland TG. Fundamentals of diagnostic
ultrasound. In: Small Animal Diagnostic Ultrasound,
Mattoon JS, Nyland TG, eds. Third edition. St Louis
MO, Elsevier. 2015, pp. 1–49.
Nayseh N, Kramer M, Ondreka N. Ultrasonographic
examination of the stifle joint in the dog. Part 1:
Ultrasonographic anatomy, standardized scanning
protocol and common indications. Tierärztl Prax
2015;43:120–129.
O’Connor PJ, Grainger AJ. Ultrasound imaging of
joint disease. In: Practical Musculoskeletal Ultrasound, McNally EG, ed. First edition. Philadelphia
PA, Elsevier. 2005, pp. 245–262.
Reed AL, Payne JT, Constantinescu GM. Ultrasonography anatomy of the normal canine stifle. Vet
Radiol Ultrasound 1995;36:315–321.
Reef VB, Sertich PL, Turner RM. Musculoskeletal
ultrasonography. In: Equine Diagnostic Ultrasound,
Reef VB, Sertich PL, Turner RM, eds. Philadelphia
PA, WB Saunders. 1998, pp. 39–186.
Samii VF, Long CD. Musculoskeletal system. In: Small
Animal Diagnostic Ultrasound, Nyland TG, Mattoon
JS eds. Second edition. Philadelphia PA, WB Saunders, 2002, pp. 267–284.
Seong Y, Eom K, Lee H, et al. Ultrasonographic
evaluation of cranial cruciate ligament rupture via
dynamic intra-articular saline injection. Vet Radiol
Ultrasound 2005;46:80–82.
Soler M, Murciano J, Latorre R, et al. Ultrasonographic, computed tomographic and magnetic resonance imaging anatomy of the normal canine stifle joint. Vet J 2007;174:351–361.
Thieman KM, Tomlinson JL, Fox DB, et al. Effect of
meniscal release on rate of subsequent meniscal
tears and owner-assessed outcome in dogs with
cruciate disease treated with tibial plateau leveling
osteotomy. Vet Surg 2006;35:705–710.
Vasseur PB, Arnoczky SP. Collateral ligaments of the
canine stifle joint: anatomic and functional analysis. Am J Vet Res 1981;42:1133–1137.
VetBooks.ir
20
Computed Tomography (CT)
of the Stifle
Ingrid Gielen and Henri van Bree
Introduction
In dogs, the stifle is a frequently injured joint.
Ligamentous and meniscal damage are common and are associated with secondary degenerative changes (Vasseur 1993; Johnson et al.
1994). The diagnosis of stifle joint disorders is
generally based on a history of lameness, physical examination, and radiography. For decades,
radiography has been the most often-used
medical imaging technique to diagnose stifle
disorders and has been proven very useful in
its clinical work-up (Marino & Loughin 2010).
A stress radiographic technique, based on the
clinical tibial compression test, has been introduced in an attempt to improve the diagnostic
accuracy of clinical evaluation of craniocaudal
instability. It is a valuable asset in the diagnosis of canine stifle instability due to cruciate
ligament rupture (CR). It is a useful technique
to prove (or disprove) a tentative diagnosis of
CR, especially when there is a lack of cranial
drawer sign on clinical examination, and is able
to detect complete or partial CR (de Rooster et al.
1998; de Rooster & van Bree 1999). In contrast to
radiography, where there is summation of the
overlying structures, cross-sectional imaging
such as computed tomography (CT) allows
examination of the internal joint structures
without superimposition. CT has proven to be
extremely sensitive in demonstrating calcified
or bony structures, and also allows demonstration of the soft tissues when the correct
windowing has been applied (Soler et al. 2007).
Indications for using CT
These include:
r
r
r
r
r
r
Developmental disorders: Osteochondrosis
(OC)/osteochondritis dissecans (OCD),
medial or lateral patellar subluxation or
luxation.
Traumatic: fractures of the tibial plateau,
femoral condylar fracture, fracture of the
patella, muscular hematoma, collateral ligament lesion, patellar tendon lesion, gastrocnemius avulsion, avulsion fractures of intraarticular ligaments including the CrCL and
the caudal cruciate ligament (CaCL), the
popliteus, the extensor digitorum longus.
Degenerative: CR, osteoarthritis, enthesiopathies.
Neoplastic: including synovial cell sarcoma,
osteosarcoma, lipoma.
Infection.
Miscellaneous: including subchondral bone
cysts.
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
141
Clinical Features
VetBooks.ir
142
Figure 20.1 Positioning of a dog for stifle CT scanning:
ventral recumbency with both stifles extended and
scanned simultaneously.
Technical aspects
Positioning
Under general anesthesia, the dogs are scanned
in ventral recumbency with both stifles
extended and scanned simultaneously. Care
should be taken to position them symmetrically
(Figure 20.1).
Figure 20.2 Scout view of a stifle CT scan: transversal
scans are made parallel to the joint space. The slice
thickness varies between 1 mm in the joint space and
2 mm at the level of the distal femur and proximal tibia.
Sagittal and dorsal reconstructions are made
afterwards. The images are displayed by adjusting window width (WW) and window level
(WL) and read in both a bone window (WW
3500; WL 500) and a soft-tissue window (WW
400; WL 65).
Technical parameters
The use of contrast medium
With single-slice CT, the X-ray beam is angled
parallel to the surface of the tibial plateau; the
scan range should cover the whole joint, from
the proximal pouches from the distal third of the
femur to the proximal fifth of the length of the
tibia (Figure 20.2).
Multi-slice CT with isotropic resolution
allows scanning of the stifle without tilting
the gantry; angulation and orientation are
performed during post-processing procedures.
In multi-slice CT the slice thickness should
be as thin as possible, 1.25 mm or thinner,
with a slice increment of 50%. In single-slice
devices the suspected pathology dictates the
thickness, which can vary between 2 and 3 mm.
Settings should be 100–120 kV and 100–200 mA,
depending on the animal’s weight and size.
Intravenous (IV) administration of 2 ml of
iodine contrast (400 mg iodine ml–1 ) medium
per kilogram body weight should be used for
any stifle problem involving soft tissues; images
with contrast enhancement provide most information regarding the pathology.
Intra-articular (IA) administration of a
diluted non-ionic, low-osmolar-type contrast
medium, such as iohexol, has been reported
to help with distinguishing the cruciate ligaments, evaluating the menisci and the surface
of the cartilage (Sungyoung Han et al. 2008)
(Figure 20.3A,B). The use of computed tomographic arthrography (CTA) has been described
(Samii 2004), and although the results for CTA
in identifying simulated meniscal injury are
143
VetBooks.ir
Computed Tomography (CT) of the Stifle
(A)
Figure 20.4 Sagittal reconstruction of a CT arthrogram
of a dog after partial medial meniscectomy. The cranial
pole is seen to be missing (black arrow), and the caudal
pole seems to be crushed (white arrows).
(B)
Figure 20.3 (A) Sagittal reconstruction of a CT
arthrogram of the stifle of a 4-month-old mongrel dog.
The articular cartilage can be seen as a radiolucent line
parallel to the subchondral bone (black arrows). The
silhouette of the lateral meniscus can be appreciated as
well (arrowheads). (B) Transverse CT arthrogram image
where the silhouettes of the cranial and caudal cruciate
ligaments can be appreciated. LFC, lateral femoral
condyle; a, caudal cruciate ligament; b, cranial cruciate
ligament; c, menisco-femoral ligament.
encouraging (Tivers et al. 2008), some clinical
studies performed in dogs have reported CTA
in the detection of naturally occurring meniscal
damage to be of limited value (Samii et al.
2009). Although gross meniscal lesions (Figures
20.4 and 20.5B) and cruciate ligament damage
(Figure 20.5A) can be evaluated, the main problem with CTA is that in inflamed stifle joints
the injected contrast medium is very rapidly
absorbed and diluted, making accurate interpretation of possible lesions difficult. Mixing
0.2 mg epinephrine with conventional contrast
agents in order to slow down any resorption
should be used (De Rycke et al. 2015). For CTA,
the normal iodine concentration should be
reduced to 80–100 mg ml–1 to reduce the risk
of contrast obscuring intra-articular structures.
The original contrast medium can be diluted
with saline, and for an average stifle joint a
volume of 4 ml is recommended. Care should
be taken to avoid the fat pad during the intraarticular injection of contrast. Repeated gentle
flexion and extension of the joint should be
performed to enhance contrast dispersion.
CT features of different stifle
conditions
Developmental disorders
OC/OCD: OCD lesions have typical features,
being radiolucencies surrounded by a sclerotic
rim (Olstad et al. 2014). More lesions can be
detected by using CT, and more intra-articular
fragments can also be seen (Figure 20.6). The
status of the joint cartilage can be checked using
CTA (Figure 20.7).
In patella luxation the location of the patella
can be checked, the depth of the patellar
Clinical Features
VetBooks.ir
144
(A)
(B)
Figure 20.5 Dorsal reconstructions of a CT arthrogram of a stifle (flexed 90◦ ) with a ruptured cranial cruciate ligament
(A) and associated medial meniscal damage. In the region of the cranial cruciate ligament a small accumulation of
contrast medium can be seen (white arrow) filling the empty space where normally the ligament is present. (B) The
damaged meniscus is visible as a small filling defect within the joint space outlined by contrast medium (white arrow).
(A)
(B)
Figure 20.6 (A) Radiograph and
corresponding CT image of the
distal femur showing an obvious
OCD lesion in the lateral femoral
condyle not visible on the
radiograph. A small fragment can
also be seen (white arrow). (B) The
corresponding arthroscopic
pictures of the OCD lesion and the
floating fragment.
VetBooks.ir
Computed Tomography (CT) of the Stifle
Figure 20.7 CT arthrogram of a 4-month-old dog
with an osteochondrosis lesion in the area of the
lateral femoral condyle. The contrast medium is
outlining the thickened articular cartilage but no flap
can be demonstrated (black and white arrowheads).
(A)
Figure 20.8 (A) Transverse CT images
of the left and right stifle of a
13-month-old Chesapeake Bay
Retriever with bilateral lateral patellar
luxation. The trochlear groove of the
femur is shallow and shows bony
reaction in the area of the left lateral
femoral condyle (white arrow).
(B) Three-dimensional reconstruction of
a lateral patella luxation in a
5-month-old Flat-Coated Retriever,
showing the lateralized position of the
patella and the tibial tuberosity (∗ ).
(B)
145
Clinical Features
VetBooks.ir
146
Figure 20.9 Transverse image of a fracture of the
distal femur showing displacement of one of the
fragments, but no involvement of the trochlear groove.
groove can be evaluated, and by using threedimensional images the rotation (curvature)
of the long bones can be appreciated (Figure 20.8A,B).
Traumatic lesions
In case of fractures, the number and size, the orientation, and possible involvement of the articular surface can be evaluated (Figure 20.9).
With avulsion fractures, the origin of the
involved tendons can be determined, which
is not always possible on radiographs. CT is
very useful for detection of avulsion fractures
of the CrCL (Figure 20.10), the CaCL (Figure 20.11), the attachment of the m. extensor
digitorum longus (Figure 20.12) (Fitch et al.
1997) and the m. popliteus (Figure 20.13).
By using CTA, the status of these fragments
can be evaluated for surgical decision-making
(Figure 20.14).
Degenerative changes
By using CT, degenerative changes can be
detected at an earlier stage than with radiography (Figure 20.15).
Neoplastic disorders
The extension of neoplastic processes can be
better evaluated with CT than with radiography
(Figure 20.16) (synovial cell sarcoma, primary
bone tumor, lipoma). By using intravenous contrast, the soft-tissue component can be better
evaluated. Biopsies can be performed under CT
guidance (Figure 20.17).
Infection
In case of infection, the extension of the process
can be better evaluated than with radiographs
(Figure 20.18).
Miscellaneous
In case of subchondral bone cysts, the communication of the cyst with the joint cavity can be
checked using CTA (Figure 20.19).
Conclusions
CT is useful in every case where the superimposition of bony structures needs to be avoided
VetBooks.ir
Computed Tomography (CT) of the Stifle
147
(A)
(B)
Figure 20.10 (A) Radiographs of a 5-month-old Golden Retriever with an avulsion of the attachment of the cranial
cruciate ligament. On the caudo-cranial view subchondral sclerosis in the area of the medial part of the lateral femoral
condyle can be appreciated (black arrowheads). (B) Corresponding transversal CT image, and sagittal and dorsal
reconstructed images showing clearly the avulsed proximal attachment of the cranial cruciate ligament at the medial part
of the lateral condyle with associated subchondral sclerosis (black arrowheads).
(Vande Berg et al. 2002). CT is useful in detecting avulsions of the different intra-articular
structures including the CrCL, the CaCL, the
m. extensor digitorum longus, and the m.
popliteus. The detection of a bony avulsion
fragment is superior with CT, compared with
other types of imaging. CTA helps in evaluating the status of these fragments. Plain
CT images are not very useful in evaluating
the integrity of the cruciate ligaments and
VetBooks.ir
148
Clinical Features
(A)
(B)
Figure 20.11 (A) Radiographs of a 6-month-old American Staffordshire Bull Terrier with an avulsion of the attachment
of the caudal cruciate ligament. On the medio-lateral and caudo-cranial views, a fragment is visible (white arrows). On
the caudo-cranial view an associated radiolucency in the medial area of the distal medial femoral condyle can also be
appreciated. (B) Corresponding transverse, and sagittal and dorsal reconstructed CT images showing multiple fragments
(white arrows) in the area of the proximal attachment of the caudal cruciate ligament in the medial area of the medial
condyle. A prominent distension of the joint capsule is present (white arrowhead).
149
VetBooks.ir
Computed Tomography (CT) of the Stifle
(A)
(B)
Figure 20.12 (A) Radiographs of a 14-month-old Great Dane with an avulsion of the origin of the long digital extensor.
On the medio-lateral and caudo-cranial views a radiodense shadow (white arrows) can be identified in the lateral aspect
of the stifle, the origin of which is unclear. (B) Corresponding transverse, and sagittal and dorsal reconstructed CT images
showing this opacity originating from the tendon of origin of the long digital extensor (white arrow).
the menisci, but the use of CTA, if performed
correctly, can help in decision-making. In some
patients with stifle problems, a fragment or
calcified structure can be detected on radiographs. CT helps to clarify the origin of such
fragments, and is very useful for diagnosing
avulsions of the CrCL in young dogs. Avulsion of the CrCL is rare and is thought to be
a disease primarily of skeletally immature
dogs. In these animals, ligamentous attachment to bone is stronger than the immature
bone itself, allowing avulsion to occur under
a force that is insufficient to cause actual
rupture of the ligament. This diagnosis is
clinically important as the avulsed fragment
may be re-attached if large enough, and
consequently the CrCL can be saved in these
young dogs.
Clinical Features
VetBooks.ir
150
(A)
(B)
Figure 20.13 (A) Radiographs of an 8-month-old Rottweiler with an avulsion of the popliteus tendon. On the
caudo-cranial view, a rounded opacity (white arrow) can be identified in the lateral part of the stifle. Its origin is unclear
from these radiographs. (B) Corresponding transverse and dorsal reconstructed CT images showing this opacity
originating from the tendon of origin of the popliteus muscle (white arrows).
Figure 20.14 Transverse image of a CT arthrogram
through the area of the avulsed attachment of the
cranial cruciate ligament. The contrast study shows
that the avulsion is not surrounded by contrast
medium, meaning that there is still some fibrous
attachment present and that the fragment is not
completely detached (arrows). The silhouette of the
involved cranial cruciate ligament can also be
appreciated.
VetBooks.ir
Computed Tomography (CT) of the Stifle
Figure 20.15 Radiograph and
corresponding CT image of the distal
part of the femur showing new bone
formation and subchondral sclerosis in
the area of the medial fabella (white
arrows). These lesions are hardly
visible on the radiograph.
(A)
Figure 20.16 (A) Radiographs of a
6-year-old Bernese Mountain Dog with
a synovial cell sarcoma. The
radiographs show several
radiolucencies in the subchondral
bone (arrows). (B) Transverse images of
the distal femur and proximal tibia
clearly demonstrating the osteolysis
caused by the tumor (arrows). One
transverse image in a soft-tissue
window after intravenous contrast
administration shows enhancement of
the severely swollen synovia (black
arrowheads). These CT images better
show the extent and severity of the
neoplastic process. (C) Sagittal and
dorsal reconstructed images giving a
clear overview of the extent of the
tumor.
(B)
151
Clinical Features
VetBooks.ir
152
(C)
Figure 20.16
(A)
(Continued)
(B)
Figure 20.17 (A) Transverse image of a primary bone tumor in the area of the proximal tibia. (B) CT guidance can be
used to obtain a bone biopsy. The silhouette of the Jamshidi needle is clearly visible.
153
VetBooks.ir
Computed Tomography (CT) of the Stifle
(A)
(B)
Figure 20.18 Transverse images in soft-tissue window of the distal femur (A) and proximal tibia (B) of an infected stifle
joint. The application of intravenous contrast delineates the capsule of different abscesses containing pus (white arrows).
(B)
(A)
(C)
Figure 20.19 (A) Transverse and (B) dorsal reconstruction of a bone cyst in the distal lateral femoral condyle. (C) A CT
arthrogram demonstrates that there is no communication between the cyst and the joint space.
VetBooks.ir
154
Clinical Features
References
De Rycke L, van Bree H, Van Caelenberg A, et al.
Epinephrine-enhanced computed tomographic
arthrography of the canine shoulder. Res Vet Sci
2015;102:15–21.
de Rooster H, Van Ryssen B, van Bree H. Diagnosis
of cranial cruciate ligament injuries in dogs by tibial compression radiography. Vet Rec 1998;142:366–
368.
de Rooster H, van Bree H. Use of compression stress
radiography for the detection of partial tears of
the canine cranial cruciate ligament. J Small Anim
Pract 1999:40;573–576.
Fitch RB, Wilson ER, Hathcock JT, et al. Radiographic,
computed tomographic and magnetic resonance
imaging evaluation of a chronic long digital extensor tendon avulsion in a dog. Vet Radiol Ultrasound 1997;38:177–181.
Johnson JA, Austin C, Breur GJ. Incidence of canine
appendicular musculoskeletal disorders in 16 veterinary teaching hospitals from 1980 through 1989.
Vet Comp Orthop Traumatol 1994;7:56–69.
Marino DJ, Loughin CA. Diagnostic imaging of the
canine stifle: a review. Vet Surg 2010;39:284–295.
Olstad KL, Kongsro J, Grindflek E, et al. Ossification
defects detected in CT scans represent early osteochondrosis in the distal femur of piglets. J Orthop
Res 2014;32:1014–1023.
Samii VF. Computed tomographic arthrography of
the normal canine stifle. Vet Radiol Ultrasound
2004;45:402–406.
Samii VF, Pozzi A, Drost WT, et al. Computed tomographic arthrography of the stifle for detection of
cranial and caudal cruciate ligament and meniscal
tears in dogs. Vet Radiol Ultrasound 2009;50:144–
150.
Soler M, Murciano J, Latorre R, et al. Ultrasonographic, computed tomographic and magnetic resonance imaging anatomy of the normal canine stifle joint. Vet J 2007;174:351–361.
Sungyoung Han, Haengbok Cheon, Hangmyo Cho,
et al. Evaluation of partial cranial cruciate ligament
rupture with positive contrast computed tomographic arthrography in dogs. J Vet Sci 2008;9:395–
400.
Tivers MS, Mahoney P, Corr SA. Canine stifle
positive contrast computed tomography arthrography for assessment of caudal horn meniscal
injury: a cadaver study. Vet Surg 2008;37:269–
277.
Vande Berg BC, Lecouvet FE, Poilvache P, et al. Spiral
CT arthrography of the knee: technique and value
in the assessment of internal derangement of the
knee. Euro Radiol 2002;12:1800–1810.
Vasseur P. Stifle joint. In: Textbook of Small Animal
Surgery, Slatter D, ed. Second edition. Philadelphia
PA, WB Saunders. 1993, pp. 1817–1865.
VetBooks.ir
21
Magnetic Resonance Imaging
of the Stifle
Peter V. Scrivani
Introduction and image acquisition
Joints limit motion between bones to a particular range, and also dissipate stress during use
(Dyce et al. 2002). The ability to perform these
functions is based on the type of joint (synovial,
cartilaginous, fibrous), bone conformation, and
supporting soft tissues (Dyce et al. 2002). Therefore, a loss of function is manifested as excessive
motion, restricted motion, or pain. In dogs the
most common cause of joint dysfunction is
osteoarthritis, a chronic degenerative disease of
the articular cartilage and underlying bone that
results from a combination of genetic and environmental factors. Other common arthropathies
are due to inflammatory, traumatic, or neoplastic causes. Relative to this information and to
the stifle joint in particular, the aims of magnetic
resonance imaging (MRI) are: (i) to provide an
early diagnosis of osteoarthritis; (ii) to provide
a more specific diagnosis of the arthropathy;
(iii) to guide therapy decisions; (iv) to offer a
more detailed prognosis; and (v) to assess any
response to treatment. MRI is apt to improve
patient care and help achieve one of these
goals.
The beneficial impact of musculoskeletal
MRI in humans is undisputed. However, only
minimal evidence is yet available in veterinary
medicine that MRI actually improves patient
care relative to the cost of the examination and
additional anesthesia time. Even though MRI is
considered accurate for diagnosing cruciate ligament rupture (CR) in dogs (Galindo-Zamora
et al. 2013), competing diagnostic modalities, such as radiography, ultrasonography, or
arthroscopy, offer additional benefits such as
guiding therapy without the need for anesthesia
or providing the ability to treat an underlying
problem during the same procedure. However,
MRI has shown much promise and may have
advantages in the early detection of lesions in
the cranial cruciate ligament (CrCL), subchondral bone, articular cartilage or menisci, or for
establishing the cause of lameness that has not
been diagnosed by conventional methods. As
such, MRI is being used more frequently to
examine the stifle joint in dogs. The anatomy
of the stifle joint has been described previously
(Pujol et al. 2011).
MRI recognition of joint lesions is based
on alterations of signal intensity (SI) and
morphologic changes (Rubin 2005). For subtle
lesions, detecting these changes depends on
acquiring images with high contrast and spatial
resolution (Rubin 2005). It is difficult to make
exact recommendations for optimal image
acquisition because of different scanners (e.g.,
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
155
VetBooks.ir
156
Clinical Features
low-field, high-field), various manufacturer
names for sequences, individual preferences,
minimal evidence of efficacy of one protocol
versus another, various breed conformations,
and coils and algorithms that are optimized for
humans. As a basic protocol, the joint should
be examined using a local coil, preferably one
that surrounds the joint, and the joint should be
located in the magnetic isocenter. The degree
of joint flexion may be dictated by coil configurations, but 90◦ flexion may improve imaging
of the CrCL (Podadera et al. 2014). Proton
density (PD) weighted fast spin–echo (SE)
sequences should be obtained in the transverse,
sagittal, and dorsal planes using a small fieldof-view centered on the area of interest and,
importantly, a large matrix size. Additionally,
a fat-suppressed PD-weighted sequence (e.g.,
short-tau inversion recovery or STIR) should
be obtained in one, two, or three planes. For
larger joints, a slice thickness of 3–4 mm should
be used, but for smaller joints use 1–2 mm
slices. Very thin slices (1 mm) may require a
T2-weighted 3D gradient recall echo sequence.
Additional sequences or planes may be of use
in certain conditions. Intravenous or intraarticular contrast medium is not used routinely.
Image orientation is accomplished by obtaining
scout images in three planes. The dorsal plane
is aligned parallel to the patellar tendon on the
sagittal scout and parallel to the caudal aspect
of the femoral condyles on the transverse scout.
The transverse plane is made parallel to the
distal aspect of the femoral condyles on the
dorsal scout and perpendicular to the patellar
tendon on the sagittal scout. The sagittal plane
is made such that slices bisect the patellar
tendon and intercondylar fossa of the femur on
the transverse scout and parallel to the patellar
tendon on the dorsal scout (Winegardner et al.
2007). High-quality images depend on the
patient being still, which often requires anesthesia. Implants or metallic objects may reduce
image quality (Banfield & Morrison 2000). This
point may be moot when surgical implants
or metal debris are far enough away from
structures of interest, such as the cruciate ligaments or medial meniscus, to not interfere with
interpretation (David et al. 2012a). Additionally,
alterations to image acquisition parameters can
reduce the severity of the susceptibility artifact
to produce a diagnostic image (David et al.
2012b; Simpler et al. 2014). High-field scanners
provide superior signal-to-noise ratio, but
are not always available.
Synovial structures
Evaluation of synovial joints is one of the most
important reasons for hospital visits relating to
gait abnormality or lameness. Synovial joints
consist of a fibrous joint capsule, synovial membrane, fluid-filled joint space, and articular cartilage (Dyce et al. 2002). The combination of the
joint capsule and synovial membrane is seen as
a low SI structure on MR images (Rubin 2005).
The synovial membrane usually is too small to
differentiate as a separate structure: it also lines
joint recesses, bursas, and tendon sheaths. The
normal synovial membrane does not enhance
(or only minimally enhances) after intravenous
contrast-medium administration (Rubin 2005).
An inflamed synovial membrane is thick and
may be nodular or mass-like, especially when
chronic (Rubin 2005). When there is active
inflammation the synovial membrane rapidly
enhances with intravenous contrast-medium
administration (Rubin 2005). Therefore, intravenous contrast-medium administration might
be helpful when an inflammatory arthropathy (e.g., immune-mediated, infectious) is suspected. Joint effusion (Figure 21.1) that is due
to increased synovial fluid production has similar signal characteristics as normal joint fluid.
Joint fluid that contains proteinaceous debris or
blood products has a decreased (darker) and
variable SI (Rubin 2005). This different appearance may be referred to as ‘dirty’ versus ‘clean’
fluid. The appearance of normal articular cartilage reflects its chemical composition and threedimensional histological organization (Rubin
2005). For example, articular cartilage has a lowPD SI that progressively increases from deep-tosuperficial. Cartilage abnormalities appear as
defects or SI changes in the smooth articular
surface, which may extend to the subchondral
bone plate. Traumatic articular lesions are often
sharply demarcated (Rubin 2005).
Meniscus
Within the stifle joint, there are lateral and
medial menisci, which are crescent-shaped
VetBooks.ir
Magnetic Resonance Imaging of the Stifle
Figure 21.1 Sagittal (A) proton
density MR image and sagittal (B)
SE T2-weighted MR image of a
2-year-old, neutered female
Mastiff with a complete rupture
of the cranial cruciate ligament.
There is increased fluid within
the stifle joint. Compare the SI of
the ‘clean’ (arrows) and ‘dirty’
synovial fluid (∗ ) on the two
images.
(A)
fibrocartilaginous structures that partially
divide the joint cavity and provide structural
integrity during movement (Dyce et al. 2002).
Each meniscus has unnamed cranial-tibial and
caudal-tibial ligaments. The lateral meniscus
also has an attachment to the femur, the meniscofemoral ligament. The transverse ligament
connects the cranial-tibial ligaments of the
two menisci. The normal MRI appearance of
the meniscus is triangular or bow-tie shape
(sagittal and dorsal planes) with uniform low
SI, although some exceptions regarding SI exist
(Martig et al. 2006). Meniscal tears are common
in dogs secondary to CR: the medial meniscus
is affected more commonly (Blond et al. 2008).
Meniscal tears may be present at the time of
CR diagnosis, or they may develop weeks to
months after surgical treatment (Taylor-Brown
et al. 2014). The MRI appearance of a meniscal
tear is a primarily linear intrameniscal area
of high SI that extends definitively to one or
both articular surfaces, or abnormal meniscal
shape (Figure 21.2) (Rubin 2005; Blond et al.
2008).
Figure 21.2 Sagittal (A) SE
T2-weighted MR image of a
2.5-year-old, neutered female
Saint Bernard and (B) sagittal SE
T2-weighted MR image of a
2.5-year-old, neutered female
Rottweiler. Compare the normal
appearance of the medial
meniscus (A) to the abnormal (B).
A full-thickness tear is present in
the cranial part of the medial
meniscus (arrow) and the caudal
portion is absent (∗ ).
(A)
157
(B)
A grading system for describing meniscal
injuries during MRI has been proposed in dogs,
ranging from 0 (normal) to 4 (Martig et al.
2006). However, the reported accuracy of MRI
signs for diagnosing meniscal tears has varied
from poor to good (Blond et al. 2008; Böttcher
et al. 2012; Galindo-Zamora et al. 2013). Falsepositive results for meniscal tears may be due
to misinterpretation of the appearance of normal structures adjacent to the meniscus, or to
artifact (Baird et al. 1998; Hashemi et al. 2004). A
truncation artifact appears as alternating bright
and dark bands at high-contrast interfaces such
as the meniscus and synovial fluid (Figure 21.3)
(Hashemi et al. 2004). It is due to an inability
to approximate exactly a step-like change in the
signal intensity due to a limited number of samples or sampling time, and usually occurs in
the phase direction (Hashemi et al. 2004). It may
be remedied by increasing the sample time to
reduce the ripples, or by decreasing the pixel
size by increasing the number of phase encodes
or decreasing the field of view (Hashemi et al.
2004).
(B)
Clinical Features
VetBooks.ir
158
(A)
Figure 21.3 Sagittal (A) SE
T2-weighted MR image of a
2-year-old, intact male Great
Dane and (B) dorsal SE
T1-weighted MR image of a
2.5-year-old, neutered female
Rottweiler. Note the linear,
high-SI band within the meniscus
(arrows) that are parallel to the
interface between meniscus and
synovial fluid that does not
extend to the articular surface.
(B)
Tendons, ligaments, and muscles
Tendons, ligaments, and muscles of the stifle joint (Table 21.1; Figures 21.4–21.9), along
with bone conformation, restrict movement primarily to a cranio-caudal plane with minimal
rotation and slide. Tendons and ligaments normally appear as homogeneous, low-SI, sharply
margined linear structures, and on cross-section
are round, oval, or flat (Rubin 2005; Soler et al.
2007). However, the quadriceps tendon, in contrast to the patellar tendon, may normally have
parallel hyperintense and hypointense linear
striations due to a coarse fiber pattern. A higher
SI may also be seen normally if muscle is interspersed with the fibers, or if the orientation
of the fibers approaches 55◦ relative to the
magnetic field (magic-angle artifact) (Spriet &
McKnight 2009). During tendon degeneration
or ligament sprain the structure may have an
increased SI, an altered size (usually increased),
irregular margins, or abnormal shape (Rubin
2005; Stahl et al. 2010). With an acute tendon
or ligament tear, total discontinuity may be
Table 21.1 Key for Figures 21.4–21.9.
Anatomic structures
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
Femur
Patella
Tibia
Fibula
Lateral collateral ligament
Medial collateral ligament
Meniscofemoral ligament
Cranial cruciate ligament
Caudal cruciate ligament
Transverse ligament
Quadriceps muscle
a. Vastus lateralis muscle
b. Vastus intermedius muscle
c. Rectus femoris muscle
d. Vastus medialis muscle
e. Quadriceps tendon
f. Patellar tendon
Infrapatellar fat pad
Sartorious muscle
a. Cranial
b. Caudal
Biceps femoris muscle
Abductor cruralis caudalis muscle
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
Semitendinous muscle
Semimembranosus muscle
Gracilis muscle
Adductor muscle
Aponeurosis of pectineus muscle
Long digital extensor muscle
a. Tendon
Extensor hallucis longus muscle
Fibularis longus muscle
(formerly peroneus longus)
Lateral digital extensor muscle
Flexor hallucis longus muscle
Popliteus muscle
a. Tendon
b. Sesamoid bone
Cranial tibial muscle
Caudal tibial muscle
Long digital flexor muscle
Gastrocnemius muscle
a. Fabella (sesamoid bone)
b. Lateral head
c. Medial head
Superficial digital flexor muscle
VetBooks.ir
Magnetic Resonance Imaging of the Stifle
11e
Figure 21.4 Sagittal (A) proton
density MR image of a
2-year-old, neutered female
Chesapeake Bay Retriever and
(B) dorsal SE T1-weighted MR
image of a 2.5-year-old, neutered
female Saint Bernard. The cranial
aspect of the joint capsule and
synovium (black arrow) is seen
immediately caudal to the
infrapatellar fat pad. For key to
labels, see Table 21.1.
159
1
1
2
5
6
11f
30
12
4
3
3
(A)
(B)
1
8
1
5
9
3
8
(A)
7
(B)
Figure 21.5 Sagittal (A) SE T2-weighted MR image of a 10-year-old, neutered female Labrador Retriever and (B)
transverse SE T1-weighted MR image of a 2.5-year-old, neutered female Saint Bernard. The proximal attachment of the
cranial cruciate ligament is on the medial aspect of the lateral femoral condyle. The proximal attachments of the caudal
cruciate and menisco-femoral ligaments are on the lateral aspect of the medial femoral condyle. The distal attachments
of the cruciate ligaments are on the tibia. The distal attachment of the menisco-femoral ligament is on the lateral
meniscus. For key to labels, see Table 21.1.
extensor
fossa
1
1
26b
26a
12
Figure 21.6 Sagittal SE
T1-weighted MR images of a
2.5-year-old, neutered female
Great Dane, depicting some
normal anatomic structures. For
key to labels, see Table 21.1.
3
3
(A)
21a
(B)
4
160
Clinical Features
VetBooks.ir
30a
30c
21a
Figure 21.7 Sagittal (A) proton
density MR image and (B)
transverse SE T1-weighted MR
image of a 2-year-old, male
Great Dane, depicting some
normal anatomic structures. The
caudal aspect of the joint capsule
and synovium (black arrow) is
seen between the joint space and
gastrocnemius muscle. For key to
labels, see Table 21.1.
1
3
3
4
(A)
(B)
Figure 21.8 Dorsal (A) and
transverse (B) SE T1-weighted
(TR860/TE26) MR images of a
2-year-old, neutered female
Chesapeake Bay Retriever,
depicting some normal anatomic
structures. The transverse scan is
obtained through both menisci:
the menisci (arrows) appear as
apposing crescents with
heterogeneous low SI due to
slice thickness artifacts. For key
to labels, see Table 21.1.
12
1
10
7
3
3
4
(A)
(B)
craniolateral
13a
11a
11c
11b
22
1
14
15
16
27
11d
13b
19
24
21
3
23
20
26
4
14
28
25
17
15
30b
31
29
30c
18
(A)
(B)
caudomedial
Figure 21.9 Schematic transverse section through the thigh (A) and crus (B) depicting the anatomic relationship of
muscles and bones. The positional relationship of the supporting musculature is important when assessing joints. For key
to labels, see Table 21.1. Source: Evans & de Lahunta 2012. Reproduced from Miller’s Anatomy of the Dog, with
permission of Elsevier.
VetBooks.ir
Magnetic Resonance Imaging of the Stifle
Figure 21.10 Sagittal (A) SE
T1-weighted MR image of a
9-year-old, intact female,
mixed-breed dog and sagittal (B)
SE T1-weighted MR image of a
2.5-year-old, neutered female
Great Dane. Note the normal
caudal cruciate ligament (CaCL,
double arrow) and cranial
cruciate ligament (CrCL, single
arrow) (A). In the other dog (B),
the CaCL (double arrow) is visible
and the CrCL is completely torn.
(A)
detected (Rubin 2005). With a chronic ligament
tear, there may be complete absence of the ligament or a low-SI scar that does not have the normal morphology of the ligament (Figure 21.10)
(Rubin 2005).
Bone
Cortical bone has a uniform low SI on all
sequences: the normal periosteum is not
visible (Rubin 2005). New bone formation
(periosteal, osteophytes, enthesophytes) has an
intermediate-to-low SI, and is differentiated by
location on the bone (Rubin 2005; D’Anjou et al.
2008). The SI of yellow bone marrow is similar
to that of fat (high T1 and T2 SI), while red marrow has a slightly lower T1 SI (Rubin 2005; Armbrust et al. 2008). In dogs, the SI of the marrow
in the femoral condyles on short T1 inversion
recovery (STIR) images varies with age. At 4
months, the SI relative to fat is inhomogeneous
and intermediate-to-low: at 8–16 months there
Figure 21.11 Dorsal GE STIR
MR image of a 2-year-old,
neutered female Chesapeake Bay
Retriever (A) and a 2-year-old,
intact male Great Dane (B).
Compare the normal appearance
(A) to the high-SI lesions (arrows)
at the proximal and distal
attachments of the cranial
cruciate ligament (B).
(A)
161
(B)
is a uniformly low SI (Armburst et al. 2008). On
STIR images, high-SI lesions may be detected
in the bone marrow and be due to trauma
(blunt or repetitive), hyperemia, ischemia,
infarction, inflammation, or neoplasia (Rubin
2005).
In dogs with CR, it is common to detect varying degrees of increased SI on STIR images that
are deep to the proximal and distal attachments
of the CrCL (Figure 21.11) (Baird et al. 1998;
Martig et al. 2007; Winegardner et al. 2007; Olive
et al. 2014). Whereas these lesions develop after
surgical resection of CrCL, they have also been
observed in dogs with a partial CR or an intact
CrCL (Winegardner et al. 2007). This observation suggests that multiple pathogeneses are
possible, and questions whether the surgical
model of osteoarthrosis is the best representation of CR in dogs. Additionally, the location
of high-SI lesions is different compared to
people with anterior cruciate ligament rupture,
which further suggests a different or multiple
pathogeneses.
(B)
VetBooks.ir
162
Clinical Features
Conclusions
Musculoskeletal MRI continues to be an emerging technique in veterinary medicine. For many
patients there is minimal evidence to show that
MRI is better than other types of examination
when justified for cost and risk. However, musculoskeletal MRI is being used more frequently
in veterinary medicine and is helpful, especially
in patients with an elusive diagnosis or multiple joint abnormalities. Continued research
also has the potential to show improved patient
care through early lesion detection, to provide a better understanding of pathogenesis,
and to lead to earlier, novel, or more specific
treatments.
References
Armbrust LJ, Ostmeyer M, McMurphy R. Magnetic
resonance imaging of bone marrow in the pelvis
and femur of young dogs. Vet Radiol Ultrasound
2008;49:432–437.
Baird DK, Hathcock JT, Kincaid SA, et al. Lowfield magnetic resonance imaging of early subchondral cyst-like lesions in induced cranial cruciate ligament deficient dogs. Vet Radiol Ultrasound
1998;39:167–173.
Banfield CM, Morrison WB. Magnetic resonance
arthrography of the canine stifle joint: technique
and applications in eleven military dogs. Vet Radiol
Ultrasound 2000;41:200–213.
Böttcher P, Armbrust L, Blond L, et al. Effects of
observer on the diagnostic accuracy of low-field
MRI for detecting canine meniscal tears. Vet Radiol
Ultrasound. 2012;53:628–635.
Blond L, Thrall DE, Roe SC, et al. Diagnostic accuracy
of magnetic resonance imaging for meniscal tears
in dogs affected with naturally occurring cranial
cruciate ligament rupture. Vet Radiol Ultrasound
2008;49:425–431.
D’Anjou MA, Moreau M, Troncy E, et al. Osteophytosis, subchondral bone sclerosis, joint effusion and
soft tissue thickening in canine experimental stifle
osteoarthritis: comparison between 1.5T magnetic
resonance imaging and computed radiography. Vet
Surg 2008;37:166–177.
David FH, Grierson J, Lamb CR. Effects of surgical
implants on high-field magnetic resonance images
of the normal canine stifle. Vet Radiol Ultrasound
2012a;53:280–288.
David FH, Grierson J, Lamb CR. Reducing susceptibility artefacts in magnetic resonance images of the
canine stifle following surgery for cranial cruciate
ligament deficiency. Vet Comp Orthop Traumatol
2012b;25:488–497.
Dyce KM, Sack WO, Wensing CJG. Textbook of Veterinary Anatomy. Third edition. Philadelphia PA, WB
Saunders. 2002.
Evans H, de Lahunta A. Miller’s Anatomy of the Dog.
Fourth edition. Philadelphia PA, WB Saunders.
2012.
Galindo-Zamora V, Dziallas P, Ludwig DC, et al.
Diagnostic accuracy of a short-duration 3 Tesla
magnetic resonance protocol for diagnosing stifle
joint lesions in dogs with non-traumatic cranial
cruciate ligament rupture. BMC Vet Res 2013;9:40.
Hashemi RH, Bradley WG, Lisanti CJ. MRI The
Basics. Second edition. Philadelphia PA, Lippincott
Williams & Wilkins. 2004.
Martig S, Konar M, Schmökel HG, et al. Low-field
MRI and arthroscopy of meniscal lesions in ten
dogs with experimentally induced cranial cruciate ligament insufficiency. Vet Radiol Ultrasound
2006;47:515–522.
Martig S, Boisclair J, Konar M, et al. MRI characteristics and histology of bone marrow lesions in
dogs with experimentally induced osteoarthritis.
Vet Radiol Ultrasound 2007;48:105–112.
Olive J, d’Anjou MA, Cabassu J, et al. Fast presurgical magnetic resonance imaging of meniscal tears
and concurrent subchondral bone marrow lesions.
Study of dogs with naturally occurring cranial cruciate ligament rupture. Vet Comp Orthop Traumatol 2014;27:1–7.
Podadera J, Gavin P, Saveraid T, et al. Effects of stifle flexion angle and scan plane on visibility of
the normal canine cranial cruciate ligament using
low-field magnetic resonance imaging. Vet Radiol
Ultrasound 2014;55:407–413.
Pujol E, Van Bree H, Cauzinille L, et al. Anatomic
study of the canine stifle using low-field magnetic
resonance imaging (MRI) and MRI arthrography.
Vet Surg 2011;40:395–401.
Rubin DA. Magnetic Resonance Imaging: Practical
Considerations. In: Bone and Joint Imaging, Resnick
D, Kransdorf MJ, eds. Third edition. Philadelphia
PA, Elsevier Saunders. 2005.
Simpler RE, Kerwin SC, Eichelberger BM, et al. Evaluation of the WARP-turbo spin echo sequence for
3 Tesla magnetic resonance imaging of stifle joints
in dogs with stainless steel tibial plateau leveling osteotomy implants. Vet Radiol Ultrasound
2014;55:414–419.
Soler M, Murciano J, Latorre R, et al. Ultrasonographic, computed tomographic and magnetic resonance imaging anatomy of the normal canine stifle joint. Vet J 2007;174:351–361.
Spriet M, McKnight A. Characterization of the magic
angle effect in the equine deep digital flexor tendon
using a low-field magnetic resonance system. Vet
Radiol Ultrasound 2009;50:32–36.
VetBooks.ir
Magnetic Resonance Imaging of the Stifle
Stahl C, Wacker C, Weber U, et al. MRI features of gastrocnemius musculotendinopathy in herding dogs.
Vet Radiol Ultrasound 2010;51:380–385.
Taylor-Brown F, Lamb CR, Tivers MS, et al. Magnetic
resonance imaging for detection of late meniscal
tears in dogs following tibial tuberosity advancement for treatment of cranial cruciate ligament
163
injury. Vet Comp Orthop Traumatol 2014;27:141–
146.
Winegardner KR, Scrivani PV, Krotscheck U, et al.
Magnetic resonance imaging of subarticular bone
marrow lesions in dogs with stifle lameness. Vet
Radiol Ultrasound 2007;48:312–317.
VetBooks.ir
VetBooks.ir
22
Risk Prediction of Cruciate
Ligament Rupture using Stifle
Diagnostic Imaging
Peter Muir
Introduction
Cruciate ligament rupture (CR) is a common
condition and is generally evaluated by physical examination. Over time, understanding of
the disease mechanism has increased. CR is now
recognized as a complex trait with genetic and
environmental components that contribute to
the risk of disease. As arthroscopy has been
used more widely for clinical evaluation and
surgical treatment during the past 15 years, it
has now been established that the pathogenesis of CR is characterized by the development
of subtle matrix damage, particularly in the cranial cruciate ligament (CrCL), and an associated inflammatory response within the stifle
joint (Bennett et al. 1988; Bleedorn et al. 2011).
Over time, progressive fiber tearing in the cruciate ligament complex, and the CrCL in particular, over a period of weeks to potentially many
months; leads to the development of an unstable stifle and complete CR (Muir et al. 2011).
As the disease becomes chronic, development
of bilateral CR is common (Muir et al. 2011).
Clinical diagnosis is centered around physical examination of the stifle. However, CR can
sometimes be difficult to diagnose by the classical tests of clinical cranial drawer and cranial tibial thrust. This is particularly true in the
early phase of the disease, when physical examination signs may be subtle, or in the chronic
phase of the disease when stifle instability may
be influenced by factors such as osteoarthritis
and periarticular fibrosis.
In dogs with stifle clinical signs suggestive
of CR, but no cranial drawer or cranial tibial
thrust, incipient CR should be suspected and
confirmed by further investigation. Dogs with
partial CR have a stable stifle (Grade I sprain).
Clinically, a soft stop to the cranial drawer test
may be identified in some dogs, suggesting
very mild cranial tibial translation (Grade II
sprain). Diagnostic imaging, particularly radiography, can be very useful to support the
diagnosis of CR, particularly in the early phase
of the disease. Recent studies have suggested
that diagnostic imaging is predictive of disease
progression (e.g., Chuang et al. 2014; Fuller
et al. 2014). This knowledge is important as it
enables refinement in patient diagnosis and
management through inference from diagnostic
imaging.
Radiography
The knowledge that subsequent contralateral
rupture is a common event in dogs with
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
165
VetBooks.ir
166
Clinical Features
unilateral CR has been used to investigate the
predictive value of stifle radiography through
the evaluation of bilateral radiographs at initial diagnosis (Bleedorn et al. 2011; Muir et al.
2011). Radiography is a more sensitive marker
of disease than physical examination, and
arthroscopy is a more sensitive marker than
radiography, particularly with regards to the
assessment of the severity of synovial effusion
and associated joint inflammation (Chuang et al.
2014; Fuller et al. 2014). Even very subtle radiographic change, particularly synovial effusion,
is clinically relevant to the diagnosis of partial
or complete CR (Bleedorn et al. 2011; Muir et al.
2011; Chuang et al. 2014; Fuller et al. 2014). During initial epidemiological studies of CR disease progression in dogs with unilateral CR,
the proportion of dogs developing subsequent
contralateral rupture was investigated, and this
risk was found to be about 50% at 12 months
after the initial diagnosis (Doverspike et al. 1993;
Moore & Read 1995; de Bruin et al. 2007; Cabrera
et al. 2008; Buote et al. 2009).
By using the Kaplan–Meier estimator, the
time to contralateral CR in dogs with unilateral CR at diagnosis was studied in more detail
in three groups of dogs (Cabrera et al. 2008;
Buote et al. 2009; Muir et al. 2011). Median time
to contralateral rupture was found to range
from 809 to 1,227 days in the three groups
(Muir et al. 2011). Subsequent contralateral rupture occurred in 54% of dogs during the study
period, with an overall time to contralateral
rupture of 947 days (Muir et al. 2011). Median
time to contralateral rupture was reduced by
neutering in both male and female dogs, and
was inversely correlated to a weak degree with
tibial plateau angle (Muir et al. 2011).
To determine whether it is feasible to use
radiographic assessment of synovial effusion
and osteophytosis to make inferences regarding
fiber damage in the cruciate ligament complex,
more recent studies have examined the development of contralateral rupture in dogs diagnosed with unilateral complete CR and contralateral partial CR. Radiographic grading of
the contralateral stifle joint for the severity of
synovial effusion and osteophytosis at diagnosis is strongly predictive of the risk of CR
(Chuang et al. 2014; Fuller et al. 2014), even when
the contralateral stifle is deemed clinically normal by palpation (Fuller et al. 2014). If com-
pression of the infrapatellar fat pad extends cranial to the cranial margin of the medial tibial
condyle, or leads to bulging of the caudal joint
capsule radiographically, then synovial effusion
is sufficiently severe to have obvious effects on
risk of disease progression over time (Chuang
et al. 2014; Fuller et al. 2014). Similar inferences
can be made if moderate to severe radiographic
osteophytosis is present (Chuang et al. 2014;
Fuller et al. 2014).
At initial diagnosis, the severity of stifle synovial effusion and osteophytosis is correlated
(Figure 22.1) (Chuang et al. 2014). In stifles with
partial CR and moderate to severe stifle synovial effusion or stifle osteophytosis, odds of
developing complete CR and an unstable stifle
in the next 12 months is approximately 10-fold
greater than for stifles with milder radiographic
change (Chuang et al. 2014). Time to development of complete CR is significantly decreased
by this severity of radiographic change (Figures 22.2 and 22.3). Breed of dog, age, body
weight, gender and tibial plateau angle each
have little effect on the risk of progression of disease from partial to complete CR (Chuang et al.
2014).
Magnetic resonance imaging
Recent work has determined that assessment of
stifle radiographs in dogs with CR can enable
inference to be made regarding the extent of
fiber damage in the cruciate ligament complex,
particularly the CrCL. A potential advantage of
magnetic resonance (MR) imaging is that the
cruciate ligament tissue can be assessed directly
for pathological change. MR images with sufficient resolution for assessment of the cruciate ligament complex are best acquired using a
3.0 Tesla magnet and isotropic sequences, such
as 3D Fast Spin Echo (FSE) Cube (Racette et al.
2016). In dogs with normal cruciate ligaments,
estimation of CrCL volume using MRI is predictive of ligament structural properties (Racette
et al. 2016). A fiber loss of 70–80% or more in the
CrCL tissue is typically seen in stifles with complete CR. In the future, it is likely that this type
of assessment will also enable inference regarding the risk of progression from partial CR to
complete CR.
Risk Prediction of Cruciate Ligament Rupture using Stifle Diagnostic Imaging
(B)
40
22
20
35
18
16
25
14
Frequency
20
15
12
10
8
6
4
2
10
5
2
Os
de
gra
is tifle
s
o
ls
yt
ph era
teo lat
Os ontra
c
2
e
0
0
0
1
1
e
rad le
n g l stif
o
i
us era
Eff ralat
nt
co
2
1
te
op
in hyt
de o
x sis
st
ifl gra
e
d
3
3
2
Ef
fu
in sio
de n
x gr
st ad
ifl e
e
1
Frequency
30
0
VetBooks.ir
(A)
167
Figure 22.1 Relationship of osteoarthritic changes in the index and contralateral stifles in dogs with unilateral complete
cruciate ligament rupture (CR) and contralateral partial CR. (A) Bivariate histogram of radiographic synovial effusion
grade in index and contralateral stifles. (B) Bivariate histogram of osteophytosis grade in index and contralateral stifles.
Severity of osteophytosis (SR = 0.39, P < 0.0005), but not synovial effusion (SR = 0.17, P = 0.13) in the index and
contralateral stifles were correlated (n = 85 dogs). Source: Chuang et al. 2014, http://journals.plos.org/plosone/
article?id=10.1371/journal.pone.0106389#. Used under CC BY 4.0, https://creativecommons.org/licenses/by/4.0/.
Conclusions
If there is any uncertainty about the diagnosis of CR, bilateral orthogonal stifle radiographs should be made in dogs with pelvic
limb lameness and carefully examined for effusion and osteophyte formation. In dogs with
Index effusion
Index osteophytosis
(B)
Grade 0
Grade 1
Grade 2
100
50
Percent survival
Percent survival
(A)
unilateral CR, bilateral films are important to
fully determine the clinical status of the dog,
particularly with regard to the risk of subsequent contralateral rupture (Chuang et al. 2014;
Fuller et al. 2014). In stifles with partial CR,
including palpably normal stifles on clinical
examination, if moderate to severe radiographic
Grade 0
Grade 1
Grade 2
Grade 3
100
50
0
0
0
1000
2000
Days
3000
0
1000
2000
3000
Days
Figure 22.2 Time to contralateral cranial cruciate ligament rupture (CR) stratified by severity of synovial effusion and
osteoarthritis in the unstable index stifle with complete CR. Kaplan-Meier plots for a population of 85 client-owned dogs
with unilateral complete CR and contralateral partial CR. Time to contralateral complete CR was not significantly
influenced by severity of synovial effusion (A) or osteophytosis (B) in the index stifle. Source: Chuang et al. 2014,
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0106389#. Used under CC BY 4.0, https://creative
commons.org/licenses/by/4.0/.
Clinical Features
Contralateral effusion
Grade 0
Grade 1
Grade 2
100
75
50
25
0
0
1000
2000
Contralateral osteophytosis
(B)
3000
Days
Percent survival
(A)
Percent survival
VetBooks.ir
168
Grade 0
Grade 1
Grade 2
Grade 3
100
50
0
0
1000
2000
3000
Days
Figure 22.3 Time to contralateral cranial cruciate ligament rupture (CR) stratified by severity of synovial effusion or
osteoarthritis in the contralateral stable stifle with partial CR. Kaplan-Meier plots for a population of 85 client-owned
dogs with unilateral complete CR and contralateral partial CR. (A) Time to contralateral complete CR was significantly
decreased in dogs with moderate to severe (Grade 2) radiographic synovial effusion of the contralateral stifle at
diagnosis, when compared with the grades of 0 or 1 (P < 0.001). (B) Time to contralateral CR was significantly decreased
in dogs with Grade 3 osteophytosis of the contralateral stifle at diagnosis, when compared with the grade 0 and grade 2
(P < 0.05). Source: Chuang et al. 2014, http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0106389#.
Used under CC BY 4.0, https://creativecommons.org/licenses/by/4.0/
synovial effusion is present, risk of disease progression to complete CR is substantially higher.
This knowledge is important, particularly with
regard to decision-making over surgical treatment. Tibial plateau leveling osteotomy, in particular, may be helpful in modifying disease
progression in stifles with partial CR (Barger
et al. 2016).
References
Barger B, Piazza A, Muir P. Treatment of stable partial
cruciate rupture (Grade I sprain) in five dogs with
tibial plateau levelling osteotomy. Vet Rec Case Rep
2016;4:e000315.
Bennett D, Tennant B, Lewis DG, et al. A reappraisal
of anterior cruciate ligament disease in the dog.
J Small Anim Pract 1988;29:275–297.
Bleedorn JA, Greuel E, Manley PA, et al. Synovitis in
dogs with stable stifle joints and incipient cranial
cruciate ligament rupture: A cross-sectional study.
Vet Surg 2011;40:531–543.
Buote N, Fusco J, Radasch R. Age, tibial plateau angle,
sex, and weight as risk factors for contralateral rupture of the cranial cruciate ligament in Labradors.
Vet Surg 2009;38:481–489.
Cabrera SY, Owen TJ, Mueller MG, et al. Comparison of tibial plateau angles in dogs with unilateral versus bilateral cranial cruciate ligament rup-
ture: 150 cases (2000–2006). J Am Vet Med Assoc
2008;232:889–892.
Chuang C, Ramaker MA, Kaur S, et al. Radiographic
risk factors for contralateral rupture in dogs with
unilateral cranial cruciate ligament rupture. PLoS
One 2014;9:e106389.
de Bruin T, de Rooster H, van Bree H, et al.
Radiographic assessment of the progression of
osteoarthrosis in the contralateral stifle joint of
dogs with a ruptured cranial cruciate ligament. Vet
Rec 2007;161:745–750.
Doverspike M, Vasseur PB, Harb MF, et al. Contralateral cranial cruciate ligament rupture: Incidence in
114 dogs. J Am Anim Hosp Assoc 1993;29:167–170.
Fuller MC, Hayashi K, Bruecker KA, et al. Evaluation
of the radiographic infrapatellar fat pad sign of the
contralateral stifle joint as a risk factor for subsequent contralateral cranial cruciate ligament rupture in dogs with unilateral rupture: 96 cases (2006–
2007). J Am Vet Med Assoc 2014;244:328–338.
Moore KW, Read RA. Cranial cruciate ligament rupture in the dog – a retrospective study comparing
surgical techniques. Aust Vet J 1995;72:281–285.
Muir P, Schwartz Z, Malek S, et al. Contralateral cruciate survival in dogs with unilateral non-contract
cranial cruciate ligament rupture. PLoS One 2011;6:
e25331.
Racette M, Al Saleh H, Waller KR, 3rd , et al. 3D FSE
Cube and VIPR-aTR 3.0 Tesla magnetic resonance
imaging predicts canine cranial cruciate ligament
structural properties. Vet J 2016;209:150–155.
VetBooks.ir
Section IV
Surgical Treatment
Introduction
A large number of different surgical procedures have been described for the treatment of
stifle instability in dogs, and decision-making
regarding surgical treatment for cruciate ligament rupture (CR) remains controversial. Currently, widely used surgical procedures are
aimed at the treatment of stifle instability,
and not reconstruction or repair of the ruptured cranial cruciate ligament. Stabilization is
accomplished either by osteotomy of the tibia
or by extracapsular stabilization. Historically,
by extrapolation from surgical treatment of
human patients with anterior cruciate ligament
rupture, intra-articular stabilization procedures
have also been popular. Although initial results
in experimental dogs were promising, the use of
intra-articular grafting procedures has become
less popular over time. Recent studies of surgical treatment have challenged the widely held
belief that stifle instability is the primary reason for lameness, particularly in chronically
affected dogs with meniscal damage.
This section provides a detailed discussion of
current surgical procedures used for the treatment of dogs affected with CR. Several new
chapters have been added to this section to
reflect advances in knowledge of surgical treatment of CR over the past five years.
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell. 169
VetBooks.ir
VetBooks.ir
23
Arthroscopy and Arthrotomy
of the Stifle
Brian S. Beale, Donald A. Hulse, Antonio Pozzi, and Peter Muir
Introduction
Arthroscopy has revolutionized the treatment
of joint disease in human beings and animals. Arthroscopic-assisted surgical techniques
improve diagnostic accuracy, reduce postoperative pain and the duration of hospitalization,
and shorten the time required for return to function (Whitney 2003; Hoelzler et al. 2004; Pozzi
et al. 2008; Ertelt & Fehr 2009). Arthroscopy
in animals is used primarily by veterinarians
with advanced surgical training. General practitioners who routinely perform joint surgery
have been slow to adopt arthroscopy due to the
learning curve involved. Consideration should
be given to implementing arthroscopy at the
time of arthrotomy to enhance surgical observation, improve treatment and assist in arthroscopic training. The arthroscopic procedure is
simplified when using arthroscopy at the time
of arthrotomy. Many conditions affecting joints
are best investigated arthroscopically, including
osteochondritis dissecans (OCD) of the shoulder and elbow, ligamentous and tendinous
injuries of the shoulder, fragmented medial
coronoid process, partial cruciate ligament rupture (CR) and meniscal damage (Whitney 2003;
Hoelzler et al. 2004; Pozzi et al. 2008; Ertelt &
Fehr 2009). Arthroscopy via a mini-arthrotomy
has been reported to be an effective method for
treating CR and meniscal injury (Whitney 2003;
Ertelt & Fehr 2009).
Stifle arthrotomy
Arthrotomy of the stifle can be performed in
a traditional open or in a minimally invasive
manner (Hoelzler et al. 2004; Pozzi et al. 2008;
Ertelt & Fehr 2009; Johnson 2014). Traditional
arthrotomy can be performed via a medial or
lateral parapatellar approach depending on the
surgeon’s preference (Johnson 2014). A medial
parapatellar approach will typically facilitate
examination of the medial femoro-tibial joint. A
lateral arthrotomy may be best if lateral extracapsular stabilization is planned, as exposure
of the caudolateral aspect of the joint is easier
(Figure 23.1). A medial arthrotomy may be most
convenient if a tibial osteotomy is to be performed due to the need to have medial exposure
to the tibia.
Arthrotomy should be performed meticulously. The skin is initially incised, followed
by subcutaneous tissue, deep fascia, and joint
capsule. Each tissue layer should be identified
and incised separately. If a lateral parapatellar
approach is used, the deep fascia is incised at
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
171
Surgical Treatment
VetBooks.ir
172
(A)
(B)
(D)
(E)
(C)
Figure 23.1 (A) A lateral parapatellar incision is most commonly used to approach the stifle joint for extracapsular
treatment of cruciate ligament rupture. (B) The deep fascia is incised in a longitudinal direction cranial to the biceps
femoris muscle. The fascial incision is continued distally along the lateral edge of the patellar tendon. (C) The deep fascia
is incised and elevated from Gerdy’s tubercle at the lateral aspect of the proximal tibia. (D) The incision is continued
caudally in a transverse manner, exposing the lateral aspect of the stifle. (E) Retraction of the fascia allows adequate
access to the lateral fabella, the caudal joint capsule, lateral collateral ligament, fibular head, long digital extensor
tendon, extensor groove, and the cranial joint capsule.
the cranial border of the biceps femoris muscle
(Figure 23.1B). The fascial incision is continued
distally 5–10 mm lateral to the edge of the patellar tendon. The deep fascia should be elevated
from the joint capsule and its bony attachment
to Gerdy’s tubercle at the craniolateral aspect
of the proximal tibia (Figure 23.1C). This allows
optimal exposure to the caudal aspect of the stifle and closure of the joint capsule and deep fascia in separate layers. The fascia and attached
biceps muscle is retracted caudally, giving good
exposure to the lateral fabella, lateral condyle
of the femur, fibular head, caudal joint capsule,
long digital extensor tendon extensor groove
and cranial joint capsule. This approach is particularly useful when performing extracapsular
stabilization. The joint capsule is incised longitudinally just lateral to the patellar tendon along
its entire length. The patella is luxated medially. The proximal aspect of the femoropatellar joint and medial and lateral gutters along
the femoral condyles are evaluated for trochlear
groove depth, cartilage integrity, periarticular
osteophytes, and degree of synovitis. The stifle
is flexed and a Gelpi retractor is used to retract
the joint capsule. A Senn retractor is used to
retract the patellar fat pad distally, allowing a
good view of the intercondylar notch, cranial
cruciate ligament (CrCL) and caudal cruciate
ligament (CaCL). If torn cruciate ligament fibers
obstruct viewing of the weight-bearing surfaces
of the femoral condyle and tibial plateau and
the menisci, they should be removed. A portion of the fat pad can also be resected if needed
to improve examination of the joint. However,
care should be taken to avoid damage to the
intermeniscal ligament, which is hidden under
the fat pad. The use of a surgical assistant
will help improve joint exposure. Cranial traction on the Senn retractor or the crus can help
improve exposure of the intra-articular structures by inducing cranial tibial subluxation. In
stifles with substantial periarticular fibrosis this
improved exposure may be limited. The use of a
joint distractor will also help improve exposure.
After optimizing joint exposure, the menisci
should be examined, probed, and treated as
indicated while maintaining joint access.
Some increase in morbidity occurs with
arthrotomy. The initial skin incision must be
VetBooks.ir
Arthroscopy and Arthrotomy of the Stifle
longer and the deeper tissues must be incised.
Incised tissues cause pain due to the initiation of
inflammatory pathways and stimulation of sensory innervation. The surgeon should strive to
minimize soft tissue trauma and surgical pain.
Smaller arthrotomy incisions and meticulous
surgical technique are recommended. Dessication of joint tissues should be avoided by frequent lavage to minimize tissue injury.
Minimally invasive arthrotomy without
luxation of the patella can help to reduce postoperative morbidity, although exposure of the
intra-articular structures is limited, compared
to arthrotomies with patella luxation. The
arthrotomy is made just medial or lateral to
the patellar tendon, extending from the distal
pole of the patella to the proximal tibia. A
Figure 23.2 (A) A minimally
invasive arthrotomy has been
used to explore the stifle. The
joint capsule is retracted using a
small Gelpi retractor. The fat pad
and cranial joint capsule are
retracted distally using a Senn
retractor. (B,C) Examination of
caudal parts of the menisci can
be difficult using an arthrotomy.
A Hohmann retractor can be
used to improve the view of the
menisci. The tip of the retractor is
inserted just caudal to or on the
caudal edge of the proximal tibia.
The body of the retractor is
levered against the trochlear
groove of the femoral condyle.
This action separates the joint
surfaces, giving a better view and
access to the menisci. An
assistant is required when using
this procedure. (D) Distraction
using the Hohmann retractor
provides a good view for
inspection of the menisci and
adequate access for partial
meniscectomy or meniscal
release.
173
small Gelpi retractor is used to retract the joint
capsule (Figure 23.2A). Retraction or resection
of the fat pad helps viewing of the joint. Care
should be taken during the surgical approach
to avoid injury to the cranial meniscotibial ligaments, the transverse meniscal ligament, and
the cranial poles of the menisci. Joint surfaces
should be distracted to facilitate meniscal evaluation and to perform meniscectomies without
damaging cartilage (Figures 23.2B–D and 23.3–
23.5). Potential concerns with mini-arthrotomy
are inadequate viewing and access to the
femoro-tibial joint compartment. This may
increase the possibility of missing a meniscal
tear unless a probe and an arthroscope is used
to improve meniscal examination. In addition,
a partial meniscectomy performed through
(A)
(B)
(C)
(D)
Surgical Treatment
VetBooks.ir
174
Figure 23.3 A Leipzig stifle distractor can be used to
separate the space between the femoral condyle and
tibial plateau, giving an improved view and better access
to the menisci. The distractor is attached to the medial
femoral condyle and proximal tibia using threaded fixator
pins. Distraction is achieved using the turnbuckle device
on the distractor. An assistant is not required when using
this device.
a mini-arthrotomy may be more difficult if
the meniscus does not displace cranially sufficiently. The risk of iatrogenic cartilage damage
may also be higher. The view obtained through
(A)
a mini-arthrotomy may limit the examination
of cruciate ligaments in the intercondylar
notch. These potential concerns become
less relevant as the surgeon becomes more
experienced.
A caudo-medial stifle arthrotomy can be used
in selected cases, to improve exposure of the
caudal pole of the medial meniscus. The arthrotomy is made along the caudal border of the
medial collateral ligament. A needle is used to
palpate the tibia and a 2–3 cm-long incision is
made through the capsule. A small Gelpi retractor allows retraction and exposure of the medial
meniscus. This arthrotomy was found to be
more sensitive for meniscal diagnosis in stable
stifles, such as in dogs with partial CR (Pozzi
et al. 2008). This approach for medial meniscectomy can be used in combination with stifle arthroscopy, when the surgeon is not able to
perform an arthroscopic meniscectomy.
Arthroscopy of the stifle
Arthroscopy of the stifle is the method of choice
for joint exploration (Whitney 2003). The arthroscopic management of dogs with CR reduces
short-term postoperative morbidity compared
to arthrotomy (Hoelzler et al. 2004). The advantages of arthroscopy include magnification and
(B)
Figure 23.4 (A) An intra-articular stifle distractor (Arthrex Vet System) has been placed through the lateral arthroscope
port to distract the joint. (B) An extra-articular human ankle distractor (Arthrex) can also be used to distract the articular
surfaces. Intra-articular distractors offer the advantage of not requiring additional incisions or points of anchorage such as
pins, but are technically more difficult to use because of the limited intra-articular space.
175
VetBooks.ir
Arthroscopy and Arthrotomy of the Stifle
(A)
(B)
(C)
(D)
Figure 23.5 Stifle distraction is recommended to improve meniscal diagnostic accuracy and to perform meniscectomy
with lesser risk of iatrogenic cartilage damage. (A) At initial evaluation without joint distraction the meniscus appears
normal. (B) Following joint distraction using the Arthrex Stifle Distractor the meniscus appears abnormal and a complex
tear is evident. (C) A partial meniscectomy is performed. (D) Further probing of the meniscus allows detection of a
horizontal tear. This example shows the importance of probing the meniscus after partial meniscectomy. Horizontal tears
are common and can progress to bucket-handle or flap tears if left untreated.
illumination, greater access to anatomic regions
of the joint, evaluation of the joint structures in
a fluid medium, and reduced morbidity.
A magnified view of stifle anatomic structures allows a more accurate diagnosis and
more precise treatment of pathologic conditions
(Figure 23.6). Arthroscopic evaluation of the stifle enables more thorough evaluation of the
patella, trochlear groove, femoral condyle, tibial
plateau, CrCL, CaCL, and menisci. Arthroscopy
of the stifle is often used to evaluate and treat
CR and meniscal tears.
Fiber rupture in both the CrCL and the CaCL
can clearly be assessed with arthroscopy, but
can easily be missed with arthrotomy (Figure 23.7). The identification of partial CR, early
in the course of the disease, may be critical for
treatment decision-making and patient management. Early surgical treatment with tibial
plateau leveling osteotomy may protect against
further CrCL fiber disruption and reduce the
Figure 23.6 (A) The cranial and
caudal cruciate ligaments are
more accurately assessed when
viewed with an arthroscope due
to magnification and evaluation in
a fluid medium. The flow of fluid
improves the appearance because
the tissues do not desiccate and
hemorrhage is flushed away. (B) A
bucket-handle tear of the medial
meniscus is better viewed and
more precisely removed using
arthroscopy.
(A)
incidence of meniscal injury and articular cartilage damage.
Examination of the menisci is also improved
as the arthroscope can be positioned adjacent to
the meniscus. Arthroscopy is superior to arthrotomy for the diagnosis of meniscal damage
(Pozzi et al. 2008), especially when combined
with probing. Joint distraction can improve
meniscus exposure and facilitate the diagnosis
and treatment of meniscal injuries. Distraction can be performed with intra- or extraarticular distractors. A joint distractor can be
placed through a lateral portal into the intercondylar notch and levered against the femoral
condyle to separate the joint surfaces and give
better access to the menisci if needed (Figure 23.8). Bucket-handle tears of the medial
meniscus are the most common type of meniscal damage associated with CR. Many of these
tears are not displaced cranially at surgery
and are easily missed. Examining the joint at
(B)
Surgical Treatment
VetBooks.ir
176
(A)
(B)
(C)
Figure 23.7 (A) The cranial
cruciate ligament (CrCL) of this
dog initially appears normal.
(B–D) A partial tear of the
cranial medial band of the CrCL
was found when the proximal
attachment of the ligament was
carefully probed. This CrCL
partial tear would be difficult to
see using traditional arthrotomy.
(D)
different flexion angles and applying tibial
thrust can displace the meniscal tear and facilitate a correct diagnosis. The magnified view
from the arthroscope aids identification of
meniscal damage. The femoral surface of the
caudal horn of the medial meniscus may have
wearing of fibers or a change in character of the
surface. These changes may be difficult to detect
without magnification, and are often associated with minimally displaced medial meniscal tears. Small radial and axial meniscal tears
are also identified more easily with magnification. The meniscus should be carefully probed
on the tibial and femoral surface to assess for
MFC
tears (Figures 23.5 and 23.9). Tear detection is
improved with arthroscopy (Pozzi et al. 2008).
Partial meniscectomy can be performed more
accurately using arthroscopy whilst minimizing articular cartilage damage. Arthroscopicassisted meniscectomy through an arthrotomy
incision (see below) often helps to ensure complete and efficient removal of damaged portions
of the meniscus.
Medial meniscal release helps to reduce
development of postliminary meniscal tears
after treatment of CR. Meniscal release can
be performed under arthroscopic guidance
by transection of the caudal meniscotibial
MFC
MM
MM
TP
(A)
TP
(B)
Figure 23.8 The view of the
medial meniscus (MM) of this
patient is improved using a stifle
distractor. (A) The view and
access to the meniscus is
inadequate initially. (B) With use
of a stifle distractor, meniscal
evaluation and access for partial
meniscectomy is improved.
MFC, medial femoral condyle;
TP, tibial plateau.
VetBooks.ir
Arthroscopy and Arthrotomy of the Stifle
MFC
MFC
MM
177
MFC
MM
BHT
TP
TP
(A)
(B)
(C)
Figure 23.9 Meniscal tears can be difficult to see during routine arthrotomy. (A) This patient appeared to have a normal
meniscus on initial arthroscopic inspection. (B) Careful probing of the medial meniscus revealed a bucket-handle tear.
(C) A partial meniscectomy was performed, leaving the remaining healthy portion of the meniscus intact. MFC, medial
femoral condyle; MM, medial meniscus; TP, tibial plateau; BHT, bucket-handle tear of medial meniscus.
ligament, or by percutaneously incising transversely across the medial meniscus, just caudal
to its attachment to the medial collateral ligament (Whitney 2003) (Figure 23.10).
Magnification of intra-articular structures
allows for more accurate identification of pathological changes to the articular cartilage. Early
degenerative changes to articular cartilage, not
MFC
MM
TP
Figure 23.10 A mid-body medial meniscal release was
performed using a #11 scalpel blade through a
percutaneous stab incision made in the caudal medial
aspect of the stifle joint. Meniscal release can be
accurately performed and assessed using arthroscopy.
MFC, medial femoral condyle; MM, medial meniscus; TP,
tibial plateau.
visible to the naked eye, are clearly seen arthroscopically (Figure 23.11). Fine and coarse fibrillation, superficial erosions and neovascularization of the cartilage are readily evaluated and
documented (Figure 23.11).
Arthroscopic-assisted arthrotomy
Arthroscopy is easier to perform when combined with arthrotomy. An arthroscope can
be introduced into the arthrotomy incision to
enhance the observation of all intra-articular
structures, which is the most important advantage of this approach. Arthroscopic-assisted
arthrotomy provides the surgeon with intraarticular images that are identical to those
obtained by traditional arthroscopy, and thus
enables complete documentation of the changes
observed and treatment provided. By combining these techniques, the arthrotomy incision
can be used for triangulation of the arthroscope and instruments, as well as fluid egress.
This approach not only shortens the learning curve regarding arthroscopic technique but
also reduces fluid leakage into the periarticular soft tissues, a common problem with portal arthroscopy. Smaller arthrotomy incisions
can be made when combined with arthroscopy.
This may help reduce morbidity. The arthroscope can be quickly and easily moved in and
out of the joint as needed. Ease of alignment
of the arthroscope and the anatomic target is
improved. The arthroscope can be positioned
VetBooks.ir
178
Surgical Treatment
MFC
P
MFC
***
***
MM
TP
***
TG
(A)
***
(B)
TP
+++
(C)
Figure 23.11 Arthroscopy improves the ability of the surgeon to assess the condition of articular cartilage. (A) A small
focal area of full-thickness erosion of the femoral cartilage (∗∗∗) is seen on the underside of the patella (P) adjacent to the
trochlear groove (TG) in this patient with medial patellar luxation. (B) Chondromalacia (∗∗∗) of the articular cartilage of
the tibial plateau (TP) can be seen in this patient with cruciate ligament rupture. (C) Fine fibrillation (∗∗∗) of the articular
cartilage of the medial femoral condyle (MFC) and fibrillation and erosion (+++) of the cartilage of the TP can be seen in
this patient with cruciate ligament rupture. Changes to cartilage as seen in panels B and C are typically only visible with
magnification. MM, medial meniscus.
in the desired location by gross observation,
while the anatomic structure of interest can be
assessed more completely using the magnification and the enhanced viewing field provided
by the arthroscope. Instruments are placed adjacent to the arthroscope through the same arthrotomy incision or through an adjacent stab incision used to create an instrument portal. This
technique can be used to help secure the instrument to facilitate surgical operative technique.
Triangulation, an arthroscopic skill that is difficult to learn, is much easier using arthroscopicassisted arthrotomy.
Arthroscopic-assisted arthrotomy typically
uses a mini-arthrotomy without luxation of the
patella (Figure 23.12A). The arthrotomy should
(A)
(B)
be made just medial or lateral to the patellar
tendon, extending from the distal pole of the
patella to the proximal tibia, preserving the
femoro-patellar ligament. A small Gelpi retractor is used to retract the joint capsule (Figure 23.12B). Retraction or resection of the fat
pad allows improved viewing. The proximal
joint pouch and medial and lateral gutters can
be examined by directing the arthroscope proximally (Figure 23.12C). Synovitis and osteophytes can be seen, assessed, and documented
with images obtained using the arthroscopic
camera (Figure 23.13A–C). The cruciate ligaments are inspected (Figure 23.14A). A joint distractor can be used to separate the joint surfaces of the femur and tibia, providing a better
(C)
Figure 23.12 (A) Arthroscopic-assisted arthrotomy can be used to evaluate the stifle with similar advantages to
arthroscopy, but with the ease of arthrotomy. The arthrotomy incision is typically small, as seen in this patient, but any
size arthrotomy incision can be used with arthroscopic assistance. (B) Gelpi retractors can be used to retract the joint
capsule and improve exposure to the joint. (C) The arthroscope is positioned in the proximal aspect of the joint to assess
the patella, trochlear groove, synovial membrane and the medial and lateral gutters for osteophytes. Fluid enters the joint
through the arthroscope cannula and drains from the arthrotomy incision.
VetBooks.ir
Arthroscopy and Arthrotomy of the Stifle
179
SM
LFC
MFC
***
SM
***
(A)
(B)
(C)
Figure 23.13 Arthroscopic-assisted arthrotomy facilitates assessment of intra-articular pathology at the time of
arthrotomy (A). The synovium can be evaluated for hyperplasia, hyperemia, and fibrosis. Synovial biopsies can be
obtained using arthroscopic assistance to ensure that optimal tissue samples are obtained. (B) Small osteophytes (∗∗∗)
along the attachment of the joint capsule to the lateral femoral condyle (LFC) can be seen in this patient having an early
cruciate ligament rupture. Minimal inflammation of the synovial membrane (SM) is seen. (C) Moderate-sized osteophytes
(∗∗∗) are present along the medial femoral condyle (MFC) in this patient with a chronic cruciate ligament rupture. The
synovial membrane (SM) appears hyperplastic in the area of the osteophytes.
view of the menisci (Figures 23.3, 23.4 and
23.14B,C). The joint is then explored using the
magnified view of the arthroscope. Controlling
the position of the arthroscope in the joint can
be more difficult with this technique, compared
with portal arthroscopy. Resting the surgeon’s
hand against the patient or resting the surgeon’s
elbow on a Mayo stand can help avoid a shaky
image and inadvertent withdrawal of the scope
from the joint (Figure 23.15). The surgeon can
also steady the image and prevent inadvertent
withdrawal of the arthroscope by grasping the
shaft of the arthroscope near the arthrotomy
incision (Figure 23.15).
Fluids are delivered through the arthroscope
cannula, similar to portal arthroscopy. The rate
of fluid flow should be lowered because of
reduced resistance to flow from the arthrotomy
incision. Fluid egress occurs freely from the incision and fluid collection should be performed.
Fluid egress can be captured using a drainage
pouch with suction attachment, floor drain, or
simply placing towels or absorbent towels on
the floor (Figure 23.15). A water-impervious
drape should be used to avoid surgical site contamination (Figure 23.15). The tip of the arthroscope should be placed near the target tissue
to provide the best view. Bubbles may obscure
the view if the tip of the scope is drawn too
far away from the tissue (Figure 23.16A). Surgical instruments are used with a combination
of direct and arthroscopic observation. Arthroscopic treatment also helps to minimize cartilage injury. A scrubbed assistant can help to
manipulate an instrument, such as a grasper
or probe, during surgery (Figure 23.16B). The
surgeon typically holds the arthroscope and
the cutting instrument or shaver. The menisci
should be carefully probed to assess for damage
(Figure 23.17). Damaged meniscal tissue, such
as a bucket-handle tear, should be removed by
partial meniscectomy (Figure 23.18). After treatment, the affected area should be re-examined,
using the arthroscope to ensure complete treatment. This is particularly important during
meniscectomy, as it is common to find a second
or third bucket-handle tear after removal of the
first tear (Figure 23.19). The meniscus should
be probed under arthroscopic viewing to ensure
that additional damaged meniscal tissue is not
left behind. Medial meniscal release can also be
performed more accurately using arthroscopic
guidance (Figure 23.20).
Surgical procedures require the use of surgical instruments. Surgeons often use a variety
of instruments for operative procedures in the
joint, including scalpel blades, hemostats, and
thumb forceps. Arthroscopic hand instruments
typically used for traditional arthroscopic
surgery may provide a benefit to surgeons using
arthroscopic-assisted arthrotomy. Arthroscopic
hand instruments are typically low profile, with
180
Surgical Treatment
VetBooks.ir
smooth edges to enhance access to tight regions
of the joint without damaging articular cartilage. They also have been designed with more
secure grasping properties to allow a stronger
grasp of intra-articular structures, to apply
tension, or to remove damaged structures.
Hand instruments designed for arthroscopy
also tend to improve joint observation due to
their ergonomic design and shaft length.
(A)
Stifle joint distraction
Distraction of the femoral and tibial joint surfaces during arthrotomy or arthroscopy is often
achieved using a narrow Hohmann retractor
with an appropriate contour and adequate
stiffness to prevent bending. The tip of the
Hohmann retractor is placed on the caudal
aspect of the tibial plateau. The blade of the
retractor is levered against the trochlear groove
of the femoral condyle, resulting in a separation
of the joint surfaces and improved viewing of
the menisci and the caudal femoro-tibial joint
space. Distraction must be maintained by the
surgeon during the procedure.
Intra-articular joint distraction
(B)
(C)
Figure 23.14 Arthroscopy-assisted arthrotomy. (A) The
cranial cruciate ligament is inspected with a probe.
Diagnosis of partial cruciate ligament rupture is
facilitated because of the magnified view supplied by the
arthroscope. (B) A Hohmann retractor has been inserted
into the mini-arthrotomy adjacent to the arthroscope
allowing an improved view of the menisci. (C) The
menisci are probed while viewed with an arthroscope.
The magnified view and ability to position the
arthroscope into an optimal position next to the meniscus
increases the surgeon’s accuracy in identifying meniscal
tears.
This approach is useful for both arthrotomy and
arthroscopic techniques. Several instruments
are currently available that have an improved
design relative to a Hohmann retractor. These
instruments are placed in the intercondylar
notch to separate the tibial and femoral joint
surfaces, but distraction needs to be maintained
by a surgical assistant. A self-retaining retractor is also available for joint distraction (Gemmill & Farrell 2009). This instrument is typically
positioned through a medial parapatellar portal
incision or through the arthrotomy. The proximal jaw is placed in the intercondylar notch and
the distal jaw in the fat pad before joint distraction (see Figures 23.3 and 23.4).
Extra-articular joint distraction
An extra-articular pin distractor (Böttcher et al.
2009; Winkels et al. 2016) can also be used to separate the joint surfaces of the femur and tibia.
Transcutaneous pins are placed in the distal
181
VetBooks.ir
Arthroscopy and Arthrotomy of the Stifle
(A)
(B)
(C)
(D)
Figure 23.15 During arthroscopy-assisted arthrotomy, the arthroscope can be stabilized by resting the surgeon’s hand
against the patient or a sterile towel positioned on the patient to avoid a shaky image and inadvertent withdrawal of the
scope from the joint (A). (B) The surgeon can steady the image and prevent inadvertent withdrawal of the arthroscope
from the joint by grasping the shaft of the scope near the arthrotomy incision. (C) Fluid egress occurs freely and fluid
collection should be performed. A water-impervious drape is used on patients having arthroscopy-assisted arthrotomy to
avoid contamination of the surgical site. The drape used in this patient is an antimicrobial surgical incise drape with an
iodophor-impregnated adhesive, designed to provide a sterile surface all the way to the wound edge and continuous
antimicrobial activity throughout the procedure. (D) Fluid egress can be captured using a drainage pouch with suction
attachment or a floor drain, or simply placing towels or absorbent towels on the floor.
(A)
(B)
Figure 23.16 (A) The tip of the arthroscope should be placed near the target tissue to provide the best view. Bubbles
will often obscure the view if the tip of the scope is drawn too far away from the tissue of interest. (B) A scrubbed
assistant can be used to hold a grasper or probe during resection of the cranial cruciate ligament remnants or partial
meniscectomy. The surgeon typically holds the scope and the cutting instrument or shaver.
Surgical Treatment
VetBooks.ir
182
MFC
MFC
MFC
MM
MM
BHT
TP
TP
(A)
(B)
(C)
Figure 23.17 The meniscus should be carefully probed to assess for meniscal tears. The meniscus of this patient was
examined using an arthroscopy-assisted arthrotomy technique. (A) The meniscus appears normal. (B) A probe is
introduced to palpate and assess the meniscus for damage. (C) A bucket-handle tear of the medial meniscus is found and
displaced cranially using the probe. MFC,-medial femoral condyle; MM, medial meniscus; TP, tibial plateau; BHT,
bucket-handle tear.
femur and proximal tibia. The design of this
distractor allows the surgeon to use a combination of cranial tibial thrust together with
distraction to optimize viewing of the femorotibial joint (Figures 23.3 and 23.4). Distraction can be maintained by the instrument after
placement.
Use of joint distraction is an important consideration in surgical evaluation of the stifle
joint. Diagnosis of medial meniscal tearing is
improved (Kim et al. 2017; Winkels et al. 2016)
(Figures 23.5 and 23.8). Improved access to the
caudal portion of the medial meniscus also facilitates meniscectomy or medial meniscal release
in both large and small dogs (Kim et al. 2016;
Winkels et al. 2016; Kim et al. 2017). Joint distraction appears a safe procedure that is unlikely to
induce collateral ligament injury or joint injury
from inadvertent pin penetration (Böttcher et al.
2009; Winkels et al. 2016).
Patient morbidity
Postoperative pain
Stifle surgery is a painful procedure. Pain is
generated locally by cellular mechanisms and
MFC
MFC
HK
G
BHT
MM
BHT
TP
MM
(A)
TP
(B)
(C)
Figure 23.18 Bucket-handle tears should be removed by partial meniscectomy. Arthroscopy-assisted arthrotomy allows
the surgeon to perform a partial meniscectomy with great precision. (A) A hook knife is used to cut the abaxial
attachment to the bucket-handle tear of the medial meniscus. (B) The torn portion of the meniscus is grasped and tension
is applied before cutting the axial attachment of the torn fragment. (C) Appearance of the periphery of the medial
meniscus and articular surfaces after partial meniscectomy. MFC, medial femoral condyle; MM, medial meniscus; TP,
tibial plateau; BHT, bucket-handle tear; HK, hook knife; G, grasper.
VetBooks.ir
Arthroscopy and Arthrotomy of the Stifle
the activation of nociceptors, particularly in the
synovium and joint capsule. In dogs with CR,
stifle synovitis also contributes to joint pain
and lameness. Surgical pain can be decreased
by applying appropriate pre-emptive analgesia, adjunctive nonsteroidal anti-inflammatory
drug (NSAID) therapy, and by meticulous surgical technique. Arthroscopic-assisted surgery
is minimally invasive and helps to reduce surgical morbidity. Persistent synovitis has been
identified in injured joints (elbow, hip, stifle)
long-term after arthrotomy or arthroscopy. This
may warrant long-term anti-inflammatory therapy to decrease the insidious progression of
osteoarthritis. Anti-inflammatory treatment can
be provided using NSAIDs or supplements
that have anti-inflammatory properties. Recent
studies have demonstrated similar improvements in the ground reaction forces of dogs with
osteoarthritis of the hips and stifles by treatment using an NSAID or a fatty acid supplement (Kwananocha et al. 2016).
Return to function
Early return to function is desirable to reduce
muscle atrophy and preserve the joint range of
motion after surgery. The loss of muscle mass
may alter forces acting on the joint and thus
influence the progression of stifle joint degeneration. Pain, tissue swelling, activity restriction
Figure 23.19 It is particularly important to reassess the
meniscus with a probe after performing a partial
meniscectomy to treat a bucket-handle tear of the medial
meniscus. It is relatively common to find a second or
even a third bucket-handle tear after removal of the first.
This patient had a triple bucket-handle tear of the medial
meniscus.
and bandaging contribute to postoperative loss
of joint range of motion. Early range of motion
exercise as part of a rehabilitation program (see
Chapter 42) is advantageous due to the tendency for joints to become stiff after surgery.
Periarticular fibrosis may lead to an irreversible
loss of range of motion and morbidity, and
should be minimized. Arthroscopic-assisted
arthrotomy helps to preserve joint range of
motion due to its effect on reducing pain and
swelling after surgery. When combined with
surgical stabilization of the stifle, morbidity is
similar to traditional portal arthroscopy.
MFC
MFC
***
MTL
PK
TP
TP
PK
(A)
183
(B)
Figure 23.20 Medial meniscal release can also be performed more accurately using arthroscopic guidance. (A) A
meniscal release was performed by cutting the medial meniscotibial ligament using a meniscal push-knife. (B) The
caudal horn of the medial ligament has displaced caudally after cutting the ligament. Note the gap (∗∗∗) at the site of
transection of the meniscotibial ligament. MFC, medial femoral condyle; MTL, medial meniscotibial ligament; TP, tibial
plateau; PK, push-knife.
VetBooks.ir
184
Surgical Treatment
References
Böttcher P, Winkels P, Oechtering G. A novel pin
distraction device for arthroscopic assessment of
the medial meniscus in dogs. Vet Surg 2009;38;595–
600.
Ertelt J, Fehr M. Cranial cruciate ligament repair in
dogs with and without meniscal lesions treated by
different minimally-invasive methods. Vet Comp
Orthop Traumatol 2009;22:21–26.
Gemmill TJ, Farrell M. Evaluation of a joint distractor
to facilitate arthroscopy of the canine stifle. Vet Surg
2009;38:588–594.
Hoelzler MG, Millis DM, Francis DA, et al. Results
of arthroscopic versus open arthrotomy for surgical management of cranial cruciate ligament deficiency in dogs. Vet Surg 2004;33:146–155.
Johnson KA. Piermattei’s Atlas of Surgical Approaches to
the Bones and Joints of the Dog and Cat. Philadelphia,
WB Saunders 2014, pp. 392–399.
Kim JH, Heo SY, Lee HB. Arthroscopic detection of
medial meniscal injury in small breed dogs with the
use of a joint distractor. J Vet Sci 2017, epub.
Kim K, Lee H, Ragetly GR. Feasibility of stifle medial
meniscal release in toy breed dogs with and without a joint distractor. Vet Surg 2016;45:636–641.
Kwananocha I, Vijarnsorn M, Kashemsant N, et al.
Effectiveness of disease modifying osteoarthritis agents and carprofen for treatment of canine
osteoarthritis. Thai K Vet Med 2016;46:363–371.
Pozzi A, Hildreth BE, Rajala-Schulz PJ. Comparison
of arthroscopy and arthrotomy for diagnosis of
medial meniscal pathology: an ex vivo study. Vet
Surg 2008;37:749–755.
Whitney WO. Arthroscopically assisted surgery of
the stifle joint. In: Small Animal Arthroscopy, Beale
BS, Hulse DA, Schulz KS, Whitney WO, eds.
Philadelphia, WB Saunders, 2003.
Winkels P, Pozzi A, Cook R, et al. Prospective evaluation of the Leipzig stifle distractor. Vet Surg
2016;45:631–635.
VetBooks.ir
24
Joint Lavage
Peter Muir
Introduction
Pharmacologic treatment of arthritis often
includes systemic or intra-articular administration of various types of drugs, particularly anti-inflammatory drugs. Common
intra-articular therapies used for the treatment of arthritis include corticosteroids and
hyaluronic acid (Jüni et al. 2007; Habib 2009).
However, these treatments may be associated
with adverse effects. Relief from arthritic pain
after joint lavage has been noted by surgeons
performing arthroscopy since 1934 (Burman
et al. 1934). Subsequently, it has been suggested that large-volume lavage or irrigation
of joints may facilitate the removal of cartilage
degradation products, inflammatory cells, proinflammatory cytokines, and matrix-degrading
enzymes. However, this remains a provocative
question which has been little considered in
canine orthopaedic surgery.
Clinical studies
To address the question of joint lavage efficacy, a number of clinical trials have been conducted in human patients, principally studying
human knee osteoarthritis patients. Results of
these trials have been conflicting. It has been
suggested that the benefit of joint lavage is due
to a placebo effect (Bradley et al. 2002). However, in at least one well-controlled trial, when
arthroscopic debridement was compared with
arthroscopic lavage or placebo surgery, arthroscopic procedures did not perform better than
placebo surgery (Moseley et al. 2002). In other
work, knee arthritis patients undergoing arthroscopic lavage have experienced persistent pain
relief for up to 24 weeks (Ravaud et al. 1999).
Comparison of arthroscopic lavage with lavage
plus intra-articular corticosteroids suggested
that little additional benefit is gained from
the use of corticosteroids; benefits from intraarticular corticosteroids appear short-lived in
the range of 2–4 weeks (Ravaud et al. 1999;
Smith et al. 2003). In at least one study, no interaction between steroid injection and joint lavage
was found (Ravaud et al. 1999), suggesting that
joint lavage may have a different and more
persistent mechanism of action than the injection of corticosteroids. The effects of these two
treatments have also been found to be additive
(Ravaud et al. 1999).
In more recent studies, arthroscopic partial
meniscectomy was compared with diagnostic
arthroscopy (sham surgery) for patients with
a degenerate meniscal tear. Outcomes after
arthroscopic partial meniscectomy were no
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
185
Surgical Treatment
Cartilage
(A) 6
Control group
*
Histologic scale
Treatment group
*
4
better than those after sham surgery (Sihvonen et al. 2013), suggesting that joint lavage
may have a role in the relief of pain in selected
patients.
*
2
0
Mechanism for relief of joint pain
Lavage at Week 1 Lavage at Week 2 Lavage at Week 3
Synovium
(B) 4
Histologic scale
VetBooks.ir
186
Control group
Treatment group
3
*
*
2
*
1
0
Lavage at Week 1 Lavage at Week 2 Lavage at Week 3
Figure 24.1 Histologic grading of femoral condyle
cartilage and synovium from stifles with osteoarthritis in a
rabbit model of bilateral medial meniscectomy with
medial collateral transection (n = 10 animals per time
period). Bilateral joint lavage with saline was performed
in 5 rabbits, with the remaining animals acting as
controls. Joint lavage was performed at 1, 2, and 3 weeks
after meniscectomy and euthanasia performed 1 week
after lavage. (A) Histologic grading of cartilage. (B)
Histologic grading of synovium. ∗ P < 0.05 versus control
group, which received no lavage treatment. Source: Fu
et al. 2009. Reproduced with permission from John Wiley
& Sons, Inc.
Few experimental data are available to provide insight into the mechanism by which joint
lavage might induce relief from joint pain.
However, in an experimental study using a
rabbit meniscectomy model, joint lavage was
found to significantly reduce joint degeneration at 1 to 3 weeks after induction of joint
instability (Fu et al. 2009). Synovial inflammation and degradation of articular cartilage
were both significantly reduced (Figure 24.1
and Table 24.1) (Fu et al. 2009). Joint lavage treatment also led to reduced expression of the proinflammatory cytokines interleukin-1β (IL-1β)
and tumor necrosis factor-alpha (TNF-α) in synovial fluid (Fu et al. 2009).
Conclusions
Collectively, these clinical trial and experimental findings suggest that joint lavage may have
efficacy in the treatment of arthritis, particularly
through reduction of joint inflammation. Metaanalysis of data from randomized, controlled
Table 24.1 Influence of joint lavage on inflammatory markers in synovial fluid in a rabbit meniscectomy and medial
collateral transection model.
Period after meniscectomy before joint lavage
Marker
1 week (n = 10)
2 weeks (n = 10)
3 weeks (n = 10)
IL-1β (pg ml–1 )
Control (n = 5/time point)
81.35 ± 2.41
67.39 ± 2.95
53.86 ± 3.79
Saline lavage (n = 5/time point)
35.79 ± 3.50∗
39.85 ± 4.78∗
29.94 ± 3.99∗
761.97 ± 17.28
446.32 ± 26.83
TNF-α (pg ml–1 )
Control (n = 5/time point)
Saline lavage (n = 5/time point)
599.36 ± 25.40
313.02 ±
24.61∗
459.15 ±
18.15∗
309.88 ± 27.69∗
Note: Euthanasia was performed at 1 week after lavage. IL-1β and TNF-α concentrations were determined using ELISA.
∗ P < 0.05 versus control group.
Reproduced from Fu et al. (2009), with permission from Wiley Blackwell.
IL-1β, interleukin-1β; TNF-α, tumor necrosis factor-alpha.
VetBooks.ir
Joint Lavage
studies investigating joint lavage for human
knee osteoarthritis suggests that at 3 months,
joint lavage alone does not provide significant
improvement in pain and function (Arouac et al.
2010). Since 2007, arthroscopic lavage in human
knee osteoarthritis patients has been a procedure in decline (Lazic et al. 2014).
In conclusion, when designing clinical trials using arthroscopy for the treatment of
dogs with stifle arthritis and cruciate ligament rupture, the possibility that a significant
treatment effect from arthroscopic lavage may
exist should be considered in the experimental design of the trial study, although any treatment effect may be small based on human knee
osteoarthritis studies. Further work is needed to
more comprehensively understand the mechanistic effects of joint lavage on arthritic canine
joints, particularly as any treatment effect
from joint lavage appears much more durable,
when compared to intra-articular corticosteroid
treatment.
References
Arouac J, Vicaut E, Bardin T, et al. Efficacy of
joint lavage in knee osteoarthritis: meta-analysis
of randomized controlled studies. Rheumatology
2010;49:334–340.
187
Bradley JD, Heilman DK, Katz BP, et al. Tidal irrigation as treatment for knee osteoarthritis. A shamcontrolled, randomized, double-blinded evaluation. Arthritis Rheum 2002;46:100–108.
Burman MS, Finkelstein H, Mayer L. Arthroscopy of
the knee joint. J Bone Joint Surg 1934;16:255–268.
Fu X, Lin L, Zhang J, et al. Assessment of the efficacy
of joint lavage in rabbits with osteoarthritis of the
knee. J Orthop Res 2009;27:91–96.
Habib GS. Systemic effects of intra-articular corticosteroids. Clin Rheumatol 2009;28:749–756.
Jüni P, Reichenbach S, Trelle S, et al. Efficacy and
safety of intraarticular hylan or hyaluronic acids
for osteoarthritis of the knee. Arthritis Rheum
2007;56:3610–3619.
Lazic S, Boughton O, Hing C, et al. Arthroscopic
washout of the knee: A procedure in decline. Knee
2014;21:631–634.
Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med 2002;347:81–88.
Ravaud P, Moulinier L, Giraudeau B, et al. Effects
of joint lavage and steroid injection in patients
with osteoarthritis of the knee. Arthritis Rheum
1999;42:475–482.
Smith MD, Wetherall M, Darby T, et al. A randomized placebo-controlled trial of arthroscopic lavage
versus lavage plus intra-articular corticosteroids in
the management of symptomatic osteoarthritis of
the knee. Rheumatology 2003;42:1477–1485.
Sihvonen R, Paavola M, Malmivaara A, et al. Arthroscopic partial meniscectomy versus sham surgery
for a degenerative meniscal tear. N Engl J Med
2013;369:2515–2524.
VetBooks.ir
VetBooks.ir
25
Extracapsular Stabilization
Selena Tinga and Stanley E. Kim
Introduction
Extracapsular stabilization (ES) encompasses
a number of different surgical techniques
designed to stabilize a cranial cruciate ligament
(CrCL)-deficient stifle. Biological or synthetic
materials are placed superficial to the joint capsule, spanning the area lateral and/or medial to
the stifle joint. From the original extracapsular
repair introduced during the 1960s to the current modifications of the technique, the general
theoretical goal is to counteract the translational
and rotational instability that is present when
the CrCL is damaged. The possible advantages
of ES over other stifle stabilization procedures
include the safety of the procedure, the potential for reduction of abnormal internal rotation,
lower technical difficulty, minimal required
inventory, and lower cost. The reported disadvantages include abnormal biomechanics such
as excessive constraint, higher infection rate,
and poorer long-term stability.
Case selection
As with any surgical treatment, correct case
selection is important for optimizing success
rates. Increased body weight has been associated with an increased risk of postoperative complications after ES (Casale & McCarthy
2009). Therefore, body weight and body condition score should be taken into account when
considering surgical options for dogs with cruciate ligament rupture (CR). Younger age has
also been associated with an increased risk
of complications after ES (Casale & McCarthy
2009), and while the cause of this was not speculated, it is assumed that it may be related to
a higher activity level. ES is likely at high risk
of failure in dogs with a steeper tibial plateau
angle (TPA). However, the TPA did not influence outcome (forceplate measures, osteoarthritis progression, and orthopaedic examination
findings) at 48 weeks after surgery in 34 dogs
with TPAs ranging from 19◦ to 35◦ (Havig et al.
2007), though it is notable that dogs with TPAs
over 35◦ were not included.
General surgical approach
Before definitive stifle stabilization, intraarticular inspection should be performed using
stifle arthroscopy or arthrotomy. Joint assessment is recommended to confirm the diagnosis
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
189
VetBooks.ir
190
Surgical Treatment
of CR and to assess the health of the meniscus,
the cranial and caudal cruciate ligaments, and
cartilage surfaces. Medial meniscal tears should
be debrided, or medial meniscal release may be
considered to decrease the risk of late meniscal
tears (see Chapters 35 and 36). An approach to
the lateral distal femur and proximal tibia is
then completed, including incising the fascia
lata and reflecting the biceps femoris caudally.
The stabilizing material is then placed in the
plane between the joint capsule and fascia
lata. Before closure, the stability and range of
motion of the joint should be tested to ensure
appropriate stability has been obtained while
maintaining adequate range of motion.
General care after surgery
Initially, animals should be kept kenneled at
all times with periodic sling walks for elimination purposes only. Starting at 2–3 weeks after
surgery, focused, controlled rehabilitation activity can be initiated and should promote a recovery of function after ES procedures (Marsolais
et al. 2002). Rehabilitation during the postoperative period is discussed in Chapter 42. Activity
restriction is maintained for 12–16 weeks after
surgery to prevent over-stressing the stabilizing structure. This is particularly important for
those ES procedures that depend on the formation of implant-stimulated periarticular fibrosis
for long-term success. Weight reduction should
also be prescribed if appropriate.
Biological extracapsular stabilization
ES was first performed using biological materials; multiple techniques have been described.
First introduced during the 1960s, fascial imbrication techniques rely solely on tightening the
soft tissues lateral and medial to the joint to prevent cranial tibial subluxation (McCurnin et al.
1971; Pearson et al. 1971). A second technique
uses a local strip of fascia lata that extends from
the tibial tuberosity and is threaded around
the fabella (Aiken et al. 1992) in an orientation
that approximately mimics the trajectory of the
native CrCL to limit cranial tibial subluxation
and internal tibial rotation. A third technique,
fibular head transposition, was introduced in
1985 (Smith & Torg 1985). By advancing the
fibular head cranially, the lateral collateral ligament is oriented in an oblique direction similar
to the native CrCL, limiting both cranial tibial
subluxation and internal tibial rotation (Smith
& Torg 1985; Mullen & Matthiesen 1989). Several studies using subjective outcome measures
have reported reasonable success rates for these
techniques (McCurnin et al. 1971; Pearson et al.
1971; Smith & Torg 1985; Mullen & Matthiesen
1989; Aiken et al. 1992). Generally, the most common complications associated with biological
ES techniques in clinical cases are recurrent or
persistent clinical lameness and/or stifle instability, occurring in one-fourth to one-third of
cases in most reports (McCurnin et al. 1971;
Pearson et al. 1971; Mullen & Matthiesen 1989;
Aiken et al. 1992; Chauvet et al. 1996). Recurrent
stifle instability likely results from stretching of
the surgically repositioned soft tissues that are
providing stability in the immediate postoperative period (Dupuis et al. 1994). Fibular head
transposition has additional potential complications including fibular head fracture and softtissue irritation, seroma, or infection associated
with the required metal implants (Smith & Torg
1985; Mullen & Matthiesen 1989). These biological ES techniques are now rarely used due to
unacceptably low success rates and high complication rates, although fascial imbrication is
often combined with other primary stifle stabilization procedures for augmentation.
Extracapsular stabilization with
synthetic materials
The use of synthetic materials is now more common than biological techniques for ES (Korvick
et al. 1994). Most commonly, a pliable linear
implant (‘suture’) is passed from the caudodistal femur to the cranioproximal tibia across
the lateral aspect of the joint, between the fascia lata and the joint capsule. A variety of
types of ES using synthetic materials have been
described, including the lateral fabello-tibial
suture (Figure 25.1), TightRope CCL® (Arthrex
Vet Systems, Naples, FL, USA) (Figure 25.2),
various bone anchor techniques (Figure 25.3),
and the Ruby Joint Stabilization System (Kyon
Veterinary Surgical Products, Boston, MA)
(Figure 25.4).
191
VetBooks.ir
Extracapsular Stabilization
Figure 25.1 Cranial and lateral illustrations of a stifle with a lateral fabello-tibial suture technique. Note that a small
portion of the ‘extra-articular’ suture is within the joint. Source: Tonks et al. 2011. Reproduced with permission from
Schattauer.
(A)
(B)
(C)
Figure 25.2 Medial (A), cranial (B), and lateral (C) illustrations of a stifle with the Tightrope CCL® technique. Source:
Tonks et al. 2011. Reproduced with permission from Schattauer.
Surgical Treatment
VetBooks.ir
192
(A)
(B)
Figure 25.3 Cranial (A) and lateral (B) illustrations of a stifle with a femoral bone anchor technique. Source: Tonks et al.
2011. Reproduced with permission from Schattauer.
The lateral fabello-tibial suture (LFTS) technique is based on Flo’s modification of the procedure described by DeAngelis and Lau (DeAngelis & Lau 1970; Flo 1975). A monofilament
nylon leader line is passed from proximal to distal around the lateral fabella. Single or double
tibial bone tunnels for suture passage have been
described. The suture should be tunneled under
the cranial tibial muscle rather than coursing
over the muscle. The final suture pattern can
be a box or a figure-of-eight configuration. The
suture is fastened with knots or crimp clamps
near the lateral fabella. The medial and lateral retinacular imbrication technique (MRIT) is
similar to the LFTS except that a medial fabellotibial suture is also placed.
The TightRope CCL® (TR) is a procedure
in which a multifilament suture (FiberTape® )
is passed through femoral and tibial bicortical
bone tunnels and secured on the medial side of
each bone using endobuttons. The femoral exit
site is 2 mm from the caudal edge of the lateral femoral condyle at the level of the distal
fabella, and the tibial exit site is located at the
caudal aspect of the extensor groove; the tunnels diverge away from the stifle joint.
Multiple bone anchor systems have been
described for ES, where the anchors are used
to secure the suture at the femoral and/or tibial attachment sites (Figures 25.3 and 25.4),
and a bone anchor at one site can be combined with a button or bone tunnel at the
other site. Typically, multifilament sutures are
used because the pliability of multifilament
may be beneficial for use with bone anchors.
The suture ends are typically joined using
a knot. Anchor sites are chosen by the surgeon but should be based on isometry (see
below). Examples of bone anchor products that
have been used for ES include FASTak® and
SwiveLock® . FASTak® anchors are pre-loaded
with FiberWire® , whereas SwiveLock® anchors
can be threaded with a suture of the surgeon’s
preference.
The Ruby Joint Stabilization System is a
bone anchor system with multiple added innovations. The Ruby system uses two titanium
alloy bone anchors with ceramic eyelets to
secure a multifilament continuous-loop suture
(Dyneema® ) to the bone. One loop of suture
is associated with the femoral anchor and one
loop with the tibial anchor, and the two loops
are joined using a titanium link; the length of
the Dyneema® loops must be pre-determined,
but no knot or crimp is required. The ultralow-friction Ruby eyelet embedded in the bone
193
VetBooks.ir
Extracapsular Stabilization
(A)
(B)
Figure 25.4 The Ruby Joint Stabilization System represented in a bone model (A) and a lateral projection stifle
radiograph of a clinical case (B). Source: Images courtesy of Dr. Otto Lanz.
anchors is purported to minimize wear on the
Dyneema® fibers.
Suture material
As discussed, the suture material can be either a
monofilament or a multifilament line. Monofilaments may have lower infection rates (Korvick et al. 1994), while multifilaments tend to
be superior in strength and stiffness, and have
a greater resistance to elongation (Burgess et al.
2010; Rose et al. 2012). Nylon leader line is the
most commonly used monofilament suture; it
is mechanically superior to nylon fishing line
(Caporn & Roe 1996; Nwadike & Roe 1998) and
also to smaller-diameter polypropylene suture
(Lewis et al. 1997). Nylon leader line is available in 20–80 pound test strengths; the test
strength of the material should approximate the
weight of the animal (Piermattei et al. 2006;
Kowaleski et al. 2012), and one or two strands
can be placed. When two strands are desired,
many surgeons use two individual lengths tied
individually, but it has been suggested that a
single continuous length of suture overcomes
the inevitable uneven tension on individual
strands, which may lead to earlier failure (Wallace et al. 2008). Some studies have shown a
weakening of the leader line after steam sterilization (Lewis et al. 1997) or ethylene oxide
sterilization (Anderson et al. 1998), while others have shown no difference in mechanical
properties after sterilization (Caporn & Roe
1996; Sicard et al. 2002). Generally, it is recommended to minimize the number of sterilization
cycles where possible, particularly with steam
sterilization.
Many different multifilament products are
available for extracapsular suture stabilization,
which can be composed of polyethylene (e.g.,
Dyneema® ), polyester, polybutester, Kevlar,
or a combination of materials. FiberWire® is
a cylindrical multifilament composed of a
core of multiple strands of high molecular
weight polyethylene surrounded by a braided
polyester jacket, while FiberTape® is a 2 mmwide tape with a similar material make-up
to FiberWire® . Early in the development of
LFTS, orthopaedic wire was used but radiographs revealed wire breakage in 26 of 33
cases (79%) by 6 weeks postoperatively (Störk
et al. 2001); consequently, use of wire is not
recommended.
VetBooks.ir
194
Surgical Treatment
Isometry
Isometry refers to maintaining the same distance between the attachment sites of the stabilizing suture over a range of motion, and is
a critical concept for ES as well as other types
of CrCL repair. The femoral and tibial suture
attachment sites should be as isometric as possible in order to minimize the impact on stifle range of flexion–extension motion and minimize stress on the suture and soft tissue or
bone attachments (Figure 25.5). Suture attachment sites at the lateral caudodistal femur and
the lateral cranioproximal tibia should create
a suture trajectory that roughly mimics that of
the CrCL in the sagittal plane. Theoretically, the
use of isometric points should maximize the
functional life span of the implant. However,
due to the complex shapes and motions of
the dog’s stifle joint, perfect isometry is not
achievable with extra-articular attachment sites
(Arnoczky et al. 1977; Fischer et al. 2010; Hulse
et al. 2010).
Numerous studies have attempted to determine the optimal tibial and femoral ES attachment points based on isometry, but resultant
recommendations vary widely (Roe et al. 2008;
Fischer et al. 2010; Hulse et al. 2010; Witte
2015). In two studies, measures of isometry
were based on the distance between the proposed suture attachment sites on radiographs
as the limb was moved through a range of
flexion–extension motion (Roe et al. 2008; Witte
2015). Unsurprisingly, isometry was not achievable, but the most isometric points were determined to be: (i) caudolaterally on the femur
at the level of the distal aspect of the lateral
fabella; and (ii) cranial and proximal on the
tibia between the tibial tuberosity and the extensor groove (Roe et al. 2008; Witte 2015). Small
changes in the femoral attachment site had a
greater effect on distance between attachment
points than small changes in the tibial attachment site (Roe et al. 2008). Two ex vivo studies have been performed where suture tension
was tested throughout a range of flexion–
extension motion, where smaller changes in
suture tension were interpreted as a higher
degree of isometry. In one study, a circumfabellar suture was recommended that then passed
through two bone tunnels just caudal to the tibial tuberosity (Fischer et al. 2010), while a second ex vivo study recommended anchoring the
suture in the femoral condyle at the level of
the distal aspect of the lateral fabella and in the
bony prominence of the tibia just caudal to the
extensor groove at the level of the tibial plateau
(Hulse et al. 2010). Due to variations of conformation, the most isometric points are likely
variable between breeds and individuals within
a breed (Witte 2015).
Methods of securing the suture to the
femur and tibia
Figure 25.5 Anatomic illustration showing points that
are most isometric on the lateral aspect of the canine
stifle, according to Hulse et al. (2010). Copyright ©
Samantha J. Elmhurst at www.livingart.org.uk.
The suture can be secured at the femoral and tibial attachment sites in various ways. At either
site, the suture can be anchored to the bone
VetBooks.ir
Extracapsular Stabilization
either by passing it through a full-thickness
bone tunnel and then through a button medially
that lags up against the bone, or using a bone
anchor. The femoral portion of the suture can
also be anchored by passing it around the proximal fabella (fabellofemoral ligament). The tibial
portion of the suture can also be anchored by
passing the suture from lateral to medial under
the patellar tendon and then back through a
bone tunnel or medially then laterally through
two bone tunnels. Few studies have been conducted to compare the various forms of anchoring, but one ex vivo study showed that the TR
procedure, which uses full thickness bone tunnels anchored medially with buttons, provided
more resistance to cranial tibial displacement
than did LFTS (Choate et al. 2013).
Methods of securing suture ends
The method of securing the suture can affect the
strength of the construct. In general, monofilament sutures can be joined using one or multiple knots and/or crimp clamps. When tying a
monofilament suture with square knots, more
throws will increase knot security (Caporn &
Roe 1996) but also increases the profile of the
knot, which can cause tissue irritation and
necrosis of the overlying skin. Four to five total
throws are typically used, starting with a square
knot (rather than a surgeon’s knot). In order
to avoid losing suture tension during the first
knot, a hemostat is often used to grasp the first
throw while throwing the second.
Metal crimp clamps negate the need for a
bulky knot and allow the use of a tensioning
device which holds the suture taut while crimping the clamp, facilitating placement of a tight
suture without assistance. The success of crimp
clamp fixation is equal to or better than knots in
most studies (Anderson et al. 1998; Peycke et al.
2002; Banwell et al. 2005; Vianna & Roe 2006),
but using crimp clamps weakens the suture at
the crimp site (Sicard et al. 2002) and slippage
of the suture through the clamp is also a concern (Burgess et al. 2010). If crimp clamps are
used, it has been suggested that more than one
crimp clamp should be placed to lessen the risk
of slippage (McCartney et al. 2007), and that a
crimping system which creates multiple crimps
is used (Maritato et al. 2012).
195
The strongest combination of monofilament
loop configuration and securing method is not
known. In a biomechanical study comparing
various double-loop suture configurations that
were secured using crimp clamps, the singlestrand, double-loop configuration using an
interlocking knot along with a crimp clamp was
mechanically superior to five other configurations (Wallace et al. 2008), while a different study
found this construct to be inferior to all tested
constructs, with the strongest construct being a
single-strand, double-loop secured purely with
crimp clamps, but no double-loop, doublestrand constructs were tested (Aisa et al. 2015).
Another ex vivo study comparing various knots
to crimp clamps found that single-strand constructs secured with crimp clamps were as good
or better than single-strand constructs secured
with knots, but a double-loop construct secured
with a self-locking knot was superior to all
single-strand constructs (Peycke et al. 2002).
Multifilament sutures can also be joined
using one or multiple knots or crimp clamps.
Knot security between types of multifilament
sutures is variable (Burgess et al. 2010) due to
differences in base material and suture coating.
Multifilament sutures may have an increased
incidence of slippage through a crimp clamp
(Burgess et al. 2010; Maritato et al. 2012) and,
therefore, knots are commonly used. The knot
profile is lower when knotting a multifilament
compared to a monofilament.
Stifle position while securing suture
As the suture is secured, cranial tibial subluxation and internal tibial rotation should be
reduced. The recommended degree of applied
suture tension is controversial. The surgeon
should be cognizant of over-tightening as this
can limit normal range of motion and increase
the contact pressure on the joint surfaces (Tonks
et al. 2010). Under-tightening can predispose
to inadequate stabilization and premature loosening. In order to mitigate under- and overtightening, one author recommends that the stifle should be placed in approximately 100◦ of
flexion when securing the suture (Fischer et al.
2010), while the TR protocol has the stifle placed
at 140◦ when tying the suture. It has been suggested that the ideal angle for tightening the
VetBooks.ir
196
Surgical Treatment
ES suture may be different for individual dogs,
depending on conformation (Witte 2015).
Clinical outcome
Extracapsular stabilization techniques generally have good outcomes, particularly subjectively. The most common major complications
associated with ES procedures are postoperative meniscal tear, failure of the stabilization, and implant-associated infection (Dulisch
1981; Korvick et al. 1994; Chauvet et al. 1996;
Conzemius et al. 2005; Guénégo et al. 2007;
Casale & McCarthy 2009; Ertelt & Fehr 2009;
Cook et al. 2010; Christopher et al. 2013).
After LFTS, owners are reportedly satisfied
with outcomes in 82–90% of cases (Moore &
Read 1995; Chauvet et al. 2009). Minimal to
no lameness was reported in 78–82% by 6–20
months’ follow up in most studies (Moore &
Read 1995; Chauvet et al. 1996; Ertelt & Fehr
2009), although one study reported only 40%
clinical improvement by 6 months (Conzemius
et al. 2005). On palpation examination, 55–76%
of dogs had no drawer palpable at 6–20 months
after surgery (Moore & Read 1995; Chauvet et al.
1996; Ertelt & Fehr 2009), and 73% had no pain
on stifle manipulation at 20 months postoperatively in the 11 dogs that returned for follow-up
(Moore & Read 1995).
Force plate examination is a more objective measure of outcome, and has been used
in multiple studies of clinical outcome after
LFTS and has shown less satisfactory results
than the previously discussed subjective outcome measures. One study reported that only
15% of dogs achieved normal ground reaction
forces within 6 months (Conzemius et al. 2005),
another reported that 86% returned to normal
by 20 months after surgery (Chauvet et al. 1996),
while a third study reported that dogs treated
with LFTS remained significantly different from
normal throughout the study period of one year
(Nelson et al. 2013).
The most recent evidence has shown tibial osteotomy procedures, particularly the tibial plateau leveling osteotomy, to have superior outcomes when compared to ES (Lazar
et al. 2005; Gordon-Evans et al. 2013; Nelson et al. 2013; Bergh et al. 2014), though
there are also studies showing no difference in
outcome between ES and osteotomy procedures
(Conzemius et al. 2005; Au et al. 2010; Cook et al.
2010; Mölsä et al. 2013).
Major postoperative complications reportedly occur in 7–17% of LFTS cases and include
implant infection, swelling or irritation associated with the implant, implant failure, tearing of
the fabellofemoral ligament, meniscal tear, failure to control stability, and peroneal nerve damage (Dulisch 1971; Casale & McCarthy 2009;
Ertelt & Fehr 2009; Au et al. 2010). In one
study, the risk of development of complications
after LFTS was increased in dogs that were
male, had a higher body weight, or were of
younger age (Casale & McCarthy 2009). When
multifilament suture is used for LFTS, the risk
of fabellofemoral ligament failure is increased
(Lodato et al. 2013), as is the risk of infection (Korvick et al. 1994). The risk of infection
when using multifilament suture may be further increased with decreased surgeon experience (Dulisch 1981).
Literature reporting clinical outcomes for
techniques other than the LFTS is sparse. In
the largest study of long-term outcome after
clinical cases of CR treated with TR, owners
reported a return to full function in 76% of
dogs (60/79) and a return to acceptable function in 23% (18/79), with 44% (35/79) still
experiencing some degree of pain (Christopher
et al. 2013). Major complications occurred in
8.9% of stifles (7/79), with the primary major
complication being postoperative meniscal tear
(6.3%; 5/79). Other major complications were
not detailed (Christopher et al. 2013). In another
clinical study, 92% of dogs (48/52) had a successful outcome more than one year after TR
surgery based on follow-up via phone conversation (Ritzo et al. 2014). The outcome was more
likely to be successful if a concurrent meniscal
tear was diagnosed and treated at the time of
initial surgery (Ritzo et al. 2014).
Owner assessment of outcome after ES using
bone anchors is also good, with 92–100% owner
satisfaction at 10–18 months after surgery
(Guénégo et al. 2007; Hulse et al. 2011). At
18 months’ follow-up, one study reported that
lameness had been resolved in 91% (44/48) of
dogs (Guénégo et al. 2007). Despite good subjective outcome, radiographs revealed that the
bone anchors had pulled out of the femur in
21% of dogs (10/48) in this study (Guénégo
VetBooks.ir
Extracapsular Stabilization
et al. 2007). These were large and giant breed
dogs, and pull-out was found to be more likely
if the anchor was placed in the less isometric mid-condylar region rather than the caudal
femoral condyle (Guénégo et al. 2007), which is
likely due to the difference in direction of pull
(Burkhart 1995; Balara et al. 2004) and/or isometry. No clinical studies have been published
using the Ruby stifle stabilization system.
Conclusions
A large in vivo clinical study comparing the
long-term outcome of each ES technique has
not been performed and, therefore, the superior method of ES has not been determined. ES
techniques are generally safe for the surgical
treatment of CR in dogs. Given the major benefits of ES over osteotomy techniques, such as
lower costs, lower technical difficulty, and minimal requirement for specialized equipment, it
is likely that ES methods will remain a popular treatment option for CR in the foreseeable
future.
References
Aiken SW, Bauer MS, Toombs JP. Extra-articular fascial strip repair of the cranial cruciate deficient stifle: Technique and results in seven dogs. Vet Comp
Orthop Traumatol 1992;5:145–150.
Aisa J, Calvo I, Buckley CT, et al. Mechanical comparison of loop and crimp configurations for extracapsular stabilization of the cranial cruciate ligamentdeficient stifle. Vet Surg 2015;44:50–58.
Anderson CC, Tomlinson JL, Daly WR, et al. Biomechanical evaluation of a crimp clamp system for
loop fixation of monofilament nylon leader material used for stabilization of the canine stifle joint.
Vet Surg 1998;27:533–539.
Arnoczky SP, Torzilli PA, Marshall JL. Biomechanical
evaluation of anterior cruciate ligament repair in
the dog: An analysis of the instant center of motion.
J Am Anim Hosp Assoc 1977;13:553–558.
Au KK, Gordon-Evans WJ, Dunning D, et al. Comparison of short- and long-term function and radiographic osteoarthritis in dogs after post-operative
physical rehabilitation and tibial plateau leveling
osteotomy or lateral fabellar suture stabilization.
Vet Surg 2010;39:173–180.
Balara JM, McCarthy RJ, Boudrieau RJ, et al. Mechanical performance of a screw-type veterinary suture
anchor subjected to single load to failure and cyclic
loads. Vet Surg 2004;33:615–619.
197
Banwell MN, Kerwin SC, Hosgood G, et al. In vitro
evaluation of the 18 and 36 kg Securos cranial cruciate ligament repair system. Vet Surg 2005;34:283–
288.
Bergh MS, Sullivan C, Ferrel CL, et al. Systematic
review of surgical treatments for cranial cruciate
ligament disease in dogs. J Am Anim Hosp Assoc
2014;50:315–321.
Burgess R, Elder S, McLaughlin R, et al. In vitro
biomechanical evaluation and comparison of FiberWire, FiberTape, OrthoFiber, and nylon leader line
for potential use during extraarticular stabilization of canine cruciate deficient stifles. Vet Surg
2010;39:208–215.
Burkhart SS. The deadman theory of suture anchors:
Observations along a south Texas fence line.
Arthroscopy 1995;11:119–123.
Caporn TM, Roe SC. Biomechanical evaluation of
the suitability of monofilament nylon fishing and
leader line for extra-articular stabilisation of the
canine cruciate-deficient stifle. Vet Comp Orthop
Traumatol 1996;9:126–133.
Casale SA, McCarthy RJ. Complications associated
with lateral fabellotibial suture surgery for cranial
cruciate ligament injury in dogs: 363 cases (1997–
2005). J Am Vet Med Assoc 2009;234:229–235.
Chauvet AE, Johnson AL, Pijanowski GJ, et al. Evaluation of fibular head transposition, lateral fabellar
suture, and conservative treatment of cranial cruciate ligament rupture in large dogs: a retrospective
study. J Am Anim Hosp Assoc 1996;32:247–255.
Choate CJ, Lewis DD, Conrad BP, et al. Assessment
of the craniocaudal stability of four extracapsular
stabilization techniques during two cyclic loading
protocols: A cadaver study. Vet Surg 2013;42:853–
859.
Christopher SA, Beetem J, Cook JL. Comparison of
long-term outcomes associated with three surgical
techniques for treatment of cranial cruciate ligament disease in dogs. Vet Surg 2013;42:329–334.
Conzemius MG, Evans RB, Besancon MF, et al. Effect
of surgical technique on limb function after surgery
for rupture of the cranial cruciate ligament in dogs.
J Am Vet Med Assoc 2005;226:232–236.
Cook JL, Luther JK, Beetem J, et al. Clinical comparison of a novel extracapsular stabilization procedure and tibial plateau leveling osteotomy for
treatment of cranial cruciate ligament deficiency in
dogs. Vet Surg 2010;39:315–323.
DeAngelis M, Lau RE. A lateral retinacular imbrications technique for the surgical correction of anterior cruciate ligament rupture in the dog. J Am Vet
Med Assoc 1970;57:79–84.
Dulisch ML. Suture reaction following extra-articular
stabilization in the dog. Part II: a prospective study
of 66 stifles. J Am Anim Hosp Assoc 1981;17:572–
574.
Dupuis J, Harari J, Blackketter D, et al. Evaluation
of the lateral collateral ligament after fibular head
transposition in dogs. Vet Surg 1994;23:456–465.
VetBooks.ir
198
Surgical Treatment
Ertelt J, Fehr M. Cranial cruciate ligament repair in
dogs with and without meniscal lesions treated by
different minimally invasive methods. Vet Comp
Orthop Traumatol 2009;22:21–26.
Fischer C, Cherres M, Grevel V, et al. Effects of attachment sites and joint angle at the time of lateral
suture fixation on tension in the suture for stabilization of the cranial cruciate ligament deficient stifle
in dogs. Vet Surg 2010;39:334–342.
Flo GL. Modification of the lateral retinacular imbrication technique for stabilizing cruciate ligament
injuries. J Am Anim Hosp Assoc 1975;11:570.
Gordon-Evans WJ, Griffon DJ, Bubb C, et al. Comparison of lateral fabellar suture and tibial plateau leveling osteotomy techniques for treatment of dogs
with cranial cruciate ligament disease. J Am Vet
Med Assoc 2013;243:675–680.
Guénégo L, Zahra A, Madelénat A, et al. Cranial cruciate ligament rupture in large and giant dogs. A
retrospective evaluation of a modified lateral extracapsular stabilization. Vet Comp Orthop Traumatol
2007;20:43–50.
Havig ME, Dyce J, Kowaleski MP, et al. Relationship of tibial plateau slope to limb function in dogs
treated with a lateral suture technique for stabilization of cranial cruciate ligament deficient stifles. Vet
Surg 2007;36:245–251.
Hulse D, Hyman W, Beale B, et al. Determination of
isometric points for placement of a lateral suture in
treatment of the cranial cruciate ligament deficient
stifle. Vet Comp Orthop Traumatol 2010;23:163–
167.
Hulse D, Saunders B, Beale B, et al. Extra-articular
stabilization of the cranial cruciate deficient stifle
with anchor systems. Tierarztliche Praxis Kleintiere
2011;39:363–367.
Kowaleski MP, Boudrieau RJ, Pozzi A. In: Veterinary
Surgery: Small Animal. Stifle Joint. Karen M, Tobias
SAJ, eds. 1st edn. St Louis, MO, Elsevier-Saunders,
2012, pp. 906–998.
Korvick DL, Johnson AL, Schaeffer DJ. Surgeons’
preferences in treating cranial cruciate ligament
ruptures in dogs. J Am Vet Med Assoc 1994;205:
1318–1324.
Lazar TP, Berry CR, de Haan JJ, et al. Long-term
radiographic comparison of tibial plateau leveling osteotomy versus extracapsular stabilization
for cranial cruciate ligament rupture in the dog. Vet
Surg 2005;34:133–141.
Lewis DD, Milthorpe BK, Bellenger CR. Mechanical comparison of materials used for extra-capsular
stabilisation of the stifle joint in dogs. Aust Vet J
1997;75:890–896.
Lodato D, Wardlaw J, Rowe D. Retrospective study
comparing two materials commonly used in the
LFS technique for CCLR. J Am Anim Hosp Assoc
2013;49:108–114.
Maritato KC, Barnhart MD, Kazanovicz AJ, et al. In
vitro mechanical evaluation and comparison of two
crimping devices for securing monofilament nylon
and multifilament polyethylene for use in extracapsular stabilization of the canine stifle. Vet Comp
Orthop Traumatol 2012;25:466–471.
Marsolais GS, Dvorak G, Conzemius MG. Effects of
postoperative rehabilitation on limb function after
cranial cruciate ligament repair in dogs. J Am Vet
Med Assoc 2002;220:1325–1330.
McCartney WT, O’Connor JV, McCann WM. Incidence of infection and premature crimp failure
after repair of cranial cruciate ligament-deficient
stifles in 110 dogs. Vet Rec 2007;161:232–233.
McCurnin DM, Pearson PT, Wass WM. Clinical and
pathologic evaluation of ruptured cranial cruciate ligament repair in the dog. Am J Vet Res
1971;32:1517–1524.
Mölsä SH, Hielm-Björkman AK, Laitinen-Vapaavuori
OM. Use of an owner questionnaire to evaluate
long-term surgical outcome and chronic pain after
cranial cruciate ligament repair in dogs: 253 cases
(2004–2006). J Am Vet Med Assoc 2013;243:689–
695.
Moore KW, Read RA. Cranial cruciate ligament rupture in the dog – A retrospective study comparing surgical techniques. Aust Vet J 1995;72:281–
285.
Mullen HS, Mattheisen DT. Complications of transposition of the fibular head for stabilization of the
cranial cruciate-deficient stifle in dogs: 80 cases
(1982–1986). J Am Vet Med Assoc 1989;195:1267–
1271.
Nelson SA, Krotscheck U, Rawlinson J, et al. Longterm functional outcome of tibial plateau leveling osteotomy versus extracapsular repair in a heterogenous population of dogs. Vet Surg 2013;42:
38–50.
Nwadike BS, Roe SC. Mechanical comparison of
suture material and knot type used for fabello-tibial
sutures. Vet Comp Orthop Traumatol 1998;11:47–
52.
Pearson PT, McCurnin DM, Carter JD, et al. Lembert
suture technique to surgically correct ruptured cruciate ligaments. J Am Anim Hosp Assoc 1971;7:1–
13.
Peycke LE, Kerwin SC, Hosgood G, et al. Mechanical comparison of six loop fixation methods with
monofilament nylon leader line. Vet Comp Orthop
Traumatol 2002;15:210–214.
Piermattei DL, Flo GL, DeCamp CE. Brinker, Piermattei, and Flo’s Handbook of Small Animal Orthopaedics
and Fracture Repair. 4th edn. St Louis, SaundersElsevier, 2006.
Ritzo ME, Ritzo BA, Siddens AD, et al. Incidence and
type of meniscal injury and associated long-term
clinical outcomes in dogs treated surgically for cranial cruciate ligament disease. Vet Surg 2014;43:
952–958.
Roe SC, Kue J, Gemma J. Isometry of potential suture
attachment sites for the cranial cruciate ligament
VetBooks.ir
Extracapsular Stabilization
deficient canine stifle. Vet Comp Orthop Traumatol
2008;21:215–220.
Rose ND, Goerke D, Evans RB, et al. Mechanical testing of orthopaedic suture material used for extraarticular stabilization of canine cruciate ligamentdeficient stifles. Vet Surg 2012;41:266–272.
Sicard GK, Hayashi K, Manley PA. Evaluation of
5 types of fishing material, 2 sterilization methods, and a crimp-clamp system for extra-articular
stabilization of the canine stifle joint. Vet Surg
2002;31:78–84.
Störk CK, Gibson NR, Owen MR, et al. Radiographic
features of a lateral extracapsular wire suture in the
canine cranial cruciate deficient stifle. J Small Anim
Pract 2001;42:487–490.
Smith GK, Torg JS. Fibular head transposition for
repair of cruciate-deficient stifle in the dog. J Am
Vet Med Assoc 1985;187:375–383.
199
Tonks CA, Pozzi A, Ling HY, et al. The effects of
extra-articular suture tension on contact mechanics of the lateral compartment of cadaveric stifles
treated with the TightRope CCL or lateral suture
technique. Vet Surg 2010;39:343–349.
Vianna ML, Roe SC. Mechanical comparison of two
knots and two crimp systems for securing nylon
leader line used for extra-articular stabilization of
the canine stifle. Vet Surg 2006;35:567–572.
Wallace AM, Cutting ED, Sutcliffe MP, et al. A
biomechanical comparison of six different double
loop configurations for use in the lateral fabella
suture technique. Vet Comp Orthop Traumatol
2008;21:391–399.
Witte PG. Tibial anatomy in normal small breed dogs
including anisometry of various extracapsular stabilizing suture attachment sites. Vet Comp Orthop
Traumatol 2015;28:331–338.
VetBooks.ir
VetBooks.ir
26
Intra-Articular Repair for
Cranial Cruciate Ligament
Rupture in the Dog
Jeffery J. Biskup and Michael G. Conzemius
Introduction
Cruciate ligament rupture (CR) is one of the
most common orthopaedic conditions seen in
small animal medicine, but an ideal repair has
not yet been elucidated (Johnson et al. 1994;
Bellumori et al. 2013; Krotscheck et al. 2016).
Although successful treatment of CR has been
achieved both medically and surgically, recent
evidence suggests that outcomes are optimized
in dogs after surgical treatment (Wucherer
et al. 2013). This chapter first identifies some
potential limitations of commonly used surgical procedures for CR, briefly explores the
historic use of intra-articular repair in dogs,
and then focuses on overcoming the identified limitations of both extra- and intra-articular
repairs. Specifically, the limitations addressed
will include graft selection, graft fixation, and
graft biology.
Current cruciate ligament rupture
surgical treatment outcomes
Surgery for CR has been shown to greatly
improve lameness but may not consistently
get patients back to normal (Mölsä et al.
2013; Wucherer et al. 2013). Current tibial
osteotomy stabilization methods have high success rates at early and mid-range follow-up
times, but outcome measures are often subjective, such as non-validated owner questionnaires (Hoffman et al. 2006; Corr & Brown 2007;
Stein & Schmoekel 2008) and veterinarians’
visual assessment (Waxman et al. 2008). More
objective outcomes, such as force platform analysis, pressure platform analysis, radiographic
scoring and thigh circumference have been
used as more sensitive ways to assess lameness after surgical treatment of CR (Jevens
et al. 1996; Conzemius et al. 2005). With more
objective measurements, outcomes with tibial
osteotomies in certain studies have shown that
operated limbs do not obtain the same function
as normal limbs (Evans et al. 2005; Voss et al.
2008).
A final challenge when interpreting CR surgical outcome studies is that standardized definitions of success and follow-up time have not
been agreed upon, and this makes the comparison of studies difficult. For example, one
study used a stringent definition of success
that combined both subjective and objective
outcomes, comparing medical management
to tibial plateau leveling osteotomy (TPLO)
(Wucherer et al. 2013). That study revealed a
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
201
VetBooks.ir
202
Surgical Treatment
success rate of only 75% at one year after
TPLO treatment. Although outcomes seem to be
optimal for current procedures in many studies,
the limitations mentioned above and the progression of more sensitive outcome measures
may change the interpretations of results.
One consistent finding between many studies is that most dogs will still have progressive osteoarthritis (OA) after surgical treatment,
affecting long-term success (Elkins et al. 1991;
Innes & Barr 1998; Lazar et al. 2005). Furthermore, although the severity of OA has not
been shown to be correlated with lameness,
dogs with OA have a greater chance of lameness compared to a dog with a normal stifle
(Gordon et al. 2003). It is hypothesized that progressive OA develops because the most commonly performed techniques do not replace all
mechanical properties of an intact cranial cruciate ligament (CrCL) (Kim et al. 2012; Skinner et al. 2013; Biskup et al. 2014a). The CrCL
is known to prevent cranial translation, internal rotation, and hyperextension of the tibia
(Heffron & Campbell 1978).
An in-depth discussion of all current repair
options is beyond the scope of this chapter,
but main concepts will be briefly discussed.
First, extra-articular sutures lack the material
strength to eliminate drawer (Cabano et al. 2011;
Rose et al. 2012; Biskup et al. 2014a), and the
anchor points are not likely to be isometric
(Roe et al. 2008; Fischer et al. 2010; Hulse et al.
2010b). The results of some studies that incorporated objective outcomes also suggest that
suture repairs are inferior to tibial osteotomies
(Gordon-Evans et al. 2013; Krotscheck et al.
2016). Similarly, tibial osteotomies have a
limited ability to prevent internal rotation,
and femoral-tibial subluxation is inconsistently
eliminated (Kim et al. 2012; Skinner et al. 2013).
Continued instability after these repairs likely
contributes to a higher rate of latent meniscal
tears and progressive OA that is demonstrated
when follow-up is extended to a year or longer
(Bennett et al. 1988; Elkins et al. 1991; Rayward
et al. 2004; Kowaleski et al. 2005; Stauffer et al.
2006). Thus, is it not surprising that the veterinary surgical community has not agreed upon
the ideal surgical treatment for CR.
The ‘gold standard’ in humans for anterior
cruciate ligament (ACL) rupture repair is intraarticular placement of a graft at the attachment sites of the ACL. Currently, there is no
consensus on the ideal graft, nor on the method
of fixation (Murray 2009). ACL graft repairs in
human patients have a reoperation rate of 3–5%,
and <20% of patients develop progressive OA
(Harilainen & Sandelin 2009). In contrast, up to
30% of dogs have postoperative meniscal injury
with complete CR, and close to 100% have progressive OA at 2 years after treatment (Lazar
et al. 2005; Hulse et al. 2010a; DeLuke et al. 2012).
Differences in pathophysiology, function, and
the ability of human patients to assess their own
outcome may explain some of these differences,
although a fivefold difference in treatment failures might suggest that the anatomic reconstruction procedures performed in people are
superior to the non-anatomic procedures commonly used in dogs.
Historical use of intra-articular repairs
Although the ACL was first mentioned in
records dated from 3000 BC, its complex
anatomy was first described by Claudis Galen
between 300 and 400 BC. Although many repair
methods were attempted, the first modern case
series reporting an intra-articular repair was
reported by Hey Groves in 1917 (Davarinos
et al. 2014). Groves described a fascia lata strip
placed through the joint and anchored in a
tibial tunnel; this procedure is the predecessor to current repairs in humans. A modification of this technique led to the first veterinary intra-articular repair. In 1952, Paatsama
described passing the lateral fascia lata through
bone tunnels in the femur and tibia and suturing it to soft tissue as the graft exited the
tunnel (Knecht 1976; Burnett & Fowler 1985).
The original repair has gone through multiple
modifications, including those by Singleton in
1957, Titemeyer and Brinker in 1958 and Rudy
in 1974, leading to the intra-articular repairs
most familiar to veterinarians, the ‘over-thetop’ and ’under-and-over’ techniques (Singleton 1957; Knecht 1976; Hulse et al. 1980; Shires
et al. 1984). As recently as 20–30 years ago,
intra-articular reconstructive techniques were
the preferred CrCL repair methods in dogs, and
have also been reported in cats (Korvick et al.
1994; Moore & Read 1995; Innes et al. 2000b;
Garcia et al. 2012). Although the outcomes
were subjective, some results were promising
(Pichler et al. 1982; Denny & Barr 1987; Innes &
VetBooks.ir
Intra-Articular Repair for Cranial Cruciate Ligament Rupture in the Dog
Barr 1998). With the development of extraarticular sutures and tibial osteotomies, intraarticular repairs fell out of favor due to their
inferior outcomes, continued stifle instability,
progressive cartilage degeneration, and donor
site morbidity (Butler et al. 1983; Elkins et al.
1991; Innes et al. 2000a; Johnson et al. 2001; Innes
et al. 2004; Conzemius et al. 2005; Snow et al.
2010; Molsa et al. 2014). These studies, as well
as surgeons’ own experiences with the procedure, have led to intra-articular repairs being
mostly abandoned in North America. However, a review of the literature addressing intraarticular repair in dogs identifies three common
limitations: inappropriate graft selection; inappropriate fixation; and an inappropriate biological environment for graft healing.
Graft selection
Autografts
The autograft is a natural extracellular matrix
(ECM) scaffold that initially can provide biomechanical properties similar to the native ligament, as well as a biochemical and structural
composition to guide cell growth. In addition,
growth factors may be trapped within the natural ECM, providing a source of biological stimuli that promote ligament fibroblast differentiation. Autografts also minimize the risk of
immune detection and disease transmission.
The use of autografts was described in many
original techniques and continues to be one
of the most commonly used grafts in humans
(Murray 2009). In veterinary medicine, using a
portion of the straight patella tendon or a strip
of the fascia lata is most commonly reported,
although skin, peroneus longus, flexor digitalis pedis longus, long digital extensor, periosteum and semitendinosus/gracilis autografts
have all been described (Chiroff 1975; Knecht
1976; Arnoczky et al. 1979a; Ramanaiah et al.
1990; Innes et al. 2000a; Lopez et al. 2003; Veena
et al. 2003; Penha et al. 2007).
Patella tendon autograft use, a technique
modified from human medicine, allows for
either bone or soft tissue anchor points,
and was first described by Dueland in 1966
(Dueland 1966). Dueland harvested the central
third of the straight patella tendon and patella,
creating a tendon-bone graft. The distal end
203
of the graft maintained attachment to the
tibia, while the free proximal end was passed
through a femoral tunnel and sutured to the
gastrocnemius. Although Dueland felt the
outcomes were good, very few were reported.
Subjective outcomes were promising enough
that the procedure and its modifications were
performed by Dueland until his retirement.
A modification was described in 1979, where
the lateral third of the straight patella tendon,
as well as a strip of fascia lata, was passed
through the joint and over the caudal aspect
of the lateral condyle, often referred to as the
‘over-the-top’ technique (Arnoczky et al. 1979a;
Arnoczky et al. 1979b; Denny & Barr 1984;
Bennett & May 1991).
Although intra-articular autografts have been
described for over 50 years, there is a paucity
of information on the suitability of these
grafts, specifically their ability to heal, graft
mechanical strength, graft attachment mechanical strength and donor site morbidity. Objective
outcomes were evaluated in 1975, when healing was assessed in experimentally replaced
CrCL using a third of the patella tendon
(Chiroff 1975). Both the tendon and bone underwent necrosis before more rapid ingrowth
occurred. Although healing progressed quickly
initially, incorporation remained incomplete at
one year. The modified ‘over-the-top’ technique
showed there was graft revascularization where
the graft contacted the fat pad and caudal joint
soft tissues, suggesting vessel ingrowth into
the sides of the graft rather than longitudinal revascularization (Arnoczky et al. 1979b;
Arnoczky et al. 1982). In contrast, a small pilot
study showed that at one year, a hamstring
graft had histopathology similar to the normal
CrCL. Clinically, it was reported the patients
were not showing signs of lameness (Lopez et al.
2003). Subsequent studies have revealed similar results of incomplete and inconsistent revascularization and repopulation based on graft
selection (Bacon et al. 1984; McFarland et al.
1986; Ng et al. 1995; Fu et al. 1999).
Available data showing the initial in vitro and
in vivo mechanical strength of common autografts is minimal. Given the critical role that
the CrCL plays in stifle mechanics, it is believed
to be of paramount importance to demonstrate
that a surgical technique can reproduce the
salient mechanical features of the intact CrCL.
Tensile testing of the medial third, central third
VetBooks.ir
204
Surgical Treatment
and lateral third, in combination with the fascia
lata, revealed that no graft was able to mimic
the strength or stiffness of the native CrCL.
Although the central and lateral thirds were
stronger than the medial third, it is likely that
no partial patella tendon graft has the mechanical properties necessary for recovery in the dog
(Butler et al. 1983; Johnson et al. 1989). In fact, it
has been reported that the entire patellar tendon
is needed to reproduce the mechanical properties of the CrCL. (Biskup et al. 2014b) Mechanical properties of the patella tendon autografts
at 4, 12, and 26 weeks after surgery revealed
strength and stiffness increasing and elongation
decreasing at each time point, although grafts
never reached the full strength of the intact
CrCL. Compared to extra-articular repairs, both
a third of the patella tendon and a fascia lata
strip showed less stiffness and greater laxity
compared to fibular head transposition and lateral imbrication (Patterson et al. 1991). Clinical assessment of laxity postoperatively showed
that the lateral third of the patella tendon
with a fascia lata strip placed in an ‘over-the–
top’ technique had increased laxity at 4 weeks
after surgery before decreasing laxity out to
26 weeks. At 26 weeks, laxity of 2.5 mm was still
more than the intact CrCL at 1.8 mm (Hulse et al.
1983).
A limited number of clinical studies have
been conducted with subjective and objective
outcomes to assess the mechanical strength of
common autografts. In one study, examinations were made of dogs with naturally occurring CR repaired with a fascial ‘over-the-top’
graft and assessed with an owner questionnaire
and force platform analysis. With an almost
1.5 year follow-up, owner satisfaction was very
high, although gait analysis revealed significantly decreased peak vertical force (Geels et al.
2000). OA also progressed in all dogs. Similar
results were found in 21 dogs with patella tendon/fascia lata grafts (Vasseur & Berry 1991).
All owners felt that their dog showed significant
improvement, although instability and progressive OA were documented in most cases.
A unique challenge to autograft collection
is donor site morbidity. A mechanical study
of the patella tendon after removal of its
central third revealed the cross-sectional area
to be dramatically increased over the control
tendon, although strength was significantly less
at 3 and 6 months (Linder et al. 1994). Another
study revealed that the donor patella tendon
decreased in failure strength by 30% compared
to a control at 6 months (Burks et al. 1990).
Although autografts have shown promise, an
autograft with the necessary mechanical properties that minimize donor site morbidity has
not been described. Further work is necessary
before autografts could be commonly used for
CrCL repair.
Allografts
Allograft benefits include a natural ECM scaffold, with the benefit of no donor site morbidity. With allografts, a whole tendon can be used,
such as the entire patella tendon rather than a
third of the patella tendon. The donor tendon
is readily available without needing intraoperative collection, Finally, there is the option of
using a ligament graft, such as the CrCL, as an
allograft. Although allografts have these advantages, they raise concern of disease transmission, immunological reaction, and alteration of
ingrowth characteristics.
Risk of disease transmission in veterinary
medicine is unlikely, especially if appropriate
donor screening is performed, if grafts are collected in a timely manner with sterile technique,
if post-collection monitoring is performed, and
graft tracking is ensured to record any future
complications. Specific protocols are often readily available from companies providing allografts commercially.
The detection, reaction, and destruction of
a graft is always a concern when foreign tissue is implanted in the body. The placement of
a fresh allograft would increase the likelihood
of an immune-directed inflammatory response,
although this is not commonly performed,
nor is it currently feasible for CrCL replacement. More commonly, allografts are treated
with an acute deep-freeze, cyclic deep-freeze–
thaw cycles, freeze-drying, gamma-irradiation
or ethylene oxide. The freezing of tendons or
ligaments has been shown to decrease disease transmission and immunogenic potential,
although some protocols may decrease mechanical properties (Gut et al. 2016). In a dog model,
central-third patella autografts were compared
to similar deep-frozen allografts (Arnoczky et al.
VetBooks.ir
Intra-Articular Repair for Cranial Cruciate Ligament Rupture in the Dog
1986). At 1 year, both grafts had a similar
appearance on histopathology. In a study of 25
dogs, central-third patella tendon deep-frozen
allografts were implanted and showed evidence
of revascularization at 6 weeks, and a similar
histopathologic appearance to the native CrCL
at 30 weeks (Shino et al. 1984). In a similar study
comparing frozen CrCL allografts to CrCL autografts (Kirkpatrick et al. 1996), allografts were
weaker than autografts, and appeared to have
delayed revascularization at all time points up
to 24 months.
Gamma-irradiation is effective at decreasing negative biological reactions in the
recipient, but can greatly alter mechanical
properties (Fu et al. 1999); this effect seems
to be dose-dependent (Fideler et al. 1995).
Goertzen reported that bone-ligament-bone
CrCL grafts deep-frozen and sterilized with
gamma-irradiation had similar strength as
non-irradiated frozen grafts. At 12 months after
implantation, the grafts had 60–70% strength
of the normal CrCL and a similar collagen
pattern (Goertzen et al. 1995). Although 60
dogs were studied, limitations included the
fact that limbs were immobilized for 5 weeks
after surgery, and functional outcome was not
assessed. Ethylene oxide has minimal effects of
mechanical properties, but residues could be
either inflammatory or carcinogenic (Silvaggio
et al. 1993; Bechtold et al. 1994).
205
A final emerging technique to decrease
immunogenic potential while maintaining
mechanical integrity of the graft is called
decellularization. This refers to the process of
removing cells from the tissue while preserving
the structural and functional proteins that
constitute the ECM. Decellularized tissue scaffolds have the potential to provide available
biocompatible graft material that can resemble
native tissue structurally, biochemically, and
biomechanically (Hoganson et al. 2010; Pridgen
et al. 2011). Many different decellularization
protocols have been described, and evaluation
of the process is in its infancy. Potential negative effects include impairment of the viability
of colonizing cells with chemical residues,
wash-out of growth factors bound by the ECM,
loss of ECM structure, and the induction of
sterile inflammation (Schultze-Tanzil et al.
2012). In veterinary medicine, a described
protocol reduced the mean DNA content by
between 44% and 83% in an equine tendon
(Youngstrom et al. 2013). In addition to verifying the removal of antigenic debris, it is also
necessary to confirm that desirable components
of the ECM (i.e., glycosaminoglycans, collagen,
protein) are retained. A similar protocol was
evaluated on the canine deep digital flexor
tendon and superficial digital flexor tendon
(Balogh et al. 2016) (Figure 26.1). The histological, biochemical, and mechanical results of
Figure 26.1 Image of a decellularized deep digital flexor tendon being prepared for implantation as a cranial cruciate
ligament allograft.
VetBooks.ir
206
Surgical Treatment
decellularization on deep digital flexor tendons
showed a significant decrease in DNA content,
preservation of the ECM, and no significant
change in mechanical properties.
The use of allografts has been described in
veterinary medicine (Shino et al. 1984; Vasseur
et al. 1991), with studies examining ideal graft
size, mechanical strength, histology, and clinical outcome (Qu et al. 2015). Vasseur et al.
1985 replaced the CrCL with CrCL allografts
in mixed-breed dogs in two studies. The first
study resulted in unstable stifles at 9 months,
with the allografts appearing immunogenic and
reaching only 14% of the strength of the intact
CrCL. A second study, although small and
short-term, demonstrated the possibility of a
successful outcome (Vasseur et al. 1987). Dogs
with stable stifles immediately after surgery
had a full recovery to normal gait (two dogs),
but when laxity was detected after surgery,
all dogs failed to have a successful outcome.
Thorson et al. 1989 performed a similar study,
implanting CrCL allografts in 11 patients with
a 73% failure rate. Three dogs developed infections and were removed from the study, and
five of the remaining eight dogs had a limp at
4 months (Thorson et al. 1989). Unfortunately,
there was no description of graft size or fixation strength. The above described study found
that allografts reached anywhere from 10% to
59% of the ultimate strength of an intact CrCL.
A more encouraging study included 28 dogs
which received CrCL allografts. Clinical assessment of the dogs was not discussed, but allografts reached 90% ultimate strength of the normal CrCL at 36 weeks (Nikolaou et al. 1986).
Although the outcome measures were not clinical, these authors concluded there were only
three failures during the 18-week study.
Freeze-dried fascia lata strips have also
served as allografts. In a study of medium-sized
dogs, eight patients underwent the ‘over-thetop’ procedure, and eight dogs had graft placement through bone tunnels. At 24 weeks, both
groups showed graft incorporation. Failure of
the grafts occurred at 536 N, compared to 801 N
for the intact CrCL (Curtis et al. 1985).
Other reported allografts for CrCL repair
have included the submucosa, bovine pericardium, and the deep digital flexor tendon
(Figure 26.2) (Aiken et al. 1994; Biasi et al. 2005;
Brendolan et al. 2007; Biskup et al. 2017).
Figure 26.2 Intra-articular placement of a deep digital
flexor tendon allograft to replace the cranial cruciate
ligament in an ex vivo stifle.
As allograft harvesting and preparation techniques continue to develop, allografts may be
an inviting option for CrCL repair. Further studies are required to determine initial strength, the
decrease in strength over time, cell ingrowth,
and immune reaction of any newly proposed
allograft.
Prosthetics
Prosthetic ligaments have been described as
either a primary repair or as augmentation for
biological grafts (Knecht 1976; Kdolsky et al.
1997; de Rooster et al. 2001; Mascarenhas &
MacDonald 2008; Müller et al. 2010; Müller
et al. 2011). Tissue-engineered scaffold biomaterials have been developed in attempts to
improve and accelerate healing or to reconstruct tendons or ligaments altogether. They
avoid donor site morbidity, eliminate the risk
VetBooks.ir
Intra-Articular Repair for Cranial Cruciate Ligament Rupture in the Dog
of disease transmission, and the initial strength
and stiffness can be selected. Braided nylon,
Teflon, Supramid, GoreTex and Dacron are just
some examples of materials described for ligament replacement. An early report showed
good subjective outcomes when polyethylene
suture was placed in an intra-articular location
in 98 dogs (Singleton 1969). The limitations of
these scaffolds include their diminished biocompatibility, unpredictable degradation rates,
and biomechanical weakening due to degradation (Liu et al. 2008). A canine study evaluated replacement of the CrCL using Dacron. The
groups included an ‘over-the-top’ placement,
femoral and tibial bone tunnel placement, and
the two techniques with extra-articular augmentation (Park et al. 1985). All grafts were
intact at 12 weeks with no loss in strength, but
at 24 weeks some grafts showed signs of wear
at the origin of the tunnels, with fibrous tissue ingrowth evident. A similar study using
polyester fiber placed in a similar manner produced equivalent results (Stead et al. 1991).
Studies have also investigated use of prosthetic material as a short-term brace for natural grafts. In dogs with CR, stifles were more
stable at 12 weeks when a fascia lata graft
and poly-L-lactide implant were used compared with the fascia lata graft alone, although
no differences were seen between the groups
by 24 weeks (Laitinen 1994). A separate study
showed that an intra-articular prosthetic graft
allowed improved healing of CrCL elongation
injury compared to an elongated CrCL with no
protection (Lopez et al. 2006).
Given the properties of the materials currently available, short-term success is often
observed, followed by long-term failure due to
a loss of mechanical strength before replacement with native tissue. If a material that promotes a rapid ingrowth of native cells, while
maintaining mechanical strength and limiting
biologic reaction, could be developed, then
prosthetic ligament replacement could be the
preferred technique for CrCL repair.
Fixation
Three main challenges arise when stabilizing an
intra-articular graft: placement at an ideal location, optimal tension at the time of fixation, and
207
development of a fixation method that will provide the required strength for recovery.
The CrCL has been described in detail
(Arnoczky 1983), and it is not a simple band.
First, there are two main components, the craniomedial and caudolateral bands, which interact intimately throughout range of motion. The
craniomedial band remains taut throughout a
range of motion as it twists close to 90◦ from
proximally to distally. The caudolateral band is
taut only in extension (Arnoczky & Marshall
1977). Intra-articular repair struggles to replicate this anatomy, and the ideal orientation of
an intra-articular graft at the time of fixation
is unknown. Second, the fan-like attachment to
the axial aspect of the lateral femoral condyle
and craniomedial tibia, underneath the intermeniscal ligament, make placement of bone
tunnels challenging. One limitation of many
intra-articular repairs previously reported is
that the graft is not placed at the attachment
sites of the CrCL (Bacon et al. 1984; Coetzee &
Lubbe 1995). The ‘over-the-top’ technique does
not follow the native path of the CrCL, but
rather passes the graft caudally and over the top
of the lateral condyle. This path also increases
the working length of the graft. When bone tunnels are created, the ideal location within the
CrCL attachment site is unknown. In humans,
it has been shown that bone tunnel placement
in the attachment sites of the ACL may not be
perfectly isometric points (Austin et al. 2007). In
dogs, it is suggested that the isometric location
may be caudal to the femoral attachment site of
the CrCL (Palmisano et al. 2000).
The next challenge with graft fixation is
deciding the ideal tension to be placed on the
graft while it is being secured. This has been
extensively explored in humans, with variation in recommendations based on the graft
and technique used (Mae et al. 2008; Grunau
et al. 2016). Obviously, too little tension will
result in postoperative laxity, but too much tension can change the contact mechanics, decrease
the range of motion and affect healing (Austin
et al. 2007; Mae et al. 2008). A study exploring hamstring grafts in dogs found that, when
placed under minimal tension (1 N), graft survival was superior when compared with high
tension (39 N) (Yoshiya et al. 1987). Preconditioning grafts with static or cyclic tension
is another highly investigated area of human
VetBooks.ir
208
Surgical Treatment
ligament replacement. A report describing
human semitendinosus grafts assessed a single
acute 80 N pull, a static 88 N pull for 20 minutes, or 20 cyclic pulls, each of 80 N. Cadaveric testing showed that either the extended
load or cyclic load was superior for preventing initial elongation (Pilia et al. 2015). In contrast, a study with a similar protocol found no
benefit when the secured grafts were tested in
using cyclic loading (Boguszewski et al. 2015).
No studies have been performed in dogs for
CrCL graft placement, although it has been suggested that preconditioning a CrCL allograft
would be important to eliminate initial elongation (Yahia & Drouin 1990). Stifle angle at
the time of fixation could also affect tension. A
study in dogs showed that the fixation angle
had a greater effect on graft tension than tunnel
location (Shelley et al. 1996). Although the ideal
angle was unknown, the study suggested that
stifles should not be flexed to 90◦ at the time of
fixation.
Finally, graft fixation methods are varied, and
the optimal method continues to be debated.
In humans, multiple techniques for securing
bone–ligament and soft tissue grafts have been
described, including interference screws, pinning, spiked washers, and suture (Hill et al.
2005). Interference screws are commonly used
in human surgery, and when used in a repair
technique they reportedly have an in vitro
strength of between 463 and 1358 N (Kousa
et al. 1995; Rupp et al. 1997). Possible benefits of
interference screws include ease of use, and that
they can be sized to accommodate grafts with
different cross-sectional areas, which improves
the contact between the bone tunnel and graft.
When using grafts that are folded to double
the graft, such as the hamstring tendon or
deep digital flexor tendon (DDFT), a cross-pin
technique is an alternative fixation technique
(Harilainen & Sandelin 2009). In cross-pin transfixation techniques, a pin is passed through the
loop created at the fold in the graft. The remaining graft ends can be secured with one of the
above-mentioned techniques.
A unique challenge in the dog is that the
initial fixation strength has to overcome daily
forces encountered by the CrCL, as a gradual increase in weight-bearing is not possible
as in humans. In ex vivo canine stifles, it was
shown that an entire patella tendon secured
with interference screws or with bone anchors
was likely not strong enough to withstand daily
physiologic loads (Biskup et al. 2015). However,
when DDFT was secured with a cross-pin and
spikes washers, the mechanical strength was
similar that of the native CrCL (Figure 26.3).
Similarly, a novel graft fixation device has been
shown to have equal strength to spiked washers (Lopez et al. 2007). In veterinary medicine,
previous reports of commonly performed intraarticular repairs showed grafts to be secured
most frequently only with suture (Bacon et al.
1984; Coetzee & Lubbe 1995). Suture stabilization of a graft undoubtedly provides insufficient
strength for patient use.
Fixation methods continue to progress in
human and veterinary medicine. The unique
challenges with management of canine patients
immediately postoperatively must be considered when choosing a method. Further studies
are needed to examine the effect of tunnel location and graft tension on healing and clinical
outcome.
Biology
Although it is believed that CrCL graft and fixation mechanics must be sound, intra-articular
graft placement also creates biological challenges, including the obstacle of intra-articular
healing, promotion of vascular ingrowth
and remodeling, and avoidance of immunemediated rejection.
It is important to understand that intraarticular graft healing differs from the healing of other extra-articular ligaments. Experiments have evaluated the ability of the ACL in
humans to heal compared to the healing potential of the medial collateral ligament, a ligament
which is responsive to medical therapy (Murray
et al. 2006; Murray et al. 2007). Cell proliferation
responses were shown to be similar between
the two ligaments. Therefore, the authors suggested that the differences must be in the biologic and mechanical environments. Similar to
the ACL, CrCL healing occurs in a unique environment, intra-articularly but extrasynovial,
due to its being completely covered by a synovial membrane. When the CrCL is damaged,
the hematoma that usually forms a scaffold for
healing is dissipated in the joint. Also, when
VetBooks.ir
Intra-Articular Repair for Cranial Cruciate Ligament Rupture in the Dog
(A)
(B)
Figure 26.3 Lateral (A) and craniocaudal (B)
radiographs of a stifle at one year after placement of an
intra-articular deep digital flexor tendon allograft secured
with a cross-pin on the femur and spiked washer on the
tibia.
209
the synovial sheath is disrupted, the ligament
is exposed to synovial fluid, which contains
inflammatory mediators. The sheath contains
vessels that serve as an important blood supply to the ligament (Murray et al. 2006). When
a graft is initially placed, it lacks the synovial
sheath, and this is suggested to deprive the
graft of an early blood supply and expose it to
inflammatory mediators (Arnoczky & Marshall
1981). The CrCL is exposed to constant mechanical forces during weight-bearing, and it is difficult to protect the ligament with a brace or
internal repair. In a CrCL model, the ends of a
transected CrCL were sutured into apposition,
and the stifle was immobilized. At 10 weeks,
the CrCL had shown evidence of healing but
did not reach full strength (O’Donoghue et al.
1966). Lastly, an appropriate scaffold is necessary for cell migration. In one study, a 3.5mm defect was created in the CrCL, leaving
peripheral bands to provide stability (Spindler
et al. 2006). The defect failed to show significant healing over a 6-week period. The addition of a collagen–platelet-rich plasma scaffold
promoted healing over the same time period
(Murray et al. 2006; Silva et al. 2013). These studies demonstrate the importance, for any graft,
of a suitable scaffold for cell migration and the
necessity to mechanically protect the graft during healing.
Autografts and allografts provide a natural ECM to guide cell ingrowth and, if processed appropriately, can initially maintain a
similar mechanical strength. All grafts will lose
strength over time if replacement with appropriate native tissue does not proceed rapidly.
One possible stimulant is the proteins in the
ECM of a donor autograft or allograft (Hoganson et al. 2010). Although prosthetic implant
scaffold technology is improving, the threedimensional layout of the scaffold likely cannot perfectly mimic Nature. It is unknown how
a different matrix affects cell ingrowth. Both
natural and synthetic scaffolds can be seeded
with protein, or potentially cells, to promote
ingrowth (Linon et al. 2014).
Many surgeons believe that intra-articular
grafts historically failed due to biological breakdown, similar to the fate of the native CrCL.
The exact pathogenesis of CR is not known
(Comerford et al. 2011) and, therefore, there is
no definitive evidence that an implanted graft
VetBooks.ir
210
Surgical Treatment
will undergo the same degradation as the native
CrCL. The immune rejection of allografts or
prosthetic materials is a concern. Processing
of allografts, including deep-freezing, chemical treatment or decellularization, may decrease
this potential. Prosthetic graft replacements will
likely become more biocompatible as new materials are developed. With any graft, further in
vivo experimental and clinical studies will be
needed in dogs to demonstrate the safety and
efficacy of any implanted intra-articular graft.
Future developments
Although extra-articular repairs continue to be
the most common surgical treatment for CR,
work should continue overcome the limitations
of extra-articular repairs and the challenges of
intra-articular repair identified in this chapter.
In the search for a suitable graft, in vitro mechanical testing has revealed that the entire patella
tendon and the DDFT allograft, when doubled
on itself, possess similar mechanical properties
to the native CrCL of a similar-sized dog (Haut
et al. 1992; Biskup et al. 2014b; Biskup et al.
2015). Fixation methods have also been evaluated, placing different grafts at the proximal
and distal attachment sites of the CrCL (Biskup
et al. 2015). Results have shown that securing a DDFT allograft with a medial femoral
cross-pin and tibial spiked washers and interference screws can mimic the mechanical properties of the native CrCL. Finally, a study evaluating the effect of decellularization on DDFTs
showed significant decreases in DNA content
upon histological and biochemical testing, but
no decrease in mechanical strength when compared to unprocessed allografts (Balogh et al.
2016).
Two recent in vivo studies have evaluated
intra-articular grafts with positive outcomes.
Cook et al. 2015 assessed replacement of the
craniomedial band of the CrCL with a long
digital extensor graft in research dogs. The
outcomes were positive, including no progression of OA and continued stifle function. A
small pilot prospective cohort study evaluated
the feasibility of intra-articular CrCL repair in
dogs with naturally occurring CR (Biskup et al.
2017). Ten client-owned dogs with unilateral
CR underwent a repair using a decellularized
Figure 26.4 Intraoperative picture of an intra-articular
repair using a deep digital flexor allograft. A drill guide is
in position to drill the femoral tunnel.
DDFT allograft placed at the femoral and tibial
attachment sites of the CrCL, and secured with
a medial femoral cross-pin and tibial spiked
washers and interference screws (Figure 26.4).
Owner questionnaire results showed improvement throughout the study, with the greatest
improvement over the first 6 months. Similarly,
peak vertical force and vertical impulse were
improved throughout all time points, with a
continued upward trend at 12 months. Radiographs revealed minimal progression of OA.
Mild subluxation was present in multiple dogs
on both orthopaedic examination and weightbearing radiographs. Notably, caution must be
taken when drawing conclusions from these
studies, given the small population size and the
fact that no direct treatment comparison was
performed (Figure 26.5). One critical limitation
was that graft integrity was not documented in
the pilot project. One possibility is that periarticular fibrosis may have contributed to clinical
outcome, although its contribution may be limited with intra-articular repairs (Hart et al. 2003).
Conclusions
Intra-articular repair in veterinary medicine
continues to be inferior to extra-articular
VetBooks.ir
Intra-Articular Repair for Cranial Cruciate Ligament Rupture in the Dog
211
Net GRF
2
1.9
1.8
1.7
Intra-articular
1.6
1.5
TPLO
1.4
NonSX
1.3
1.2
1.1
1
PreOp
2-month
6-month
12-month
Figure 26.5 Mean values of net ground reaction force (GRF) measured via force platform gait analysis of the limb with
cranial cruciate ligament rupture immediately before and at various time points after surgery. Values obtained were
during different time periods but data were collected by the same laboratory under identical conditions.
repairs in controlled studies and in surgeon
opinion. The potential mechanical benefit over
current stifle stabilization surgeries makes
its continued exploration justified, and likely
explains why intra-articular repairs remain the
‘gold standard’ for ACL rupture treatment in
human patients. As research into graft selection
and processing, fixation techniques and graft
healing advances, intra-articular repairs may
become more common in veterinary medicine.
References
Aiken SW, Badylak SF, Toombs JP, et al. Small intestinal submucosa as an intra-articular ligamentous
repair material: a pilot study in dogs. Vet Comp
Orthop Traumatol 1994;7:124–128.
Arnoczky SP. Anatomy of the anterior cruciate ligament. Clin Orthop Related Res 1983;172:19–25.
Arnoczky SP, Marshall JL. Pathomechanics of cruciate and meniscal injuries. In: Pathophysiology of
Small Animal Surgery, Bojrab MJ, ed. Philadelphia,
PA, Lea & Febiger. 1981, pp. 590–603.
Arnoczky SP, Marshall JL. The cruciate ligaments of
the canine stifle: an anatomical and functional analysis. Am J Vet Res 1977;38:1807–1814.
Arnoczky SP, Rubin RM, Marshall JL. Microvasculature of the cruciate ligaments and its response to
injury: an experimental study in dogs. J Bone Joint
Surg 1979b;61A:1221–1229.
Arnoczky SP, Tarvin GP, Marshall JL. Anterior cruciate ligament replacement using patella tendon.
J Bone Joint Surg 1982;64A:217–224.
Arnoczky SP, Tarvin GP, Marshall JL, et al. The overthe-top procedure: a technique for anterior cruciate
ligament substitution in the dog. J Am Anim Hosp
Assoc 1979a;15:283–290.
Arnoczky SP, Warren RF, Ashlock MA. Replacement
of the anterior cruciate ligament using a patellar
tendon allograft. An experimental study. J Bone
Joint Surg Am 1986;68:376–385.
Austin JC, Phornphutkul C, Wojtys EM. Loss of knee
extension after anterior cruciate ligament reconstruction: effects of knee position and graft tensioning. J Bone Joint Surg Am 2007;89:1565–1574.
Bacon JP, Pichler ME, Lynd FT, et al. Histopathological examination of two cranial cruciate ligament reconstructions. J Am Anim Hosp Assoc
1984;20:65–68.
Balogh DG, Biskup JJ, O’Sullivan MG, et al. Biochemical, histologic, and biomechanical characterization
of native and decellularized flexor tendons specimens harvested from the pelvic limbs of orthopedically normal dogs. Am J Vet Res 2016;77:388–
394.
Bechtold JE, Eastlund DT, Butts MK, et al. The effects
of freeze-drying and ethylene oxide sterilization on
the mechanical properties of human patellar tendon. Am J Sports Med 1994;22:562–566.
Bellumori TP, Famula TR, Bannasch DL, et al. Prevalence of inherited disorders among mixed-breed
and purebred dogs: 27,254 cases (1995–2010). J Am
Vet Med Assoc 2013;242:1549–1555.
Bennett D, May C. An “over-the-top with tibial tunnel” technique for repair of cranial cruciate ligament rupture in the dog. J Small Anim Pract
1991;32:103–110.
Bennett D, Tennant B, Lewis DG, et al. A reappraisal
of anterior cruciate ligament disease in the dog.
J Small Anim Pract 1988;29:275–297.
VetBooks.ir
212
Surgical Treatment
Biasi F, Rahal SC, Volpi RS, et al. Cranial cruciate
ligament reconstruction in dogs associated or not
to chondroitin sulfate. Arq Bras Med Vet Zootec
2005;57:442–447.
Biskup JJ, Balogh DG, Haynes KH, et al. Mechanical strength of four allograft fixation techniques for
ruptured cranial cruciate ligament repair in dogs.
Am J Vet Res 2015;76:411–419.
Biskup JJ, Balogh DG, Scott RM, et al. Long-term outcome of an intra-articular allograft technique for
treatment of spontaneous cranial cruciate ligament
rupture in the dog. Vet Surg 2017;46:691–699.
Biskup J, Freeman A, Camisa W, et al. Mechanical properties of canine patella-ligament-tibia segment. Vet Surg 2014b;43:136–141.
Biskup JJ, Griffon DJ, Socie M, et al. Ability of
the Tightrope® and percutaneous lateral fabellar
suture techniques to control cranial tibial translation. Vet Surg 2014a;43:959–965.
Boguszewski DV, Joshi NB, Wang D, et al. Effect
of different preconditioning protocols on anterior
knee laxity after ACL reconstruction with four
commonly used grafts. J Bone Joint Surg Am
2015;97:1059–1066.
Brendolan AP, Rezende CMF, Melo EG, et al. Clinical and radiographic aspects of the bovine pericardium as a substitute of the canine cranial cruciate ligament. Arq Bras Med Vet Zootec 2007;59:920–
931.
Burks RT, Haut RC, Lancaster RL. Biomechanical and
histological observations of the dog patellar tendon
after removal of its central one-third. Am J Sports
Med 1990;18:146–153.
Burnett QM, Fowler PJ. Reconstruction of the anterior
cruciate: historical review. Orthop Clin North Am
1985;16:143–157.
Butler DL, Hulse DA, Kay MD, et al. Biomechanics of
cranial cruciate ligament reconstruction in the dog
II. Mechanical properties. Vet Surg 1983;12:112–
118.
Cabano NR, Troyer KL, Palmer RH, et al. Mechanical comparison of two suture constructs for extracapsular stifle stabilization. Vet Surg 2011;40:334–
339
Chiroff RT. Experimental replacement of the anterior
cruciate ligament. J Bone Joint Surg 1975;57A:1124–
1127.
Coetzee GL, Lubbe AM. A prospective study comparing two fascial reconstruction techniques to stabilise the cranial cruciate deficient stifle in the dog.
Vet Comp Orthop Traumatol 1995;8:82–90.
Comerford EJ, Smith K, Hayashi K. Update on
the aetiopathogenesis of canine cranial cruciate
ligament disease. Vet Comp Orthop Traumatol
2011;24:91–98.
Conzemius MG, Evans RB, Besancon MF, et al. Effect
of surgical technique on limb function after surgery
for rupture of the cranial cruciate ligament in dogs.
J Am Vet Med Assoc 2005;226:232–236.
Cook JL, Smith PA, Stannard JP, et al. A canine hybrid
double-bundle model for study of arthroscopic
ACL reconstruction. J Orthop Res 2015;33:1171–
1179.
Corr SA, Brown C. A comparison of outcomes following tibial plateau levelling osteotomy and cranial tibial wedge osteotomy procedures. Vet Comp
Orthop Traumatol 2007;20:312–319.
Curtis RJ, Delee JC, Drez DJ, Jr. Reconstruction of the
anterior cruciate ligament with freeze dried fascia
lata allografts in dogs. A preliminary report. Am J
Sports Med. 1985;13:408–414.
Davarinos N, O’Neill BJ, Curtin W. A brief history
of anterior cruciate ligament reconstruction. Adv
Orthop Surg 2014:706042.
DeLuke AM, Allen DA, Wilson ER, et al. Comparison of radiographic osteoarthritis scores in dogs
less than 24 months or greater than 24 months following tibial plateau leveling osteotomy. Can Vet J
2012;53:1095–1099.
Denny HR, Barr ARS. A further evaluation of the
“over-the-top” technique for anterior cruciate ligament replacement in the dog. J Small Anim Pract
1987;28:681–686.
Denny HR, Barr ARS. An evaluation of two “over
the top” techniques for anterior cruciate ligament replacement in the dog. J Small Anim Pract
1984;25:759–769.
de Rooster H, Vangheluwe L, van Bree H, et al. Biomechanical properties of braided polyester tapes
intended for use as intra-articular cranial cruciate ligament prostheses in dogs. Am J Vet Res
2001;62:48–53.
Dueland TR. A recent technique for reconstruction of the anterior cruciate ligament. Anim Hosp
1966;2:1–5.
Elkins AD, Pechman R, Kearney MT, et al. A retrospective study evaluating the degree of degenerative joint disease in the stifle joint of dogs following surgical repair of anterior cruciate ligament
rupture. J Am Anim Hosp Assoc 1991;27:533–
540.
Evans R, Horstman C, Conzemius M. Accuracy and
optimization of force platform gait analysis in
Labradors with cranial cruciate disease evaluated
at the walking gait. Vet Surg 2005;34:445–449.
Fideler BM, Vangsness CT, Jr, Lu B, et al. Gamma
irradiation: effects on biomechanical properties of
human bone-patellar tendon-bone allografts. Am J
Sports Med 1995;23:643–646.
Fischer C, Cherres M, Grevel V, et al. Effects of attachment sites and joint angle at the time of lateral
suture fixation on tension in the suture for stabilization of the cranial cruciate ligament deficient stifle
in dogs. Vet Surg 2010;39:334–342.
Fu FH, Bennett CH, Latterman C, et al. Current trends
in anterior cruciate ligament reconstruction. Part 1:
biology and biomechanics of reconstruction. Am J
Sports Med 1999;27:821–830.
VetBooks.ir
Intra-Articular Repair for Cranial Cruciate Ligament Rupture in the Dog
Garcia ÉFV, Schossler JEW, Pinheiro M. Cranial cruciate ligament rupture in a cat: reconstitution with
fascia lata. Ciênc Rural 2012;42:1446–1449.
Geels JJ, Roush JK, Hoskinson JJ, et al. Evaluation of
an intracapsular technique for the treatment of cranial cruciate ligament rupture. Vet Comp Orthop
Traumatol 2000;13:197–203.
Goertzen MJ, Clahsen H, Bürrig KF, et al. Sterilisation of canine anterior cruciate allografts by gamma
irradiation in argon. Mechanical and neurohistological properties retained one year after transplantation. J Bone Joint Surg Br. 1995;77:205–212.
Gordon WJ, Conzemius MG, Riedesel E, et al.
The relationship between limb function and
radiographic osteoarthrosis in dogs with stifle
osteoarthrosis. Vet Surg 2003;32:451–454.
Gordon-Evans WJ, Griffon DJ, Bubb C, et al. Comparison of lateral fabellar suture and tibial plateau leveling osteotomy techniques for treatment of dogs
with cranial cruciate ligament disease. J Am Vet
Med Assoc 2013;243:675–680. Erratum in: J Am Vet
Med Assoc 2013;243:1297.
Grunau PD, Arneja S, Leith JM. A randomized clinical trial to assess the clinical effectiveness of a
measured objective tensioning device in hamstring
anterior cruciate ligament reconstruction. Am J
Sports Med 2016;44:1482-1486.
Gut G, Marowska J, Jastrzebska A, et al. Structural mechanical properties of radiation-sterilized
human bone-tendon-bone grafts preserved by different methods. Cell Tissue Bank 2016;17:277-287.
Harilainen A, Sandelin J. A prospective comparison of 3 hamstring ACL fixation devices – Rigidfix, BioScrew, and Intrafix – randomized into 4
groups with 2 years of follow-up. Am J Sports Med
2009;37:699–706
Hart RC, Hulse D, Slater MR. Contribution of periarticular tissue to stabilization of the canine stifle
joint after cranial cruciate ligament reconstruction.
Vet Comp Orthop Traumatol 2003;1:21–25.
Haut RC, Lancaster RL, DeCamp CE. Mechanical
properties of the canine patellar tendon: some correlations with age and the content of collagen.
J Biomech 1992;25:163–173.
Heffron LE, Campbell JR. Morphology, histology and
functional anatomy of the canine cranial cruciate
ligament. Vet Rec 1978;102:280–283.
Hill C, An YH, Young FA. Tendon and ligament fixation to bone. In: Repair of Ligament and Tendons,
Walsh W, ed. Totowa, NJ, Humana Press. 2005,
pp. 257–278.
Hoffman DE, Miller JM, Ober CP, et al. Tibial tuberosity advancement in 65 canine stifles. Vet Comp
Orthop Traumatol 2006:4;219–227.
Hoganson DM, O’Doherty EM, Owens GE, et al.
The retention of extracellular matrix proteins and
angiogenic and mitogenic cytokines in a decellularized porcine dermis. Biomaterials 2010;31:6730–
6737.
213
Hulse D, Beale B, Kerwin S. Second look arthroscopic
findings after tibial plateau leveling osteotomy. Vet
Surg 2010a;39:350–354.
Hulse D, Hyman W, Beale B, et al. Determination of
isometric points for placement of a lateral suture in
treatment of the cranial cruciate ligament deficient
stifle. Vet Comp Orthop Traumatol 2010b;23:163–
167.
Hulse DA, Butler DL, Kay MD, et al. Biomechanics of
cranial cruciate ligament reconstruction in the dog
I. In vitro laxity testing. Vet Surg 1983;12:109–112.
Hulse DA, Michaelson F, Johnson C, et al. A technique
for reconstruction of the anterior cruciate ligament
in the dog: preliminary report. Vet Surg 1980;4:135–
140.
Innes JF, Bacon D, Lynch C, et al. Long-term outcome
of surgery for dogs with cranial cruciate ligament
deficiency. Vet Rec 2000b;147:325–328.
Innes JF, Barr AR. Clinical natural history of the postsurgical cruciate deficient canine stifle joint: year 1.
J Small Anim Pract. 1998;39:325–332.
Innes JF, Barr AR, Sharif M. Efficacy of oral calcium pentosan polysulphate for the treatment of
osteoarthritis of the canine stifle joint secondary
to cranial cruciate ligament deficiency. Vet Rec
2000a;146:433–437.
Innes JF, Costello M, Barr FJ, et al. Radiographic
progression of osteoarthritis of the canine stifle
joint: a prospective study. Vet Radiol Ultrasound
2004;45:143–148.
Jevens DJ, DeCamp CE, Hauptman J, et al. Use of
force-plate analysis of gait to compare two surgical techniques for treatment of cranial cruciate ligament rupture in dogs. Am J Vet Res 1996;57:389–
393.
Johnson JA, Austin C, Breur GJ. Incidence of canine
appendicular musculoskeletal disorders in 16 veterinary teaching hospitals from 1980 to 1989. Vet
Comp Orthop Traumatol 1994;7:56–59.
Johnson KA, Hart RC, Chu Q, et al. Concentrations of
chondroitin sulfate epitopes 3B3 and 7D4 in synovial fluid after intra-articular and extracapsular
reconstruction of the cranial cruciate ligament in
dogs. Am J Vet Res 2001;62:581–587.
Johnson SG, Hulse DA, Hogan HA, et al. System behavior of commonly used cranial cruciate ligament reconstruction autografts. Vet Surg
1989;18:459–465.
Kdolsky RK, Gibbons DF, Kwasny O, et al. Braided
polypropylene augmentation device in reconstructive surgery of the anterior cruciate ligament:
long-term clinical performance of 594 patients and
short-term arthroscopic results, failure analysis by
scanning electron microscopy and synovial histomorphology. J Orthop Res 1997;15:1–10.
Kim SE, Lewis DD, Pozzi A. Effect of tibial plateau
leveling osteotomy on femorotibial subluxation: in vivo analysis during standing. Vet Surg
2012;41:465–470.
VetBooks.ir
214
Surgical Treatment
Kirkpatrick JS, Seaber AV, Glisson RR, et al. Cryopreserved anterior cruciate ligament allografts in a
canine model. J South Orthop Assoc 1996;5:20–29.
Knecht CD. Evolution of surgical techniques for cruciate ligament rupture in animals. J Am Anim Hosp
Assoc 1976;12:717–726.
Korvick DL, Johnson AL, Schaeffer DJ. Surgeons’
preferences in treating cranial cruciate ligament
ruptures in dogs. J Am Vet Med Assoc 1994;205:
1318–1324.
Kousa P, Jarvinen TL, Pohjonen T, et al. Fixation
strength of a biodegradable screw in anterior cruciate ligament reconstruction. J Bone Joint Surg Br
1995;77:901–905.
Kowaleski MP, Apelt D, Mattoon JS, et al. The effect
of tibial plateau leveling osteotomy position on cranial tibial subluxation: an in vitro study. Vet Surg
2005;34:332–336.
Krotscheck U, Nelson SA, Todhunter RJ, et al.
Long term functional outcome of tibial tuberosity
advancement vs. tibial plateau leveling osteotomy
and extracapsular repair in a heterogeneous population of dogs. Vet Surg 2016;45:261–268.
Laitinen O. Prospective clinical study of biodegradable poly-1-lactide implant as an augmentation
device with fascia lata in cranial cruciate ligament
repair in the dog: early results. Vet Comp Orthop
Traumatol 1994;7:51–55.
Lazar TP, Berry CR, deHaan JJ, et al. Long-term
radiographic comparison of tibial plateau leveling osteotomy versus extracapsular stabilization
for cranial cruciate ligament rupture in the dog. Vet
Surg 2005;34:133–141.
Linder LH, Sukin DL, Burks RT, et al. Biomechanical and histological properties of the canine patellar tendon after removal of its medial third. Am J
Sports Med 1994;22:136–142.
Linon E, Spreng D, Rytz U, Forterre S. Engraftment of
autologous bone marrow cells into the injured cranial cruciate ligament in dogs. Vet J 2014;202:448–
454.
Liu Y, Ramanath HS, Wang D-A. Tendon tissue engineering using scaffold enhancing strategies. Trends
Biotechnol 2008;26:201–209.
Lopez MJ, Markel MM, Kalsheur VL, et al. Hamstring graft technique for stabilization of canine
cranial cruciate ligament deficient stifles. Vet Surg
2003;32:390–401.
Lopez MJ, Robinson SO, Quinn MM, et al. In vivo evaluation of intra-articular protection in a novel model
of canine cranial cruciate ligament mid-substance
elongation injury. Vet Surg 2006;35:711–720.
Lopez MJ, Spencer N, Casey JP, et al. Biomechanical characteristics of an implant used to secure
semitendinosus-gracilis tendon grafts in a canine
model of extra-articular anterior cruciate ligament
reconstruction. Vet Surg 2007;36:599–604.
Mae T, Shino K, Nakata K, et al. Optimization of graft
fixation at the time of anterior cruciate ligament
reconstruction. Part I: effect of initial tension. Am
J Sports Med 2008;36:1087–1093.
Mascarenhas R, MacDonald PB. Anterior cruciate
ligament reconstruction: a look at prosthetics –
past, present and possible future. McGill J Med
2008;11:29–37.
McFarland EG, Morrey BF, An KN, et al. The relationship of vascularity and water content to tensile strength in a patella tendon replacement of the
anterior cruciate ligament in dogs. Am J Sports
Med 1986;14:436–448.
Mölsä SH, Hielm-Bjorkman AK, Laitinen-Vapaavuori
OM. Use of an owner questionnaire to evaluate
long-term outcome and chronic pain after cranial
cruciate ligament repair in dogs: 253 cases (2004–
2006). J Vet Med Assoc 2013;243:689–695.
Mölsä SH, Hyytiäinen HK, Hielm-Björkman AK, et al.
Long-term functional outcome after surgical repair
of cranial cruciate ligament disease in dogs. BMC
Vet Res 2014;10:266.
Moore KW, Read RA. Cranial cruciate ligament rupture in the dog – a retrospective study comparing
surgical techniques. Aust Vet J 1995;72:281–285.
Müller DCM, Basso PC, Serafini GMC, et al. Replacement of the cranial and caudal cruciate ligaments
in dogs by double t polypropylene implant. Ciênc
Rural 2011;41:487–491.
Müller DCM, Pippi NL, Basso PC, et al. Synthetic
implant as a stabilizer link, after desmotomy of the
cruciate ligaments in dogs: proposition technique.
Ciênc Rural 2010;40:1327–1334.
Murray MM. Current status and potential of primary
ACL repair. Clin Sports Med 2009;28:51–61.
Murray MM, Spindler KP, Ballard P, et al. Enhanced
histologic repair in a central wound in the anterior cruciate ligament with a collagen-plateletrich plasma scaffold. J Orthop Res 2007;25:1007–
1017.
Murray MM, Spindler KP, Devin C, et al. Use of
a collagen-platelet rich plasma scaffold to stimulate healing of a central defect in the canine ACL.
J Orthop Res 2006;24:820–830.
Ng GY, Oakes BW, Deacon OW, et al. Biomechanics of
patella tendon autograft for reconstruction of the
anterior cruciate ligament in the goat: three year
study. J Orthop Res 1995;13:602–608.
Nikolaou PK, Seaber AV, Glisson RR, et al. Anterior
cruciate ligament allograft transplantation. Longterm function, histology, revascularization, and
operative technique. Am J Sports Med 1986;14:348–
360.
O’Donoghue DH, Rockwood CA, Frank GR, et al.
Repair of the anterior cruciate ligament in dogs.
Bone Joint Surg 1966;48A:503–519.
Palmisano MP, Andrish JT, Olmstead ML, et al. A
comparative study of the length patterns of anterior cruciate ligament reconstructions in the dog
and man. Vet Comp Orthop Traumatol 2000;13:73–
77.
VetBooks.ir
Intra-Articular Repair for Cranial Cruciate Ligament Rupture in the Dog
Park JP, Grana WA, Chitwood JS. A high-strength
Dacron augmentation for cruciate ligament reconstruction. A two-year canine study. Clin Orthop
Relat Res 1985;196:175–185.
Patterson RH, Smith GK, Gregor TP, et al. Biomechanical stability of four cranial cruciate ligament repair
techniques in the dog. Vet Surg 1991;20:85–90.
Penha EM, Rezende CMF, Melo EG, et al. Late postoperative of cranial cruciate ligament replacement in
dog. Arq Bras Med Vet Zootec 2007;59:1184–1193.
Pichler ME, Bacon JP, Evans JA. The fascia lata as a
replacement for the cranial cruciate ligament: two
new surgical techniques. J Am Anim Hosp Assoc
1982;18:779.
Pilia M, Murray M, Guda T, et al. Pretensioning of soft
tissue grafts in anterior cruciate ligament reconstruction. Orthopedics 2015;38:e582–e587.
Pridgen BC, Woon CY, Kim M, et al. Flexor tendon tissue engineering: Acellularization of human
flexor tendons with preservation of biomechanical
properties and biocompatibility. Tissue Eng Part C
Methods 2011;17:819–828.
Qu J, Thoreson AR, An K-N, et al. What is the best
candidate allograft for ACL reconstruction? An in
vitro mechanical and histologic study in a canine
model. J Biomech 2015;48:1811–1816.
Ramanaiah CV, Ramakrishna O, Sreeraman PK.
Chondrogenic potential of free intra-articular
periosteal autografts in dogs. Indian Vet J 1990;67:
844–847.
Rayward RM, Thomson DG, Davies JV, et al. Progression of osteoarthritis following TPLO surgery:
a prospective radiographic study of 40 dogs. J Small
Anim Pract 2004;45:92–97.
Roe SC, Kue J, Gemma J. Isometry of potential suture
attachment sites for the cranial cruciate ligamentdeficient canine stifle. Vet Comp Orthop Traumatol
2008;21:215–220.
Rose ND, Goerke D, Evans RB, et al. Mechanical testing of orthopedic suture material used for extraarticular stabilization of canine cruciate ligamentdeficient stifles. Vet Surg 2012;41:266–272.
Rupp S, Krauss PW, Fritsch EW. Fixation strength
of a biodegradable interference screw and a pressfit technique in anterior cruciate ligament reconstruction with a BPTB graft. Arthroscopy 1997;13:
61–65.
Schultze-Tanzil G, Al-Sadi O, Ertel W, et al. Decellularized tendon extracellular matrix – a valuable approach for tendon reconstruction? Cells
2012;1:1010–1028.
Shelley BA, Hulse DA, Slater MR, et al. Determination
of graft forces for cranial cruciate ligament reconstruction in the dog. Vet Comp Orthop Traumatol
1996;9:165–171.
Shino K, Kawasaki T, Hirose H, et al. Replacement of
the anterior cruciate ligament by an allogeneic tendon graft. An experimental study in the dog. J Bone
Joint Surg Br 1984;66:672–681.
215
Shires PK, Hulse DA, Liu W. The under-and-over fascial replacement technique for anterior cruciate ligament rupture in the dog: A retrospective study.
J Am Anim Hosp Assoc 1984;20:69–77.
Silva RF, Carmona JU, Rezende CM. Intra-articular
injections of autologous platelet concentrates in
dogs with surgical reparation of cranial cruciate
ligament rupture: a pilot study. Vet Comp Orthop
Traumatol 2013;26:285–290.
Silvaggio VJ, Fu FH, Georgescu HI, et al. The induction of IL-1 by freeze-dried ethylene oxide-treated
bone-patellar tendon-bone allograft wear particles:
an in vitro study. Arthroscopy 1993;9:82–86.
Singleton WB. The diagnosis and treatment of some
abnormal stifle conditions in the dog. Vet Rec
1957;69:1387–1394.
Singleton WB. Observations based upon the surgical repair of 106 cases of anterior cruciate ligament
rupture. J Small Anim Pract 1969;10:269–278.
Skinner OT, Kim SE, Lewis DD, Pozzi A. In vivo
femorotibial subluxation during weight-bearing
and clinical outcome following tibial tuberosity
advancement for cranial cruciate ligament insufficiency in dogs. Vet J 2013;196:86–91.
Snow LA, White R, Gustafson S, et al. Ex vivo comparison of three surgical techniques to stabilize canine
cranial cruciate ligament deficient stifles. Vet Surg
2010;39:195–207.
Spindler KP, Murray MM, Devin C, et al. The central
ACL defect as a model for failure of intra-articular
healing. J Orthop Res 2006;24:401–406.
Stauffer KD, Tuttle TA, Elkins AD, et al. Complications associated with 696 tibial plateau leveling
osteotomies (2001-2003). J Am Anim Hosp Assoc
2006;42:44–50.
Stead AC, Amis AA, Campbellt JR. Use of polyester
fibre as a prosthetic cranial cruciate ligament in
small animals. J Small Anim Pract 1991;32:448–454.
Stein S, Schmoekel H. Short-term and eight to 12
months results of a tibial tuberosity advancement
as treatment of canine cranial cruciate ligament
damage. J Small Anim Pract 2008;49:398–404.
Thorson E, Rodrigo JJ, Vasseur P, et al. Replacement
of the anterior cruciate ligament. A comparison
of autografts and allografts in dogs. Acta Orthop
Scand 1989;60:555–560.
Vasseur PB, Berry CR. Progression of stifle
osteoarthrosis following reconstruction of the
cranial cruciate ligament in 21 dogs. J Am Anim
Hosp Assoc 1991;28:129–136.
Vasseur PB, Stevenson S, Gregory CR, et al. Anterior
cruciate ligament allograft transplantation in dogs.
Clin Orthop Relat Res 1991;269:295–304.
Vasseur PB, Pool RR, Arnoczky SP, et al. Correlative biomechanical and histologic study of the
cranial cruciate ligament in dogs. Am J Vet Res
1985;46:1842–1854.
Vasseur PB, Rodrigo JJ, Stevenson S, et al. Replacement of the anterior cruciate ligament with a
VetBooks.ir
216
Surgical Treatment
bone-ligament-bone anterior cruciate ligament
allograft in dogs. Clin Orthop Relat Res 1987;219:
268–277.
Veena P, Ramakrishna O, Bharathi S, et al. Reconstruction of ruptured cranial cruciate ligament using
whole thickness skin and patellar ligament as a
graft in canines. Indian Vet J 2003;80:432–434.
Voss K, Damur DM, Guerrero T, et al. Force plate
analysis to assess limb function after tibial tuberosity advancement in dogs with cranial cruciate
ligament disease. Vet Comp Orthop Traumatol
2008;21:243–249.
Waxman AS, Robinson DA, Evans RB, et al. Relationship between objective and subjective assessment
of limb function in normal dogs with an experimentally induced lameness. Vet Surg 2008;3:241–
246.
Wucherer KL, Conzemius MG, Evans RB, et al. Shortterm and long-term outcomes for overweight dogs
with cranial cruciate ligament rupture treated surgically or nonsurgically. J Am Vet Med Assoc
2013;242:1364–1372.
Yahia LH, Drouin G. Study of the hysteresis phenomenon in canine anterior cruciate ligaments.
J Biomed Eng 1990;12:57–62.
Yoshiya S, Andrish JT, Manley MT, et al. Graft tension
in anterior cruciate ligament reconstruction. An in
vivo study in dogs. Am J Sports Med 1987;15:464–
470.
Youngstrom DW, Barrett JG, Jose RR, et al. Functional characterization of detergent-decellularized
equine tendon extracellular matrix for tissue
engineering applications. PLoS One 2013;8:
e64151.
VetBooks.ir
27
Tibial Plateau Leveling
Osteotomy
Susan L. Schaefer
Introduction
Tibial plateau leveling osteotomy (TPLO) was
first described in 1993 by Slocum to address stifle instability due to cruciate ligament rupture
(CR) (Slocum & Slocum 1993). By decreasing
the natural caudodistal orientation of the tibial plateau, TPLO limits the shear force generated by compression of the stifle during weightbearing, thereby abating cranial tibial thrust
(Reif et al. 2002). The dynamic stability imparted
to the cranial cruciate ligament (CrCL)-deficient
stifle via TPLO is achieved by performing a
radial osteotomy of the proximal tibia and rotating the proximal segment to decrease the tibial
plateau angle (TPA) (Figure 27.1).
Preoperative determination of the patient’s
TPA allows calculation of the magnitude of
rotation necessary to achieve a desired postoperative TPA. The minimum amount of rotation required to neutralize cranial tibial thrust
results in a postoperative TPA of 6.5 ± 0.9◦ . Further rotation increases strain on the caudal cruciate ligament (CaCL); rotating from 6.5◦ to 0◦
increases CaCL strain by 37.7 ± 17.4% (Warzee
et al. 2001). While convention dictates measuring and changing the TPA, more recent studies
have evaluated the patella tendon angle (PTA)
change seen in TPLO. After TPLO, the PTA
measures around 90◦ in both ex vivo and clinical
situations (Drygas et al. 2010; Sathya et al. 2014).
This finding suggests that the biomechanics of
TPLO may be similar to that of tibial tuberosity advancement (TTA). It is important to note
that the TPLO procedure itself only addresses
dynamic stifle instability. Therefore, an inspection of intra-articular structures with appropriate treatment of meniscal injuries or other
abnormalities must accompany the procedure.
An excellent review of the proposed mechanism of action for TPLO is available (Boudrieau
2009).
TPLO technique
The magnitude of rotation planned preoperatively generally correlates well with the
realized postoperative TPA result (Windolf et al.
2008). However, achieving an accurate TPA
measurement and executing the osteotomy and
tibial rotation in a manner to accurately achieve
the desired postoperative TPA without inadvertently creating angular or rotational limb
deformities involves a complex interplay of factors. Intra- and interobserver variability in TPA
assessment has the potential to influence preoperative planning and subsequent postoperative
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
217
Surgical Treatment
VetBooks.ir
218
Pre-op
Post-op
(A)
TPA. Interobserver variability in TPA measurement has been shown to be relatively small
(standard deviation of 0.8◦ ) but significant,
whereas intraobserver variability and between
groups of observers was not statistically significant (Caylor et al. 2001; Fettig et al. 2003).
Measurement variability in the TPA is reduced
when digital radiography and computerized measurement systems are used (Unis
et al. 2010). While the stifle flexion angle has
been shown to not influence TPA measurement
(Aulakh et al. 2011), limb position does influence
radiographic TPA measurement. Cranial and
proximal positioning of the limb relative to the
X-ray beam results in overestimation, whereas
caudal and distal positioning results in underestimation of the TPA (Reif et al. 2004). Both
preoperative and intraoperative planning of the
osteotomy position improves the likelihood of a
more centered osteotomy, and reduces the risk
of tibial tuberosity fractures (Collins et al. 2014).
When planning techniques were compared,
measuring the distance from the insertion
point of the patella tendon to two points on the
proposed osteotomy line (perpendicular to the
cranial border of the tibial crest and at the joint
surface) proved the most accurate (Mossman
et al. 2015). An emphasis on osteotomy reduction at the expense of medial cortex alignment
minimizes angular and rotational deformities due to TPLO (Wheeler et al. 2003). Distal
(B)
Figure 27.1 Schematic drawing
depicting the reduction in tibial
plateau angle following a tibial
plateau leveling osteotomy and
the subsequent change in
individual tibiofemoral forces.
(A) The tibiofemoral forces are
broken down into a
perpendicular and a parallel
force relative to the tibial plateau
(blue arrows). The force parallel
to the tibial plateau represents
tibial femoral shear. (B) With
rotation of the tibial plateau note
the elimination of tibial femoral
shear. The resultant compressive
force remains unchanged and is
represented by the white arrow
in both A and B. Source:
Boudrieau 2009. Reproduced
with permission from John Wiley
& Sons, Inc.
positioning of the osteotomy (versus centering
on the proximal tibial long axis point dividing the intercondylar tubercles) results in a
postoperative TPA greater than is expected. In
addition, undesired craniodistal translation of
the tibial plateau and tibial long axis shift is
noted (Kowaleski et al. 2005).
In the original surgical technique as described
by Slocum, an alignment jig is secured to the
tibia with the goal of maintaining a fixed plane
during proximal segment rotation. The necessity for a jig for TPLO has been questioned
by some authors. One study found no significant differences in postsurgical TPA, tibial crest
thickness, varus–valgus malalignment, or tibial torsion between TPLOs performed with or
without a jig (Bell & Ness 2007). The same
authors found that the use of a jig resulted in
a more distally positioned osteotomy. Another
group found no significant difference in postsurgical TPA, fragment reduction, or proximodistal osteotomy orientation when a jig was
not used, as long as the limb was held in 10–
15◦ of internal rotation and parallel to horizontal while performing a vertically oriented
osteotomy (Schmerbach et al. 2007). A third
group showed that fibular penetration by screw
tip is more likely when a jig is not utilized
(Flynn et al. 2014). With the recent development
of a novel jig and saw guide (Mariano et al.
2016), current studies have shown improved
VetBooks.ir
Tibial Plateau Leveling Osteotomy
accuracy of osteotomy placement over the previous jig model (Burton et al. 2013; Tan et al.
2014).
TPLO reportedly eliminates the wedge effect
of the medial meniscus, which may protect it
from postoperative injury (Pozzi et al. 2006).
Hence, the necessity for medial meniscal release
during TPLO has been debated and appears to
be related to the quality of intraoperative meniscal evaluation. A subsequent meniscal tear is
3.8-fold more likely to occur when meniscal
evaluation is performed via an arthrotomy and
no meniscal release is performed, as compared
to either meniscal evaluation via an arthroscopy
with no release or meniscal evaluation via
arthrotomy with a release performed (Thieman
et al. 2006). Importantly, although TPLO eliminates dynamic craniocaudal stifle instability
and may impart protection to the medial meniscus, it fails to restore normal femorotibial contact mechanics. Postoperative femorotibial contact areas are significantly smaller than normal,
with higher peak contact pressures (Kim et al.
2009).
Patient selection
Appropriate case selection is important to the
success of TPLO. TPLO results in an increased
strain on the CaCL ligament. Therefore, patients
with a compromised CaCL are not candidates
for the procedure (Warzee et al. 2001). While this
surgery is most commonly performed on largebreed dogs (Duerr et al. 2014), patients as small
as a cat (Hoots & Petersen 2005) and as large as
a llama (Ray et al. 2004) have been successfully
treated with TPLO. Patient size in itself is not a
concern, as long as appropriately sized implants
are chosen for the procedure. With the continued introduction of smaller implants, TPLO is
quickly becoming more common in small-breed
dogs (Witte & Scott 2014; Cosenza et al. 2015).
It is important to note that the morphology of
the proximal tibia differs between large- and
small-breed dogs, with small-breed dogs generally having a larger TPA (Vedrine et al. 2013;
Aertsens et al. 2015).
Anecdotally, TPLO has been advocated in
cases with a lack of cranial drawer where
partial CR is suspected as a means to decrease
the biomechanical strain on the CrCL and
219
theoretically protect it from further damage.
Research now supports this recommendation
with three studies. Haynes et al. (2015) showed
that decreasing the TPA will decrease strain in
the intact CrCL. Hulse et al. (2010) reported normal to near-normal intra-articular structures
on second-look arthroscopic examination of
stifles with stable partial CR treated with TPLO,
while joints with full ruptures showed a range
of pathologic changes. At long-term clinical
follow-up in a small case series, progression of
osteoarthritis appeared reduced with ongoing
preservation of passive stability (Barger et al.
2016).
TPLO implant selection
A wide range of orthopaedic implant manufacturers produce commercially available TPLO
implants in a growing variety of sizes. Both
locking and non-locking implants are available (Figures 27.2 and 27.3). A biomechanical
comparison between three different commercial manufacturer’s TPLO plates has been performed in an axially loaded gap model: Synthes TPLO plate (Synthes Vet, West Chester, PA,
USA)/tibia constructs were found to be significantly stiffer than Slocum TPLO plate (Slocum
Enterprises, Inc., Eugene, OR, USA)/tibia constructs, which were found to be not significantly
different than Securos TPLO plate (Securos,
Fiskdale, MA, USA)/tibia constructs (Kloc et al.
2009). Notably, the Synthes TPLO implant used
in the above study was a locking bone plate,
whereas the Slocum and Securos implants were
conventional (non-locking) bone plates.
The use of locking bone screws causes
significantly less translational movement of
the proximal tibial segment towards the bone
plate compared to the use of conventional bone
screws in an identical plate. However, no significant difference exists between locking and conventional screw constructs in mean stiffness or
cycles to failure under load-sharing conditions
(Leitner et al. 2008). Mechanical testing between
non-locking and locking plates in an osteotomy
gap model showed that locking plates have a
higher load to failure, with the broad locking
plate having both a higher load to failure and a
greater mean stiffness (Bordelon et al. 2009). A
retrospective evaluation of change in TPA
Surgical Treatment
VetBooks.ir
220
(A)
(B)
(C)
Figure 27.2 Example of four
commercial manufacturer’s
tibial plateau leveling osteotomy
plates. (A) Synthes 3.5 mm. (B)
Arthrex 3.5 mm. (C) New
Generation Devices 3.5 mm. (D)
New Generation Devices
3.5 mm Broad. Plates shown in
panels A and B do not require
contouring.
(D)
(D)
(C)
3.5
(B)
(A)
2.7
2.4
2.0
Figure 27.3 Example of TPLO plate sizes. Synthes 2.0 mm, 2.4 mm, 2.7 mm, (A) 3.5 mm compact, (B) 3.5 mm
standard, (C) 3.5 mm broad, (D) Veterinary Orthopedic Implants 3.5 mm Jumbo.
VetBooks.ir
Tibial Plateau Leveling Osteotomy
during bone healing and radiographic
osteotomy stability showed no difference
between non-locking and locking plates
(Krotscheck et al. 2012), while a similar prospective study concluded that locking screw fixation
increases the stabilization of TPA during healing and provides improved radiographic
evidence of osteotomy healing (Conkling et al.
2010). The use of a locking plate construct
is also associated with a lower incidence of
infection and a lower general complication rate
(Kowaleski et al. 2013; Solano et al. 2015).
Concerns related to the use of the original
Slocum TPLO plate center around plate corrosion in vivo with the subsequent generation of
chemical species that have the potential to cause
disease, the presence of plate magnetism, and
findings showing the plate to be a cast stainless steel implant (Boudrieau et al. 2006; Charles
& Ness 2006). Furthermore, Slocum TPLO
implant-associated sarcoma has been reported
(Boudrieau et al. 2005). Metallurgical analysis of
alternative TPLO implants by an independent,
unbiased party is currently lacking.
Complications after TPLO
The overall postoperative complication rate of
TPLO has been reported to vary from 7.2%
to 28% (Pacchiana et al. 2003; Priddy et al.
2003; Stauffer et al. 2006; Fitzpatrick & Solano
2010; Gatineau et al. 2011; Oxley et al. 2013;
Coletti et al. 2014). Factors associated with
the development of complications include tibial plateau angle >30◦ , increased body weight,
and complete versus partial CR (Fitzpatrick
& Solano 2010; Coletti et al. 2014). A higher
complication rate has also been reported in
dogs undergoing simultaneous bilateral TPLO
(Priddy et al. 2003). Notably, most complications can be resolved without surgical intervention (Pacchiana et al. 2003). Examples of complications include hemorrhage, poor incision site
healing, patellar tendon enlargement, fractures
involving the fibula or tibia, subsequent meniscal injury, implant failures and infection.
Infection rates for TPLO average around
4.6% (Bergh & Peirone 2012), which is higher
than expected for a clean surgical procedure. Theoretically, postoperative administration of antimicrobials is not indicated for clean
221
surgeries, but numerous studies have shown
that postoperative antibiotic therapy does provide a protective affect against surgical site
infection in TPLO (Fitzpatrick & Solano 2010;
Frey et al. 2010; Nazarali et al. 2014; Nazarali
et al. 2015; Solano et al. 2015). If treated appropriately, no association is seen between surgical
site infection and long-term functional outcome
(Brown et al. 2016).
Dogs with a preoperative TPA ≥35◦ have
a higher incidence of postoperative complications, with a loss of postoperative TPA or
‘rockback’ during the convalescent period being
the most common. The addition of ancillary
implants to TPLO significantly reduces the incidence of this problem (Duerr et al. 2008). A combination of TPLO with a closing cranial wedge
ostectomy has been suggested as one possible means of addressing excessive TPA (Talaat
et al. 2006). Small losses of postoperative TPA of
about 1.5◦ during the convalescent period have
been documented in the face of apparently stable implant fixation, and by themselves do not
appear to have any deleterious effects on clinical outcome (Moeller et al. 2006; Hurley et al.
2007).
Radiographic evidence of patellar tendon
enlargement is a common finding after TPLO,
with up to 80% of clinical cases showing evidence of moderate to severe thickening at
2 months postoperatively (Carey et al. 2005)
(Figure 27.4). Despite this finding, only 7%
of the dogs in this study displayed clinical
signs of patellar tendinosis, with most dogs
improving with medical management. Patellar femoral joint kinematics are altered by
TPLO, and this may be a predisposing factor
to patellar tendinosis (Pozzi et al. 2013). Patella
fracture after TPLO is a rare complication
(0.25–2%) that has been associated with radiographic evidence of patellar tendon thickening
(Pacchiana et al. 2003; Carey et al. 2005; Gatineau
et al. 2011; Rutherford et al. 2014). Non-surgical
management generally provides a satisfactory
outcome.
Dogs that are cranial tibial thrust-negative
immediately after surgery occasionally become
thrust-positive after surgery. Affected dogs
often have poor limb function and pivot shift on
ambulation. Pivot shift is created by a combination of cranial translation of the tibia with internal rotation of the stifle. The mechanism for this
Surgical Treatment
VetBooks.ir
222
Figure 27.4 Lateral view radiograph of a dog 8 weeks
after tibial plateau leveling osteotomy, demonstrating
marked thickening of the patellar tendon (white arrows).
(A)
(B)
complication is unclear and is more commonly
identified in heavily muscled dogs with genu
varum conformation. Most cases improve with
aggressive physical therapy. However, a lateral
fabellar imbrication suture or a femoral corrective osteotomy may be required in severe cases.
Fractures of the fibula or tibia are potentially more serious complications that may be
encountered during or after the TPLO procedure (Figure 27.5). Fibular fractures occurred in
5.4% of cases in a series of 168 TPLO procedures,
with identified risk factors including increased
body weight, greater preoperative TPA, greater
change in TPA, and TPLO performed without
the use of a jig (Tuttle & Manley 2009). A subsequent study by Taylor et al. (2011) of 355 TPLO
cases reported a 15% fibula fracture rate, with
increased body weight and an unfilled fibular
drill hole identified as risk factors. Risk factors
for tibial tuberosity fracture after TPLO include
simultaneous bilateral TPLO, a thinner postoperative mean thickness of the tibial tuberosity,
and an increase in TPA during convalescence
(Kergosien et al. 2004; Bergh et al. 2008).
The use of a structured postoperative physiotherapy program has been shown to result
in a greater stifle range of motion (ROM)
for dogs undergoing TPLO at 3 and 6 weeks
postoperatively, and greater likelihood of full
Figure 27.5 Cranial-caudal (A)
and lateral (B) radiographic
views of a dog 10 weeks after
tibial plateau leveling osteotomy,
showing a short oblique proximal
fibular fracture (white arrows).
VetBooks.ir
Tibial Plateau Leveling Osteotomy
function at 8 weeks, as compared to standard
home-exercise-restricted dogs (Monk et al. 2006;
Romano & Cook 2015). This highlights the
importance of postoperative physiotherapy, as
a loss of ≥10◦ ROM has been associated with
significantly higher subjective clinical lameness
scores than dogs with <10◦ ROM loss. Loss of
extension is also correlated with osteoarthritis
(OA) in the cranial femorotibial joint (Jandi &
Shulman 2007). Although progression of OA
occurs after TPLO (Boyd et al. 2007; Hurley et al.
2007), in general the presence of stifle OA correlates poorly with clinical function (Gordon et al.
2003).
223
TPLO evaluated via force platform gait analysis
preoperatively and ≥4 months postoperatively,
found no relationship between postoperative
TPA (range 0–14◦ ) and postoperative ground
reaction forces (Robinson et al. 2006). Client satisfaction with postoperative outcomes of TPLO
in both large- and small-breed dogs has been
reported as very good in multiple studies, even
though such subjective assessments often do
not correlate with the incidence of postoperative complications or objective measures of limb
function (Priddy et al. 2003; Talaat et al. 2006;
Thieman et al. 2006; Boyd et al. 2007; Waxman
et al. 2008; Christopher et al. 2013; Gordon-Evans
et al. 2013; Berger et al. 2015).
Outcome after TPLO
Despite these potential complications, outcome
after TPLO has been reported as favorable
in subjective and objective studies in both
large- and small-breed dogs. Subjective studies employed clinical assessments such as lameness scoring, radiographic osteophyte scoring,
and client questionnaires (Kergosien et al. 2004;
Stauffer et al. 2006; Thiemann et al. 2006; Boyd
et al. 2007; Christopher et al. 2013). The objective evaluation of limb use after TPLO via
force plate and kinematic analysis has corroborated the observation that recovery after TPLO
is rapid in the early stages, particularly when
compared to lateral fabello-tibial suture stabilization (de Medeiros et al. 2011; Böddeker
et al. 2012). Very good long-term outcome is
seen in large breeds after TPLO, with improvement of ground reaction forces comparable to
(Conzemius et al. 2005; Millis et al. 2008) or
greater than lateral fabello-tibial suture stabilization (Gordon-Evans et al. 2013; Nelson et al.
2013). Improvement in ground reaction forces
greater than lateral fabello-tibial suture stabilization is also seen in small-breed dogs with
TPLO (Berger et al. 2015). A meta-analysis of
the literature on surgical treatments for CR by
Bergh et al. (2014) concluded that the evidence
evaluated strongly supports TPLO in its ability
to return dogs to normal function.
While ex vivo studies (Warzee et al. 2001)
have demonstrated that a postoperative TPA
of 6.5 ± 0.9◦ neutralizes cranial tibial thrust,
a study of 32 client-owned Labrador Retrievers with naturally occurring CR undergoing
Conclusions
TPLO is an important surgical stabilization
technique with documented short- and longterm favorable outcomes in both large- and
small-breed dogs.
References
Aertsens A, Rincon Alvarez J, Poncet CM, et al. Comparison of the tibia plateau angle between small
and large dogs with cranial cruciate ligament disease. Vet Comp Orthop Traumatol 2015;28:385–390.
Aulakh KS, Harper TA, Lanz OI, et al. Effect of stifle
angle on the magnitude of the tibial plateau angle
measurement in dogs with intact and transected
cranial cruciate ligament. A cadaveric study. Vet
Comp Orthop Traumatol 2011;24:272–278.
Barger B, Piazza A, Muir P. Treatment of stable partial
cruciate rupture (Grade I sprain) in five dogs with
tibial plateau levelling osteotomy. Vet Rec Case Rep
2016;4:e000315.
Berger B, Knebel J, Steigmeier-Raith S, et al. Longterm outcome after surgical treatment of cranial
cruciate ligament rupture in small breed dogs.
Comparison of tibial plateau leveling osteotomy
and extra-articular stifle stabilization. Tierarztl
Prax Ausg K Kleintiere Heimtiere 2015;43:373–380.
Bell JC, Ness MG. Does use of a jig influence the precision of tibial plateau leveling osteotomy surgery?
Vet Surg 2007;36:228–233.
Bergh MS, Peirone B. Complications of tibial plateau
levelling osteotomy in dogs. Vet Comp Orthop
Traumatol 2012;25:349–358.
Bergh MS, Rajala-Schultz P, Johnson KA. Risk factors
for tibial tuberosity fracture after tibial plateau leveling osteotomy in dogs. Vet Surg 2008;37:374–382.
VetBooks.ir
224
Surgical Treatment
Bergh MS, Sullivan C, Ferrell CL, et al. Systematic
review of surgical treatments for cranial cruciate
ligament disease in dogs. J Am Anim Hosp Assoc
2014;50:315–321.
Böddeker J, Drüen S, Meyer-Lindenberg A, et al.
Computer-assisted gait analysis of the dog: comparison of two surgical techniques for the ruptured
cranial cruciate ligament. Vet Comp Orthop Traumatol 2012;25:11–21.
Bordelon J, Coker D, Payton M, et al. An in vitro
mechanical comparison of tibial plateau levelling
osteotomy plates. Vet Comp Orthop Traumatol
2009;22:467–472.
Boudrieau RJ, McCarthy RJ, Sisson RD Jr. Sarcoma of
the proximal portion of the tibia in a dog 5.5 years
after tibial plateau leveling osteotomy. J Am Vet
Med Assoc 2005;227:1613–1617.
Boudrieau RJ, McCarthy RJ, Sprecher CM, et al. Material properties of and tissue reaction to the Slocum
TPLO plate. Am J Vet Res 2006;67:1258–1265.
Boudrieau RJ. Tibial plateau leveling osteotomy or
tibial tuberosity advancement? Vet Surg 2009;38:1–
22.
Boyd DJ, Miller CW, Etue SM, et al. Radiographic
and functional evaluation of dogs at least 1 year
after tibial plateau leveling osteotomy. Can Vet J
2007;48:392–396.
Burton NJ, Fitzpatrick N, Wallace AM. Evaluation
of cut accuracy and cis cortical damage for tibial plateau leveling osteotomy performed with and
without aid of a novel saw guide: an in vitro study.
Vet Surg 2013;42:28–37.
Brown G, Maddox T, Baglietto Siles MM. Clientassessed long-term outcome in dogs with surgical site infection following tibial plateau levelling
osteotomy. Vet Rec 2016;179:409.
Carey K, Aiken SW, DiResta GR, et al. Radiographic
and clinical changes of the patellar tendon after
tibial plateau leveling osteotomy 94 cases (2000–
2003). Vet Comp Orthop Traumatol 2005;18:235–
242.
Caylor KB, Zumpano CA, Evans LM, et al. Intraand interobserver measurement variability of tibial plateau slope from lateral radiographs in dogs.
J Am Anim Hosp Assoc 2001;37:263–268.
Charles AE, Ness MG. Crevice corrosion of implants
recovered after tibial plateau leveling osteotomy in
dogs. Vet Surg 2006;35:438–444.
Christopher SA, Beetem J, Cook JL. Comparison of
long-term outcomes associated with three surgical
techniques for treatment of cranial cruciate ligament disease in dogs. Vet Surg 2013;42:329–334.
Coletti TJ, Anderson M, Gorse MJ, et al. Complications associated with tibial plateau leveling
osteotomy: a retrospective of 1519 procedures. Can
Vet J 2014;55:249–254.
Collins JE, Degner DA, Hauptman JG, et al. Benefits of
pre- and intraoperative planning for tibial plateau
leveling osteotomy. Vet Surg 2014;43:142–149.
Conkling AL, Fagin B, Daye RM. Comparison of tibial plateau angle changes after tibial plateau leveling osteotomy fixation with conventional or locking screw technology. Vet Surg 2010;39:475–481.
Cosenza G, Reif U, Martini FM. Tibial plateau levelling osteotomy in 69 small breed dogs using conically coupled 1.9/2.5 mm locking plates. A clinical and radiographic retrospective assessment. Vet
Comp Orthop Traumatol 2015;28:347–354.
Conzemius MG, Evans RB, Besancon MF, et al. Effect
of surgical technique on limb function after surgery
for rupture of the cranial cruciate ligament in dogs.
J Am Vet Med Assoc 2005;226:232–236.
de Medeiros M, Sánchez Bustinduy M, Radke H, et al.
Early kinematic outcome after treatment of cranial
cruciate ligament rupture by tibial plateau levelling
osteotomy in the dog. Vet Comp Orthop Traumatol
2011;24:178–184.
Drygas KA, Pozzi A, Goring RL, et al. Effect of tibial plateau leveling osteotomy on patellar tendon
angle: a radiographic cadaveric study. Vet Surg
2010;39:418–424.
Duerr FM, Duncan CG, Savicky RS, et al. Comparison
of surgical treatment options for cranial cruciate
ligament disease in large-breed dogs with excessive tibial plateau angle. Vet Surg 2008;37:49–62.
Duerr FM, Martin KW, Rishniw M, et al. Treatment of
canine cranial cruciate ligament disease. A survey
of ACVS Diplomates and primary care veterinarians. Vet Comp Orthop Traumatol 2014;27:478–483.
Fettig AA, Rand WM, Sato AF, et al. Observer variability of tibial plateau slope measurement in 40
dogs with cranial cruciate ligament-deficient stifle
joints. Vet Surg 2003;32:471–478.
Fitzpatrick N, Solano MA. Predictive variables for
complications after TPLO with stifle inspection
by arthrotomy in 1000 consecutive dogs. Vet Surg
2010;39:460–474.
Flynn P, Duncan CG, Palmer RH, et al. In vitro
incidence of fibular penetration with and without the use of a jig during tibial plateau leveling
osteotomy. Vet Surg 2014;43:495–499.
Frey TN, Hoelzler MG, Scavelli TD, et al. Risk factors for surgical site infection-inflammation in dogs
undergoing surgery for rupture of the cranial
cruciate ligament: 902 cases (2005–2006). J Am Vet
Med Assoc 2010;236:88–94.
Gatineau M, Dupuis J, Planté J, et al. Retrospective
study of 476 tibial plateau levelling osteotomy procedures. Rate of subsequent ‘pivot shift’, meniscal tear and other complications. Vet Comp Orthop
Traumatol 2011;24:333–341.
Gordon WJ, Conzemius MG, Riedesel E, et al.
The relationship between limb function and
radiographic osteoarthrosis in dogs with stifle
osteoarthrosis. Vet Surg 2003;32:451–454.
Gordon-Evans WJ, Griffon DJ, Bubb C, et al. Comparison of lateral fabellar suture and tibial plateau leveling osteotomy techniques for treatment of dogs
VetBooks.ir
Tibial Plateau Leveling Osteotomy
with cranial cruciate ligament disease. J Am Vet
Med Assoc 2013;243:675–680.
Haynes KH, Biskup J, Freeman A, et al. Effect of tibial
plateau angle on cranial cruciate ligament strain: an
ex vivo study in the dog. Vet Surg 2015;44:46–49.
Hoots EA, Petersen SW. Tibial plateau leveling
osteotomy and cranial closing wedge ostectomy in
a cat with cranial cruciate ligament rupture. J Am
Anim Hosp Assoc 2005;41:395–399.
Hulse D, Beale B, Kerwin S. Second look arthroscopic
findings after tibial plateau leveling osteotomy. Vet
Surg 2010;39:350–354.
Hurley CR, Hammer DL, Shott S. Progression of
radiographic evidence of osteoarthritis following
tibial plateau leveling osteotomy in dogs with cranial cruciate ligament rupture: 295 cases (2001–
2005). J Am Vet Med Assoc 2007;230:1674–1679.
Jandi AS, Shulman AJ. Incidence of motion loss of
the stifle joint in dogs with naturally occurring cranial cruciate ligament rupture surgically treated
with tibial plateau leveling osteotomy: longitudinal clinical study of 412 cases. Vet Surg 2007;36:114–
121.
Kergosien DH, Barnhart MD, Kees CE, et al. Radiographic and clinical changes of the tibial tuberosity after tibial plateau leveling osteotomy. Vet Surg
2004;33:468–474.
Kim SE, Pozzi A, Banks SA, et al. Effect of tibial
plateau leveling osteotomy on femorotibial contact mechanics and stifle kinematics. Vet Surg
2009;38:23–32.
Kloc PA, Kowaleski MP, Litsky AS, et al. Biomechanical comparison of two alternative tibial plateau leveling osteotomy plates with the original standard
in an axially loaded gap model: an in vitro study.
Vet Surg 2009;38:40–48.
Kowaleski MP, Apelt D, Mattoon JS, et al. The effect
of tibial plateau leveling osteotomy position on cranial tibial subluxation: an in vitro study. Vet Surg
2005;34:332–326.
Kowaleski MP, Boudrieau RJ, Beale BS, et al.
Radiographic outcome and complications of tibial plateau leveling osteotomy stabilized with an
anatomically contoured locking bone plate. Vet
Surg 2013;42:847–852.
Krotscheck U, Thompson MS, Ryan KK, et al. Comparison of TPA, bone healing, and intra-articular
screw placement using conventional nonlocked
application of surgeon-contoured versus locked
application of precontoured TPLO plates in dogs.
Vet Surg 2012;41:931–937.
Leitner M, Pearce SG, Windolf M, et al. Comparison of locking and conventional screws for maintenance of tibial plateau positioning and biomechanical stability after locking tibial plateau leveling osteotomy plate fixation. Vet Surg 2008;37:357–
365.
Mariano AD, Kowaleski MP, Boudrieau RJ. Novel
TPLO alignment jig/saw guide reproduces free-
225
hand and ideal osteotomy positions. PLoS One
2016;11:e0161110.
Millis D, Durant A, Headrick J, et al. Long term kinetic
and kinematic comparison of cruciate-deficient
dogs treated with tibial plateau leveling osteotomy
or modified retinacular imbrications technique. Vet
Surg 2008;37:E23.
Moeller EM, Cross AR, Rapoff AJ. Change in tibial plateau angle after tibial plateau leveling
osteotomy in dogs. Vet Surg 2006;35:460–464.
Monk ML, Preston CA, McGowan CM. Effects
of early intensive postoperative physiotherapy
on limb function after tibial plateau leveling
osteotomy in dogs with deficiency of the cranial
cruciate ligament. Am J Vet Res 2006;67:529–536.
Mossman H, von Pfeil DJ, Nicholson M, et al. Accuracy of three pre- and intra-operative measurement
techniques for osteotomy positioning in the tibial plateau levelling procedure. Vet Comp Orthop
Traumatol 2015;28:250–255.
Nazarali A, Singh A, Moens NM, et al. Association
between methicillin-resistant Staphylococcus pseudintermedius carriage and the development of surgical site infections following tibial plateau leveling osteotomy in dogs. J Am Vet Med Assoc
2015;247:909–916.
Nazarali A, Singh A, Weese JS. Perioperative administration of antimicrobials during tibial plateau leveling osteotomy. Vet Surg 2014;43:966–971.
Nelson SA, Krotscheck U, Rawlinson J, et al. Longterm functional outcome of tibial plateau leveling
osteotomy versus extracapsular repair in a heterogeneous population of dogs. Vet Surg 2013;42:38–
50.
Oxley B, Gemmill TJ, Renwick AR, et al. Comparison
of complication rates and clinical outcome between
tibial plateau leveling osteotomy and a modified
cranial closing wedge osteotomy for treatment of
cranial cruciate ligament disease in dogs. Vet Surg
2013;42:739–750.
Pacchiana PD, Morris E, Gillings SL, et al. Surgical and
postoperative complications associated with tibial
plateau leveling osteotomy in dogs with cranial
cruciate ligament rupture: 397 cases (1998–2001).
J Am Vet Med Assoc 2003;222:184–193.
Pozzi A, Dunbar NJ, Kim SE. Effect of tibial plateau
leveling osteotomy on patellofemoral alignment:
a study using canine cadavers. Vet J 2013;198:98–
102.
Pozzi A, Kowaleski MP, Apelt D, et al. Effect of medial
meniscal release on tibial translation after tibial
plateau leveling osteotomy. Vet Surg 2006;35:486–
494.
Priddy NH, Tomlinson JL, Dodam JR, et al. Complications with and owner assessment of the outcome
of tibial plateau leveling osteotomy for treatment of
cranial cruciate ligament rupture in dogs: 193 cases
(1997–2001). J Am Vet Med Assoc 2003;222:1726–
1732.
VetBooks.ir
226
Surgical Treatment
Ray WM, Gustafson SB, Huber MJ. Tibial plateau
leveling osteotomy in a llama with a ruptured
cranial cruciate ligament. J Am Vet Med Assoc
2004;225:1739–1742.
Reif U, Dejardin LM, Probst CW, et al. Influence of
limb positioning and measurement method on the
magnitude of the tibial plateau angle. Vet Surg
2004;33:368–375.
Reif U, Hulse DA, Hauptman JG. Effect of tibial
plateau leveling on stability of the canine cranial
cruciate-deficient stifle joint: an in vitro study. Vet
Surg 2002;31:147–154.
Robinson DA, Mason DR, Evans R, et al. The effect
of tibial plateau angle on ground reaction forces 4–
17 months after tibial plateau leveling osteotomy in
Labrador Retrievers. Vet Surg 2006;35:294–299.
Romano LS, Cook JL. Safety and functional outcomes associated with short-term rehabilitation
therapy in the post-operative management of tibial
plateau leveling osteotomy. Can Vet J 2015;56:942–
946.
Rutherford S, Bell J, Ness M. Fracture of the patella
after TPLO in dogs. Vet Surg 2014;43:523–524.
Sathya S, Gilbert P, Sharma A, et al. Effect of tibial plateau levelling osteotomy on patellar tendon angle: a prospective clinical study. Vet Comp
Orthop Traumatol 2014;27:346–350.
Schmerbach KI, Boeltzig CK, Reif U, et al. In vitro comparison of tibial plateau leveling osteotomy with
and without use of a tibial plateau leveling jig. Vet
Surg 2007;36:156–163.
Slocum B, Slocum TD. Tibial plateau leveling
osteotomy for repair of cranial cruciate ligament
rupture in the canine. Vet Clin North Am Small
Anim Pract 1993;23:777–795.
Solano MA, Danielski A, Kovach K, et al. Locking
plate and screw fixation after tibial plateau leveling osteotomy reduces postoperative infection rate
in dogs over 50 kg. Vet Surg 2015;44:59–64.
Stauffer KD, Tuttle TA, Elkins AD, et al. Complications associated with 696 tibial plateau leveling
osteotomies (2001–2003). J Am Anim Hosp Assoc
2006;42:44–50.
Talaat MB, Kowaleski MP, Boudrieau RJ. Combination tibial plateau leveling osteotomy and cranial closing wedge osteotomy of the tibia for the
treatment of cranial cruciate ligament-deficient sti-
fles with excessive tibial plateau angle. Vet Surg
2006;35:729–739.
Tan CJ, Bergh MS, Schembri MA, et al. Accuracy
of tibial osteotomy placement using 2 different
tibial plateau leveling osteotomy jigs. Vet Surg
2014;43:525–533.
Taylor J, Langenbach A, Marcellin-Little DJ. Risk
factors for fibular fracture after TPLO. Vet Surg
2011;40:687–693.
Thieman KM, Tomlinson JL, Fox DB, et al. Effect of
meniscal release on rate of subsequent meniscal
tears and owner-assessed outcome in dogs with
cruciate disease treated with tibial plateau leveling
osteotomy. Vet Surg 2006;35:705–710.
Tuttle TA, Manley PA. Risk factors associated
with fibular fracture after tibial plateau leveling
osteotomy. Vet Surg 2009;38:355–360.
Unis MD, Johnson AL, Griffon DJ, et al. Evaluation of
intra- and interobserver variability and repeatability of tibial plateau angle measurements with digital radiography using a novel digital radiographic
program. Vet Surg 2010;39:187–194.
Vedrine B, Guillemot A, Fontaine D, et al. Comparative anatomy of the proximal tibia in healthy
Labrador Retrievers and Yorkshire Terriers. Vet
Comp Orthop Traumatol 2013;26:266–70.
Warzee CC, Dejardin LM, Arnoczky SP, et al. Effect
of tibial plateau leveling on cranial and caudal tibial thrusts in canine cranial cruciate deficient stifles.
Vet Surg 2001;30:278–286.
Waxman AS, Robinson DA, Evans RB, et al. Relationship between objective and subjective assessment
of limb function in normal dogs with an experimentally induced lameness. Vet Surg 2008;37:241–
246.
Wheeler JL, Cross AR, Gingrich W. In vitro effects
of osteotomy angle and osteotomy reduction on
tibial angulation and rotation during the tibial
plateau-leveling osteotomy procedure. Vet Surg
2003;32:371–377.
Windolf M, Leitner M, Schwieger K, et al. Accuracy
of fragment positioning after TPLO and effect on
biomechanical stability. Vet Surg 2008;37:366–373.
Witte PG, Scott HW. Tibial plateau leveling
osteotomy in small breed dogs with high tibial plateau angles using a 4-hole 1.9/2.5 mm
locking T-plate. Vet Surg 2014;43:549–557.
VetBooks.ir
28
Tibial Tuberosity Advancement
Randy J. Boudrieau
Introduction
Advancement of tibial tuberosity was first
described by Maquet, where the premise of
the procedure was that an increase in the
efficiency of the quadriceps mechanism would
subsequently decrease retropatellar pressure,
thus alleviating pain associated with the
patellofemoral joint in humans (Maquet 1976).
Other possible effects on the biomechanics of
the tibiofemoral joint included evidence that a
variable tibiofemoral shear force was present
in the knee joint, which was directed either
anteriorly or posteriorly depending upon
the angle of knee joint extension or flexion
and patellar tendon angle (PTA), respectively
(Nisell 1985), and that the magnitude and
direction of the tibiofemoral shear force was
determined by the PTA (Nisell et al. 1986)
(Figure 28.1). An increase in translational knee
joint instability has been demonstrated by a
number of biomechanical studies in humans
as a result of variations in tibial plateau slope
(Giffin et al. 2004), axial loading (Li et al. 1998),
and knee flexion angle (Nisell et al. 1989). A
three-dimensional (3D) nonlinear finite element model of the human knee evaluating the
Maquet procedure found it to be effective in
decreasing the femorotibial contact forces in
stifle joint extension, in addition to decreasing
retropatellar pressure (Shirazi-Adl & Mesfar
2007). Similarly, changes in tibiofemoral shear
forces were observed depending on the knee
flexion angle, which placed either more or less
stress on the anterior and posterior cruciate
ligaments depending on the amount of tibial
tuberosity advancement (Shirazi-Adl & Mesfar
2007). A relationship between tibial tuberosity
advancement, knee joint flexion/extension,
tibiofemoral shear force, retropatellar pressure,
femorotibial contact forces, and patellar tendon
force has been suggested and supported by a
variety of experimental studies (Maquet 1976;
Nakamura et al. 1985; Nisell 1985; Nisell et al.
1986; Nisell et al. 1989; Li et al. 1998; Giffin et al.
2004; Shirazi-Adl & Mesfar 2007).
Stifle biomechanics
Based on data published by Maquet and Nisell,
Montavon and Tepic proposed that a similar situation existed in the dog, and tibial tuberosity
advancement (TTA) would similarly neutralize cranial tibiofemoral shear force in a cranial
cruciate ligament (CrCL)-deficient stifle joint in
the dog (Maquet 1976; Nisell et al. 1986; Montavon et al. 2002; Tepic et al. 2002). A PTA of 90◦
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
227
VetBooks.ir
228
Surgical Treatment
(A)
Fp
Knee
Angle
TPS
PTA
PTA
(B)
120°
110°
100°
60°
90°
180°
80°
150°
120°
90°
Knee Angle
Fs (N)
(C)
600
was suggested as the crossover point at 135◦ of
stifle joint extension; thus, the TTA technique
was developed so as to achieve this PTA (Figure 28.2). These assumptions were supported in
four experimental ex vivo models (Apelt et al.
2007; Miller et al. 2007; Kipfer et al. 2008; Hoffmann et al. 2011). These models were used to
evaluate cranial tibiofemoral shear force either
indirectly with cranial tibial subluxation (Apelt
et al. 2007; Miller et al. 2007; Kipfer et al. 2008)
or directly with cranial tibial thrust under varying loading conditions (Hoffmann et al. 2011)
(Figure 28.3). A recent 3D quasi-static rigid
body pelvic limb computer model simulating
the stance phase of gait predicted improved
joint loading in the CrCL-deficient stifle, but not
restoration of normal CrCL-intact biomechanics (Brown et al. 2015). In this model, the TTA
effectively reduced tibial translation, but did
not stabilize tibial rotation (Brown et al. 2015).
These results were similar whether using either
the tibial plateau angle (TPA) or common tangent planning methods to achieve a target PTA
of 90◦ (Brown et al. 2015). The findings in this
model were consistent with an in vivo assessment of the TTA during weight-bearing, which
demonstrated that craniotibial translation was
reduced, but not eliminated (Skinner et al. 2013).
A 3D nonlinear joint finite element model
reconstruction, which was based on a cadaver
knee joint of a human, was used to evaluate the reduction in retropatellar pressure and
patellar tendon force. The analysis confirmed
not only a decrease in patellofemoral contact
forces after TTA, but also femorotibial contact
forces with stifle joint extension (Shirazi-Adl &
400
200
90°
60°
0
180°
–200
150°
120°
Knee Angle
Figure 28.1 (A) Anatomic landmarks of the radiographic
and morphologic studies of the knee. The patellar tendon
force (Fp) is shown, which is approximately of the same
magnitude and direction of the tibiofemoral compressive
force, and results in a variable amount of tibiofemoral
shear force depending on the knee flexion angle and
tibial plateau slope (TPS), both of which influence the
patellar tendon angle (PTA). (B) The relationship between
Figure 28.1 (Continued) the PTA (y-axis) and knee
flexion angle (x-axis); note that the PTA = 90◦ at a knee
flexion angle of ∼100◦ ; the 95% confidence intervals of
the means are shown for men (filled circles) and women
(open circles). (C) Tibiofemoral shear force (Fs; y-axis)
during isometric knee extension at various knee flexion
angles (x-axis) for men (filled circles) and women (open
symbols). During knee extension, the application of
posteriorly directed external forces of 100 N (squares and
circles) and 50 N (diamonds) against the anterior tibia at
0.4 m, 0.4 m and 0.2 m distal to the tibial plateau,
respectively. Positive values (Fs) indicate that the tibia
tends to slide anteriorly in relation to the femur (anterior
tibiofemoral shear). Source: Nisell 1985. Reproduced
with permission from Taylor & Francis.
VetBooks.ir
Tibial Tuberosity Advancement
Figure 28.2 Schematic representation of stifle joint
flexion with respect to PTA. In full extension, the PTA is
>90◦ and in full flexion the PTA is <90◦ . There is a point
such that the PTA is 90◦ , which is termed the ‘crossover’
point (see Figure 28.1C, Fs = 0.0). At this point, there is
neither cranial nor caudal tibiofemoral shear force
present. The premise of the tibial tuberosity advancement
(TTA), according to Tepic, is to alter the geometry of the
proximal tibia such that the PTA is maintained at ≤90◦
throughout the stifle joint range of motion during
weight-bearing; the TTA will change the PTA and move
the crossover point such that Fs = 0.0 N when PTA = 90◦
when the stifle joint is in full extension. Further stifle joint
flexion ensures that Fs is always ≤0.0 N and PTA ≤90◦ .
The PTA is thus maintained at ≤90◦ throughout the stifle
joint range of motion during weight-bearing. Compare
with Figure 28.5. Source: Boudrieau 2009. Reproduced
with permission from John Wiley & Sons, Inc.
Mesfar 2007). A decrease in retropatellar pressure after TTA also has been demonstrated
experimentally in the dog (Hoffmann et al.
2011). Theoretically, this diminished force can
protect the articular cartilage of both the
patella and the femur from subsequent damage.
Femorotibial contact pressure and location have
been evaluated in vitro using an experimental
model of a CrCL-deficient stifle joint, which
demonstrated an approximately 40% decrease
in contact area with an associated 100% increase
229
in peak pressure; furthermore, the positioning
of the peak pressure was found to shift caudally (Kim et al. 2009). TTA appeared to restore
the normal femorotibial contact and pressure
(Kim et al. 2009), which may spare the meniscus from risk of trauma after TTA (Figure 28.4).
This study also suggested that because TTA
did not change the geometry of the joint, and
the pressure distributions essentially remained
unchanged, there may be less development of
osteoarthritis over time. All of these findings
could support clinical studies that implied an
absence of problems with the patellar tendon
and the joint surfaces after TTA (Hoffmann et al.
2006; Lafaver et al. 2007; Stein & Schmoekel
2008; Kim et al. 2009).
These studies have recently been challenged
by more recent evaluations performed in vivo
on clinical cases, where persistent instability
was observed in dogs after TTA despite reportedly good postoperative function (Böttcher et al.
2013; Skinner et al. 2013). The reason for continued postoperative instability is debated, as
precise assessment of the amount of advancement after surgery is lacking. A number of
errors inherent in the techniques for preoperative planning and intraoperative technical
failures will contribute to the final position of
the tibial advancement and the resultant PTA.
These include such items as the differing proximal versus distal cage width and its final position within the osteotomy and patella-based
versus distal tibial tuberosity-based advancement. Furthermore, the appropriate PTA that
neutralizes tibiofemoral shear has not yet been
definitively documented in vivo.
As the resultant PTA is crucial to the determination of the amount of TTA, it has been suggested that the PTA is more accurately determined by the method of the common tangent (PTACT ) (Dennler et al. 2006; Schwandt
et al. 2006; Boudrieau 2009), as opposed to the
method using the TPA (PTATPA) (Boudrieau
2009; Hoffmann et al. 2011). The former method
has been proposed to be clinically more accurate as it takes into account the anatomic relationship between the femoral condyles and tibial plateau, as opposed to a static relationship
of the tibial plateau with the patellar tendon
(Boudrieau 2009) (Figure 28.5). Based on these
suppositions, PTACT has been recommended for
clinical use (2007 Veterinary Symposium – The
Surgical Treatment
VetBooks.ir
230
CTS-T
CTS-I
*
*
*
dI
*
CTS-O
CTS-CP
*
*
d
d
*
d
*
Figure 28.3 Lateral radiographic images of cranial tibial subluxation (CTS) in a loaded stifle joint within an
experimental limb press model. Left to right: before cranial cruciate ligament (CrCL) transection (CTS-I); after CrCL
transection (CTS-T); post-tibial tuberosity advancement after maximal tibial tuberosity advancement (CTS-O); and at
critical point tibial tuberosity advancement (CTS-CP). The critical point for the tibial tuberosity advancement distance in
this model was defined as the position one revolution before stifle joint instability occurred. The CTS was defined as ‘d’
in each figure: CTS-T/CTS-O/CTS-CP = d – dI , where dI (arrow) is the horizontal distance between the tibial marker (∗ )
and the vertical passing through the femoral marker (dotted line) in the intact CrCL (the intact CrCL was the reference
position), and d is the same horizontal distance (arrows) for each respective position (CTS-T, CTS-O, and CTS-CP). In this
specimen, CTS-T was positive, CTS-O was negative, and CTS-CP was slightly negative. Source: Apelt et al. 2007.
Reproduced with permission from John Wiley & Sons, Inc.
Normal
CrCL-Deficient
TTA-Treated
MPa
Figure 28.4 Axial view of bone models depicting three-dimensional poses of normal, cranial cruciate-deficient
(CrCL-Deficient), and tibial tuberosity advancement (TTA-Treated) stifles, with corresponding contact maps
representative of each testing condition. The tibia (light gray) is cranially displaced and internally rotated relative to the
femur (dark gray) after CrCL transection; the femorotibial poses of normal and TTA-treated stifles are similar. CrCL
transection resulted in a caudal shift, a reduced area and an increased pressure of femorotibial contact; TTA contact
patterns are similar to normal. Left = lateral; top = cranial. CrCL, cranial cruciate ligament; TTA, tibial tuberosity
advancement. Source: Kim et al. 2009. Reproduced with permission from John Wiley & Sons, Inc.
231
VetBooks.ir
Tibial Tuberosity Advancement
Post-op
Pre-op
(A)
(B)
(C)
Figure 28.5 Schematic representation of the tibiofemoral forces in the stifle joint, according to Tepic, before (A) and
after (B) tibial tuberosity advancement (TTA). The resultant compressive force (large white arrow) across the stifle joint is
parallel to the patellar tendon. Using the common tangent at the tibiofemoral contact point as the baseline (solid red
line), whereby the femur can move along this surface if the cranial cruciate ligament (CrCL) is deficient, the resultant
force can be broken down into its two orthogonal components (small blue arrows), one perpendicular and one parallel
to the tibial plateau. The latter represents the tibiofemoral shear force. If the angle of the tibial tuberosity is advanced
cranially until the patellar tendon angle (PTA) is reduced to 90◦ , the tibiofemoral shear force vector becomes zero, and
the joint compressive force and resultant force become one and the same. Note that the cranial tibiofemoral shear force
is smaller than that depicted with the PTA using the tibial plateau slope (TPS), which is indicated by the green dotted
line. Note that the common tangent and TPS are similar in stifle joint flexion (C). The insets clarify the force vectors
depicted on the schematic bone models. Compare with Figure 28.2. Source: Boudrieau 2009. Reproduced with
permission from John Wiley & Sons, Inc.
Surgical Summit; Pre-Symposium Laboratories:
TTA Laboratory; Chicago, IL, USA). Support
for this concept has been demonstrated experimentally, whereby less variability was observed
with PTACT versus PTATPA to achieve the target
PTA of 90◦ (Hoffmann et al. 2011). These findings have recently been questioned in a study
that found a poor agreement between PTACT
and PTATPA, moderate intra-observer reliability
and poor inter-observer reliability with PTACT ,
with good intra-observer reliability and moderate inter-observer reliability with PTATPA, thus
concluding that PTACT is not recommended
(Millet et al. 2013). Reconciling the differences
between the different studies is problematic
(Dennler 2006; Hoffmann et al. 2011; Millet
et al. 2013). An agreement between PTACT and
PTATPA is certainly not expected due to the complex joint anatomy that differs between dogs,
including differing stifle joint extension angles
and change of femoral position as the femoral
condyles roll backwards with stifle joint flexion (Boudrieau 2009). The latter factors are the
arguments supporting the rationale for using
the PTACT in the pre-planning, as described by
the originators of the surgical technique (Tepic
et al. 2002).
Implants and techniques
Currently there are two general techniques
to perform the TTA, described as the firstand second-generation methods. The firstgeneration method is the initial method as proposed by Tepic (Kyon; Boston, MA, USA), using
a titanium cage to maintain the advancement
and a corresponding titanium plate with forks
VetBooks.ir
232
Surgical Treatment
to make a stable construct. In this technique, a
patella-based positioning of the tibial tuberosity is performed, with a slight proximal shift of
the tibial crest segment with the advancement,
so as to not change the patella position. Finally,
a graft is applied within the osteotomy gap and
within the cage (Lafaver et al. 2007). The need
for a graft is controversial (Guerrero et al. 2011;
Boudrieau 2011).
The second-generation method is currently
evolving. Plates are no longer used; instead,
the construct is held in place by a cage only,
but with varying ‘accessories’ or ‘adjunct’ methods to ensure that the cage remains in place
(Brunel et al. 2013; Samoy et al. 2015; Torrington 2015). One of the major conceptual modifications is an incomplete distal osteotomy of the
tibial tuberosity, so as to help stabilize the fixation. This encompasses a distal-based tuberosity advancement. This type of advancement
was not recommended during development of
the first-generation method, where a patellabased advancement is used. With the secondgeneration TTA, the advancement causes some
distal displacement of the patella. The rationale
for the incomplete osteotomy of the distal end
of the tibial tuberosity is that it aids construct
stability and neutralization of the distractive
force of the quadriceps mechanism that were
previously neutralized with a plate. A result
of this modification is some distal patella displacement. The clinical ramifications, if any, of
this change in patella position have yet to be
investigated.
First-generation implants and techniques
The original implants were produced by the
technique inventors (Tepic, Kyon). These
titanium implants have been copied exactly,
although there is controversy as to the quality
of the copies. Other alternate implants that use
different fixation methods to achieve the same
general concept are also available. For example,
stainless steel plates with standard screws
instead of a fork for the tuberosity fixation
(XGEN forkless TTA plates; Securos Surgical,
Boise, ID, USA). Another approach is locking
screw fixation for the tuberosity segment, again
with a similar-appearing stainless steel plate
with a PEEK spacer (DePuy Synthes Vet, West
Chester, PA, USA). Many other similar copies
are available from a variety of manufacturers.
Second-generation implants
and techniques
Three basic concepts are currently marketed.
These include the modified Maquet procedure1
(MMP; Orthomed, West Yorkshire, UK), TTA
Rapid2 (Rita Leibinger, DE, USA) and TTA-23
(KYON Veterinary Surgical Products, Boston,
MA, USA). These techniques have resulted
in the development of alternative stand-alone
cage designs and techniques to orient the tibial osteotomy a fixed distance along the cranial tibial shaft that corresponds to the degree
of tuberosity advancement and cage width
desired. The specific technical feature of these
approaches, primarily pertain to the location
and length of the osteotomy, and the method
to spread of the incomplete osteotomy and
achieve the tuberosity advancement needed.
These details can be found on the manufacturer’s websites.1,2,3
TTA pre-planning and surgery
There are many considerations regarding the
pre-planning of TTA, particularly with regard
to the measurement methods using PTACT or
PTATPA. Additional alternative methods have
also been proposed. Some of the other techniques, such as the MMP procedure, have been
critically assessed; here, the target PTA of 90◦
is often not achieved as current planning methods may lead to underadvancement of the tibial
tuberosity (Kapler et al. 2015).
The planning methods for first- and secondgeneration techniques are similar and aim to
achieve a PTA of 90◦ . There are a number of
nuances with both the plan and its execution
to ensure that the TTA does achieve a postoperative PTA of 90◦ . Unfortunately, minimal data
1 MMP see pdf downloads at http://www.orthomed
.co.uk/
2 TTA Rapid, http://tta-rapid.com/
3 TTA-2, http://www.kyon.ch/current-products/tibialtuberosity-advancement-tta/tta-2-developmenttechnique
VetBooks.ir
Tibial Tuberosity Advancement
are available on postoperative evaluation of the
PTA in clinical cases; a single report has determined postoperative PTA in a series of cases
(Wolf et al. 2012). This oversight needs to be
corrected, so as to ensure that the technique is
performed appropriately. Such data will help
confirm clinically that TTA does result in stability of the stifle joint after surgery with neutralization of the tibiofemoral shear force in vivo.
Despite the many reports of successful surgical
outcomes, such evidence is not yet available.
The current recommendation, as presented
by the inventors of this technique (Tepic), is
to use the PTACT technique. This recommendation is based on knowledge of the variations
in the anatomy of the proximal tibial plateau
and the distal femur, and how anatomic factors affect advancement measurements when
using the common tangent between the tibial
and femoral surfaces at their contact point, or
PTACT (Boudrieau 2005; Boudrieau 2009). Less
variation has been reported with PTACT compared with PTATPA, further supporting this recommendation (Hoffmann et al. 2011).
The accuracy in planning the osteotomy and
determining amount of advancement has been
studied (Etchepareborde et al. 2011; Millet et al.
2013; Cadmus et al. 2014). Errors will occur
because of the varied anatomy encountered,
such as positioning (tibial drawer or stifle
joint extension angle), patella tendon insertion
point (high versus low), unrecognized effects
with regard to tibial tuberosity hinge point
(maintained at the distal attachment versus
allowed to move proximally), variation in the
pre-planning measurement method (Inauen
et al. 2009; Bush et al. 2011), and loss of advancement due to the saw kerf and cage position
(Botte 2013). For these reasons, virtual surgery
pre-planning is currently recommended. This
can be accomplished using digital software
(e.g., Orthoplan Elite; Sound, Carlsbad, CA,
USA) or a cut-and-paste manual method using
radiographic film. Virtual pre-planning (Figure 28.6) allows the cage advancement to be
measured at the appropriate point of cage
placement/position to achieve the desired
90◦ PTA postoperatively. Regardless of which
pre-planning method is used, accurate transfer
of the plan to the bone is required to achieve
the desired advancement. Factors related
to saw kerf, tuberosity displacement with
233
patella-based advancement, and cage positioning all need to be recognized.
TTA case selection
Several factors specific to the anatomic configuration of the limb should be considered before
selection of this surgical technique (Boudrieau
2009).
Low versus high patellar tendon
insertion point
The tibial tuberosity may be at greater risk for
fracture with TTA in cases with a low patellar tendon insertion point, as a smaller plate is
applied to the tibial crest and the usual position of the interspersed cage is above the most
proximal position of the plate, with little bone
present for support. Interestingly, this conformation may be better suited for a tibial plateau
leveling osteotomy as there is increased buttress support of the tibial tuberosity with greater
amounts of tibial plateau rotation. In dogs with
a high insertion point the TTA is preferable,
as a larger TTA plate can be applied to the
tibial crest, and the interspersed cage that is
placed within the gap remains buttressed with
adequate bone. Finally, the larger plate better
disperses all the forces to the tibial crest (Figure 28.7). Currently, there are no experimental
or clinical studies reported that support these
assumptions.
Excessive tibial plateau angle
Cases where there is excessive TPA are not conducive to TTA. The target PTA is 90◦ , but achieving this angle in such cases require substantially
greater advancement, sometimes beyond that
obtained with currently available implants (the
maximal cage width for the osteotomy gap is
15 mm). More importantly, there is a conformational deformity of the joint with excessive tibial
plateau angle that places the joint in a relative
angle of hyperextension, despite the limb itself
not being in the extended position (Figure 28.8).
The TTA does not address this malformation.
The maximal TPA to perform a TTA has yet to
Surgical Treatment
VetBooks.ir
234
(A)
(B)
(C)
(D)
(E)
(F)
Figure 28.6 (A) Preoperative lateral radiograph of the stifle joint in full but not forced extension. Different breeds of
dogs will have differing full extension joint angles. (B) The circles outline the femoral condyle and the tibial plateau,
respectively; a line (#1) is drawn between the centers of these two circles; a second line (#2) drawn perpendicular to #1
between the circles is the common tangent of the joint surfaces; finally, a third line (#3) parallel to line #1 is drawn that
passes through the cranial-most origin of the patella tendon at the distal pole. This is the planned tuberosity position in
order to obtain a patellar tendon angle of 90◦ . Note that the distance to move the most proximal point of the tibial
tuberosity to line #3 is NOT equivalent to the cage width (blue arrowheads, and also see panel D). A straight or distally
curved osteotomy can be planned for the tibial tuberosity (dotted lines). In this case, a curved line is selected to provide
more craniocaudal width due to the concave shape of the cranial border of the tibial crest (see panel C). (C) The outline
(red) of the tibial tuberosity is selected to match the planned osteotomy from panel B; note the length of the patellar
tendon (the orange line between the two orange arrowheads). (D) The tibial tuberosity is moved cranially so that the
proximal point of the tibial tuberosity intersects with the line #3, indicating the appropriate advancement distance. Note
that the position of the patella is unchanged (orange line between the two orange arrowheads). Therefore, the distal end
of the osteotomized tuberosity must move proximally (yellow arrows). The appropriate cage template is selected that
235
VetBooks.ir
Tibial Tuberosity Advancement
Figure 28.7 Lateral radiographs of the stifle joint, demonstrating the variation between the insertion points of the
patellar tendon into the tibial tuberosity. (A) Tibial tuberosity with a low insertion point. (B) Tibial tuberosity with a high
insertion point. A smaller plate must be applied when a shorter tibial tuberosity distance is available. The result is an
increase in the forces at each tine of the fork. Additionally, the overall plate length is shortened, potentially creating a
stress riser at the distal end of the osteotomy and the screws placed to secure the distal end of the plate. The tuberosity
shifts proximally with advancement in order to maintain patellar position. Furthermore, cage position (double-headed
arrow) provides greater buttress support of the tuberosity, and also buttresses the proximal attachment of the plate when a
high insertion point is present.
be determined. No data have been published
regarding the range of TPAs in dogs with TTA,
although it has been presented that successful
procedures have been performed in dogs with
a TPA of ∼30◦ . Anecdotally, it is proposed that
angles >30◦ are not well suited for a TTA (2007
Veterinary Symposium – The Surgical Summit;
Pre-Symposium Laboratories: TTA Laboratory;
Chicago, IL, USA).
Angular and torsional limb deformities
Angular and torsional limb deformities may
be treated with TTA. However, a separate
osteotomy is required for correction of any tibial varus, valgus, or torsion. The disadvantage of performing a separate osteotomy is
that the medial side of the bone already has
a plate positioned for the first-generation TTA
Figure 28.6 (Continued) spans the osteotomy gap 2–3 mm distal to the tibial plateau surface (white arrows). Note the
location of this cage and the corresponding location of the most proximal point of the tibial tuberosity. The width of the
cage is not equal to the distance observed in panel B; rather, it is wider as the upper edge of the cage and the
corresponding cage size is NOT placed at the level of the proximal point of the tibial tuberosity. (E) The appropriate plate
template is selected that spans the length of the tibial crest, and its orientation is noted so as to provide appropriate
positioning of both the fork and the distal screws of the plate. The large green arrowheads show the plate more caudally
positioned proximally as the most cranial border cannot be followed due to the concave cranial border of the tibial crest.
Note that the distal portion of the plate also overlies the tibial diaphysis, this occurs despite a slightly more caudal
orientation. (F) Postoperative radiograph that has copied the virtual plan and successfully resulted in appropriate
advancement to obtain a patellar tendon angle of 90◦ . The osteotomy and its position, and the cage and plate positions
have been successfully duplicated on the patient.
VetBooks.ir
236
Surgical Treatment
(A)
(B)
25°
43°
Figure 28.8 Lateral stifle joint radiographs demonstrating differences in the anatomic shape of the proximal tibia such
that the tibial plateau angle (TPA) is either considered excessive (A) at 43◦ , or within normal limits (B) at 25◦ . This
conformational deformity of the stifle joint angle in panel (A) places the joint in a relatively hyperextended position,
compared with panel (B). Advancing the tibial tuberosity does not correct this hyperextension as the TPA remains
unaltered. Source: Boudrieau 2009. Reproduced with permission from John Wiley & Sons, Inc.
in the proximal one-third of the medial tibial
surface, which will interfere with subsequent
additional medial plate fixation. Although a
standard plate could be applied over the thin
TTA plate, this is far from ideal and generally
not recommended. With the second-generation
TTA, using a wedge-only technique and no
plate, this issue is ameliorated. However, a second osteotomy in the transverse plane is still
required to address these deformities. Therefore, TTA is generally not recommended under
these circumstances.
Patellar luxation
Patellar luxation requiring tibial tuberosity
transposition combined with cruciate ligament
rupture may be very well suited to TTA, as any
desired transposition may be simultaneously
performed concurrently with the advancement.
In this instance, the TTA plate is slightly overbent to conform to the new laterally (or medially) transposed tibial crest. The alteration in
the surgical technique occurs with cage application. For example, in a medial patellar luxation, where the tibial crest is moved laterally,
either the caudal ‘ear’ of the cage is recessed
into the proximal tibia, or the cranial ‘ear’ of
the cage is elevated above the surface of the tibial tuberosity by interposing some washers, or
both (Figure 28.9). Ancillary fixation generally
is unnecessary. This technique has been briefly
described (2007 Veterinary Symposium – The
Surgical Summit; Pre-Symposium Laboratories:
TTA Laboratory; Chicago, IL, USA) (Boudrieau
2005), and reported in a series of cases (Yeadon
et al. 2011).
Patient size
TTA has been performed in dogs as small as
5 kg and as large as 92 kg (Hoffmann et al.
2006; Lafaver et al. 2007). Size limitation is
dependent on the availability of appropriately
sized implants (2- to 8-hole plates, and 3- to
15-mm cage widths, Kyon; Zürich, Switzerland). The implants are produced in a variety
of sizes such that they can be used in almost
any sized dog. In some instances, in very tall
dogs such as Great Danes, a limitation of the
TTA may be the large advancement distance
(>15 mm) that is required (Burns & Boudrieau
2008). The widest cage currently available to
support the osteotomy gap is 15 mm, which
became available in early 2009. Whereas the
cage can be moved further distally to increase
VetBooks.ir
Tibial Tuberosity Advancement
(A)
237
(B)
Figure 28.9 Craniomedial
view of the proximal tibia after
tibial tuberosity transposition
(TTA) performed routinely (A)
and after simultaneous lateral
transposition (B) with the
advancement for a medial
patellar luxation treatment. Note
that the caudal cage ‘ear’ has
been recessed slightly into the
caudal tibial bone fragment. This
is done by bending this ‘ear’ at
∼45◦ without removing a large
amount of bone. The plate also
is contoured such that it meets
the tuberosity more laterally.
Alternatively, or additionally, the
cranial cage ‘ear’ may be
elevated off of the tuberosity
bone by placing one to two
small metal washers under this
‘ear.’
the width of the gap, this must be done
judiciously because a large stress riser is created above the cage, which could result in fracture of the tibial tuberosity at that level (Burns &
Boudrieau 2008) (Figure 28.10). It is possible to
(A)
Figure 28.10 Mediolateral
radiographs of a 2.5-year-old,
neutered male Labrador
Retriever. (A) Immediately
postoperatively a 9-mm cage is
observed 1.2 cm distally within
the osteotomy gap along the
tibia with 2.3 cm of tibial
tuberosity proximal to the cage.
The granular material observed
within and below the cage is the
allograft of corticocancellous
chips. (B) At 8 weeks
postoperatively the tibial
tuberosity has fractured just
above the cage. Source: Burns &
Boudrieau 2008. Reproduced
with permission from Schattauer.
buttress the tibial tuberosity above the cage with
a block of cancellous bone allograft. However,
adding this graft adds a considerable additional
expense to the procedure (Burns & Boudrieau
2008).
(B)
VetBooks.ir
238
Surgical Treatment
Outcome and complications with
first-generation TTA
The first-generation cage with plate and fork
or screws has been in general use since 2006.
There are many anecdotal reports of good to
excellent results, and a number of early clinical results published (Hoffmann et al. 2006;
Lafaver et al. 2007; Stein & Schmoekel 2008; Voss
et al. 2008; Dymond et al. 2010; Kemper et al.
2011; Steinberg et al. 2011; Hirshenson et al. 2012;
Wolf et al. 2012; MacDonald et al. 2013; Skinner
et al. 2013; Kiefer et al. 2015). These reports comprise approximately 1600 cases, with an overall
complication rate of ∼19.0% to 59%. Major complications represent 2.3% to 26.1%, and minor
complications were 7.6% to 37%, with a reoperation rate of 9.8% (Hoffmann et al. 2006; Stein
& Schmoekel 2008; Voss et al. 2008; Dymond
et al. 2010; Kemper et al. 2011; Steinberg et al.
2011; Hirshenson et al. 2012; Wolf et al. 2012;
Kiefer et al. 2015). The most common complications were postliminary meniscal tears and tibial tuberosity fractures with or without implant
failure, infection, medial patella luxation and
tibial fracture. It has been proposed that many
of these complications are related to technical
failures, particularly insufficient advancement
and incorrect osteotomy placement (Botte 2013).
Radiographic healing was reported to
occur by 8–10 weeks postoperatively, and
with reported outcomes generally from 3 to
15 months postoperatively (Hoffmann et al.
2006; Lafaver et al. 2007; Stein & Schmoekel
2008). Good to excellent overall function and
clinical outcome in more than 90% of the dogs
was reported by the owners. The major differences between all of the reports included the
frequency of meniscal tears and the number of
technical failures reported.
Meniscus
Whether meniscal tears are the result of a
postliminary tear of an intact meniscus, or are
latent tears is unclear. Postliminary tears suggest that a meniscal release might be indicated,
whereas latent tears suggest that thorough joint
evaluation is necessary. Controversy remains
regarding the use of meniscal release. More
recently, persistent instability in the joint after
tibial tuberosity advancement has been suggested (Böttcher et al. 2013; Skinner et al. 2013),
but whether this is a consequence of the technique itself or incorrect execution of the TTA is
debated. Under-advancement because of inexperience with the technique and lack of awareness of potential pitfalls with preoperative planning may occur (Etchepareborde et al. 2011;
Bush et al. 2011; Botte 2013; Boudrieau 2013; Millet et al. 2013; Cadmus et al. 2014). The problem is reduced by virtual planning. Regardless of the reason, insufficient advancement can
result in persistent tibiofemoral shear instability and can be expected to result in postliminary meniscal tears. This may explain the purported value of meniscal release. Despite these
assertions, it appears that the clinical results
remain satisfactory in the majority of the cases
(Skinner et al. 2013). Given the limited information on TTA biomechanics, debate remains as
to whether or not to perform a medial meniscal release. It appears there are two opposing
opinions regarding the necessity of meniscal
release at this time with TTA. Further discussion of meniscal release is presented in Chapters
35 and 36. Continued postoperative instability
with confirmation of the amount of advancement and postoperative PTA needs to be documented to advance any understanding of TTA
clinical outcomes related to surgical planning
and technique.
Technical failures
The most common technical failures involve
an osteotomy that is too cranial with a small
tibial tuberosity bone fragment, or too low
adjacent to the level of distal plate screws,
which can create a stress-riser and a tibial
fracture. Tibial tuberosity fracture from inappropriate fork/screw placement into the tibial tuberosity bone fragment, most often due
to a small size crest fragment, patellar luxation from inappropriate realignment of the tibial tuberosity in the sagittal plane; distal patella
displacement because of a tuberosity-based
advancement, as opposed to a patella-based
advancement, are also common. Other miscellaneous complications include cage malposition (too high, too low, angled mediolaterally,
upside down), intra-articular screw placement,
VetBooks.ir
Tibial Tuberosity Advancement
(A)
239
(B)
Figure 28.11 Lateral radiographs of the stifle of 41.8-kg Golden Retriever after treatment with TTA-2. (A) Immediate
postoperative lateral radiograph. The saw guide was placed with four Kirschner wires to temporarily anchor it in position
to guide the osteotomy; three of the four holes are visible (small white arrows). An intraoperative bridge fracture at the
distal end of the tibial tuberosity occurred at the time of the tibial advancement. Note that it is no longer recommended
to use the adjacent K-wire hole as the location for a restraining suture. As a result of this fracture, three K-wires (0.062")
and an 18-gauge tension-band wire were placed proximally. The tension-band wire also passes through a hole used to
temporarily secure the saw guide. (B) The dog fractured the tibial diaphysis one day postoperatively when rising. This
shaft fracture originated at the site of the bridge fracture due to the stress-riser at this level. Recommendations for TTA-2
are evolving and have been recently updated. Currently, the saw cut is longer, with the length based on cage width/size,
and applied with a revised saw guide. The tuberosity should be advanced slowly, using gradual steps to prevent any
acute stress at the distal end of the tuberosity. The restraining suture at the distal end of the osteotomy is no longer used.
Similarly, a distal screw placed cranio-caudal below the cage is also no longer recommended. A proximal staple is
currently recommended (placed medially) to span the cage at its proximal extent to help neutralize torsional forces. All
of these measures are designed to avoid the bridge fracture at the distal end of the tibial tuberosity at the termination of
the osteotomy. (See also http://www.kyon.ch/current-products/tibial-tuberosity-advancement-tta/tta-2-developmenttechnique). Complications of the second-generation techniques are not unique to the TTA-2. All of the
second-generation techniques continue to evolve. Images provided courtesy of Dr Robert Botte.
transection or injury of the tendon of origin of
the long digital extensor, and delayed union or
non-union of the gap, often because no graft or
osteoconductive filler material was used.
Outcome and complications with
second-generation cage-only TTA
Second-generation TTA procedures eliminate
plate fixation. These methods propose a novel
cage and alternate osteotomy, but few results
have been published. All of the complications
noted previously with the first-generation techniques are a concern with second-generation
TTA. Some technical issues have been resolved
with use of a saw guide, but this approach
also introduces other potential problems. The
most obvious concern is the complication
of tibial fractures at the distal end of the
osteotomy (Figure 28.11) (Etchepareborde et al.
2011; Brunel et al. 2013; Barthélémy et al. 2014;
VetBooks.ir
240
Surgical Treatment
Etchepareborde et al. 2014; Bleakley 2015; Botte
2015; Hopmans 2015; Samoy et al. 2015; Torrington 2015).
All second-generation TTA methods have
varying techniques to decrease the stress-riser
at the distal end of the axially oriented incomplete frontal plane osteotomy, such as a tensionband wire, staple, relief drill-hole at the termination of the osteotomy, or increased osteotomy
length. No data are available indicating which
technique, if any, is superior for preventing subsequent problems. All of these techniques use
a distal tuberosity-based advancement which
will result in some distal patella displacement and an underestimation of the degree
of tibial advancement obtained. Whether distal patella displacement results in any clinical problems is unclear. However, inadequate
advancement may result in continued instability with tibiofemoral shearing and an increased
frequency of subsequent meniscal tears (Wolf
et al. 2012; Boudrieau 2013). An additional and
related complication is the possibility of tibial shaft fractures (Botte 2015; Hopmans 2015;
Torrington 2015). Some recommendations have
been proposed, along with newer saw guides,
to improve the osteotomy with regard to its
length, curvature, orientation in the frontal
plane, width of hinge area, and the need to modify or supplement the distal aspect of the cut
(Etchepareborde et al. 2011; Brunel et al. 2013;
Etchepareborde et al. 2014; Bleakley 2015; Botte
2015; Hopmans 2015; Samoy et al. 2015; Torrington 2015). Further studies are needed to
determine which of these strategies are most
effective. Clinical studies are also needed to
determine the frequency of complications with
second-generation TTA.
Conclusions
Currently there is no peer-reviewed evidence
of any substantial superiority for any one of
the surgical techniques for stifle stabilization
in dogs with cruciate ligament rupture over
the long term, and the specific technique chosen primarily depends on individual surgeon
preference (Leighton 1999). Anecdotal evidence
suggests that there may be a quicker recovery and return to full mobility in a shorter
period of time with TTA, similar to TPLO. The
rapid return to function is one of the primary
reasons that this technique is frequently performed. In addition, there is anecdotal evidence
from owners that dogs treated with TTA and
TPLO do better, interpreted as returning to
work such as hunting or field trials, than dogs
with either extra-articular lateral suture stabilization or intra-articular stabilization using an
over-the-top or similar method. Long-term clinical outcomes after TTA relative to other surgical techniques need to be documented.
References
Apelt D, Kowaleski M, Boudrieau RJ. Effect of tibial tuberosity advancement on cranial tibial subluxation in canine cranial cruciate-deficient stifle
joints: an in vitro experimental study. Vet Surg
2007;36:170–177.
Barthélémy N, Ramirez JM, Noel S, et al. Modified Maquet technique for treatment of canine cranial cruciate ligament injury: Early results, complications and risk factors in 109 dogs. Vet Surg
2014;43:E129.
Bleakley S. TTA-2: Research Projects, 2015 Kyon Symposium.
Böttcher P, Ray J, Fisher M. In vivo stifle kinematics:
The truth about TPLO and TTA. Proceedings of the
2013 ACVS Veterinary Symposium. San Antonio,
TX, October 24–26, 2013, pp. 415–417.
Botte R. Kyon TTA Masterclass. 2013 ACVS Veterinary
Symposium. San Antonio, TX, October 23, 2013.
Botte R. TTA-2 planning: Tips and tricks. 2015 Kyon
Symposium.
Boudrieau RJ. Tibial tuberosity advancement (TTA):
Clinical results. Proceedings of the ACVS Veterinary Symposium, 2005, pp. 443–445.
Boudrieau RJ. Tibial plateau leveling osteotomy or
tibial tuberosity advancement? Vet Surg 2009;38:1–
22.
Boudrieau RJ. Letter to the Editor; Comparison of
healing of the osteotomy gap after tibial tuberosity advancement with and without use of an autogenous cancellous bone graft [Vet Surg 2011;40:27–
33]. Vet Surg 2011;40:641–643.
Boudrieau RJ. Why I cut the meniscus. Kyon TTA
Masterclass. 2013 ACVS Veterinary Symposium. San
Antonio, TX, October 23, 2013.
Brown NP, Bertocci GE, Marcellin-Little DJ. Canine
stifle biomechanics associated with Tibial Tuberosity Advancement predicted using a computer
model. Vet Surg 2015;44:866–873.
Brunel L, Etchepareborde S, Barthélémy N, et al.
Mechanical testing of a new osteotomy design for
tibial tuberosity advancement using the modified
Maquet technique. Vet Comp Orthop Traumatol
2013;26:47–53.
VetBooks.ir
Tibial Tuberosity Advancement
Burns CG, Boudrieau RJ. Modified tibial tuberosity advancement procedure with tibial tuberosity
advancement in excess of 12 mm in four large breed
dogs with cranial cruciate ligament-deficient joints.
Vet Comp Orthop Traumatol 2008;21:250–255.
Bush MAZ, Bowlt K, Gines JA, et al. Effect of use of
different landmark methods on determining stifle
angle and on calculated tibial tuberosity advancement. Vet Comp Orthop Traumatol 2011;24:205–
210.
Cadmus J, Palmer RH, Duncan C. The effect of preoperative planning method on recommended tibial tuberosity advancement cage size. Vet Surg
2014;43:995–1000.
Dennler R, Kipfer NM, Tepic S, et al. Inclination of the
patellar ligament in relation to flexion angle in stifle
joints of dogs without degenerative joint disease.
Am J Vet Res 2006;67:1849–1854.
Dymond NL, Goldsmid SE, Simpson DJ. Tibial
tuberosity advancement in 92 canine stifles: Initial results, clinical outcome and owner evaluation.
Aust Vet J 2010;88:381–385.
Etchepareborde S, Mills J, Busoni V, et al. Theoretical
discrepancy between cage size and efficient tibial
tuberosity advancement in dogs treated for cranial
cruciate ligament rupture. Vet Comp Orthop Traumatol 2011;24:27–31.
Etchepareborde S, Barthélémy N, Brunel L, et al.
Biomechanical testing of a β-tricalcium phosphate
wedge for advancement of the tibial tuberosity. Vet
Comp Orthop Traumatol 2014;27:14–19.
Giffin JR, Vogrin TM, Zantop T, et al. Effects of increasing tibial slope on the biomechanics of the knee.
Am J Sports Med 2004;32:376–382.
Guerrero TG, Makara MA, Katiofsky K, et al. Comparison of healing of the osteotomy gap after tibial tuberosity advancement with and without use
of an autogenous cancellous bone graft. Vet Surg
2011;40:27–33.
Hirshenson MS, Krotscheck U, Thompson MS, et al.
Evaluation of complications and short-term outcome after unilateral or single-session bilateral
tibial tuberosity advancement for cranial cruciate rupture in dogs. Vet Comp Orthop Traumatol
2012;25:402–409.
Hoffmann DE, Miller JM, Ober CP, et al. Tibial
tuberosity advancement in 65 canine stifles. Vet
Comp Orthop Traumatol 2006;19:219–227.
Hoffmann DE, Kowaleski MP, Johnson KA, et al.
Ex vivo biomechanical evaluation of the canine
CrCL deficient stifle with varying angles of stifle
joint flexion and axial loads after TTA. Vet Surg
2011;40:311–320.
Hopmans J. TTA-2 clinical experience. Kyon Symposium 2015.
Inauen R, Koch D, Bass M, et al. Tibial tuberosity conformation as a risk factor for cranial cruciate ligament rupture in the dog. Vet Comp Orthop Traumatol 2009;22:16–20.
241
Kapler MW, Marcellin-Little DJ, Roe SC. Planned
wedge size compared to achieved advancement in
dogs undergoing the modified Maquet procedure.
Vet Comp Orthop Traumatol 2015;28:379–384.
Kemper M, Koch D, Bass M, et al. Revisionsoperationsrate nach 214 Tibial Tuberosity Advancements als Thbusherapie des vorderen Kreuuzbandrisses beim Hund [Major complication rate after
214 tibial tuberosity advancements as a therapy for
cranial cruciate ligament rupture]. Schweiz Arch
Teirheilkd 2011;153:131–133.
Kiefer JE, Langenbach A, Boim J, et al. Singlestage bilateral tibial tuberosity advancement for
treatment of bilateral canine cranial cruciate ligament deficiency. Vet Comp Orthop Traumatol
2015;28:215–219.
Kim SE, Pozzi A, Banks SA, et al. Effect of tibial tuberosity advancement on femorotibial contact mechanics and stifle kinematics. Vet Surg
2009;38:33–39.
Kipfer NM, Damur DM, Guerrero T, et al. Effect of tibial tuberosity advancement on femorotibial shear
in cranial cruciate-deficient stifles: an in vitro study.
Vet Comp Orthop Traumatol 2008;21:385–390.
Lafaver S, Miller NA, Stubbs WP, et al. Tibial tuberosity advancement for stabilization of the canine cranial cruciate ligament-deficient stifle joint: surgical technique, early results and complication in 101
dogs. Vet Surg 2007;36:573–586.
Leighton RL. Letter to the Editor, Preferred method
of repair of cranial cruciate ligament rupture in
dogs: A survey of ACVS diplomates specializing in
canine orthopedics. Vet Surg 1999;28:194.
Li G, Rudy TW, Allen C, et al. Effect of combined
axial compressive and anterior tibial loads on in situ
forces in the anterior cruciate ligament: a porcine
model. J Orthop Res 1998;16:122–127.
Maquet P. Tibial tuberosity advancement. Clin
Orthop Rel Res 1976;115:225–230.
MacDonald TL, Allen DA, Monteith GJ. Clinical
assessment following tibial tuberosity advancement in 28 stifles at 6 months and 1 year after
surgery. Can Vet J 2013;54:249–254.
Miller JM, Shires PK, Lanz OI, et al. Effect of 9
mm tibial tuberosity advancement on cranial tibial
translation in the canine cranial cruciate ligamentdeficient stifle. Vet Surg 2007;36:335–340.
Millet M, Bismuth C, Labrunie A, et al. Measurement of the patellar tendon-tibial plateau angle and
tuberosity advancement in dogs with cranial cruciate ligament rupture: Reliability of the common
tangent and tibial plateau methods of measurement. Vet Comp Orthop Traumatol 2013;26:469–
478.
Montavon PM, Damur DM, Tepic S. Advancement
of the tibial tuberosity for the treatment of cranial
cruciate deficient canine stifle. 1st World Orthopedic Veterinary Congress, Munich, Germany, 2002,
p. 152.
VetBooks.ir
242
Surgical Treatment
Nakamura N, Ellis M, Seedhom BB. Advancement of
the tibial tuberosity: a biomechanical study. J Bone
Joint Surg 1985;67B:255–260.
Nisell R. Mechanics of the knee. A study of joint and
muscle load with clinical applications. Acta Orthop
Scand Suppl 1985;56:3–42.
Nisell R, Németh G, Ohlsén H. Joint forces in the
extension of the knee: Analysis of a mechanical
model. Acta Orthop Scand 1986;57:41–46.
Nisell R, Ericson MO, Nemeth G, et al. Tibiofemoral
joint forces during isokinetic knee extension. Am J
Sports Med 1989;17:49–54.
Samoy Y, Verhoeven G, Bosmans T, et al. TTA Rapid:
Description of the technique and short term clinical trial results of the first 50 Cases. Vet Surg
2015;44:474.
Schwandt CS, Bohorquez-Vanelli A, Tepic S, et al.
Angle between the patellar ligament and the tibial
plateau in dogs with partial rupture of the cranial
cruciate ligament. Am J Vet Res 2006;67:1855–1860.
Shirazi-Adl A, Mesfar W. Effect of tibial tubercle elevation on biomechanics of the entire knee joint
under muscle loads. Clin Biomech 2007;22:344–351.
Skinner OT, Kim SE, Pozzi A. In vivo femorotibial subluxation during weight-bearing and clinical outcome following tibial tuberosity advancement for
cranial cruciate ligament insufficiency in dogs. Vet
J 2013;196:86–91.
Stein S, Schmoekel H. Short-term and eight to 12
months results of a tibial tuberosity advancement
as treatment of canine cranial cruciate ligament
damage. J Small Anim Pract 2008;49:398–404.
Steinberg EJ, Prata RG, Palazzini K, et al. Tibial
tuberosity advancement for treatment of CrCL
injury: Complications and owner satisfaction. J Am
Anim Hosp Assoc 2011;47:250–257.
Tepic S, Damur D, Montavon PM. Biomechanics of
the stifle joint. 1st World Orthopedic Veterinary
Congress, Munich, Germany, 2002, pp. 189–190.
Torrington A. TTA-2 clinical trial study data. Kyon
Symposium 2015.
Voss K, Damur DM, Guerrero T, et al. Force plate
gait analysis to assess limb function after tibial
tuberosity advancement in dogs with cranial cruciate ligament disease. Vet Comp Orthop Traumatol
2008;21:243–249.
Wolf RE, Scavelli TD, Hoelzler MG, et al. Surgical and
postoperative complications associated with tibial
tuberosity advancement for cranial cruciate ligament rupture in dogs: 458 cases (2007–2009). J Am
Vet Med Assoc 2012;240:1481–1487.
Yeadon R, Fitzpatrick N, Kowaleski M. Tibial tuberosity transposition-advancement for treatment of
medial patellar luxation and concomitant cranial
cruciate ligament disease in the dog. Vet Comp
Orthop Traumatol 2011;24:18–26.
VetBooks.ir
29
Closing Cranial Wedge
Ostectomy and Triple
Tibial Osteotomy
Simon C. Roe
Closing cranial wedge
ostectomy (CCWO)
there are associated varus, valgus, or rotational
deformities.
Introduction
Technique research
Closing cranial wedge ostectomy (CCWO) was
the first osteotomy procedure proposed to alter
the forces that act around the stifle and on the
cranial cruciate ligament (CrCL) (Slocum &
Devine 1984). Previously, the technique had
been reported for the management of five dogs
with proximal tibial deformity and cruciate ligament rupture, the idea being that normalization of the tibial anatomy would improve stifle
function (Read & Robins 1982). This approach
was later superseded by tibial plateau leveling
osteotomy (TPLO), with the potential advantages that the length of the tibia was not altered
and the osteotomy did not cross the whole shaft
of the bone. However, CCWO continues to be
used by some surgeons, particularly in situations where TPLO may have an increased risk
of complications. This applies primarily to dogs
that have an excessively steep tibial plateau
angle (TPA), though it may also be considered if
It had been assumed that the target TPA for
CCWO was similar to that proposed for TPLO
(6◦ ), and therefore that the removal of a wedge
that was 6◦ less than the measured tibial slope
would result in the appropriate TPA. However, because the TPA is calculated from the
functional tibial axis (from intercondylar eminences to center of the talus) and that, after
CCWO, the intercondylar notches move cranial relative to their original position, thereby
also shifting the functional axis cranially, a full
correction would not be achieved using this
technique (Bailey et al. 2007; Apelt et al. 2010).
To minimize this cranial shift (and thus the size
of the wedge that needs to be removed), the
osteotomy should be located as proximally as
possible (while allowing sufficient length for
engaging three screws), and the cranial cortices
should be aligned, rather than simply hinging
the wedge on its apex (which would align the
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
243
VetBooks.ir
244
Surgical Treatment
caudal cortices). If this is done, the functional
axis shift will be around 5◦ for a 25◦ wedge, and
7–8◦ for a 35–40◦ wedge.
Technique: planning
The principles of CCWO for either managing
proximal tibial deformity or reducing the TPA
are similar to those used when correcting deformities in other bones, though there are certain considerations that are specific to this location. In early descriptions of the procedure,
the osteotomy was located more distal because
only straight plates were available for stabilization, and sufficient space was needed to ensure
purchase for three bicortical screws. With the
development of purpose-designed plates (TWO
plates; Veterinary Instrumentation, Sheffield,
UK, and TPLO plates from various manufacturers), the level of the osteotomy is now positioned more proximal, and the amount of functional axis shift is smaller. The size of the wedge
to be removed is planned on the ‘90–90’ lateral
view of the tibia, named after the fact that the
stifle and tarsus are position at 90◦ of flexion,
with the beam centered over the stifle. The TPA
is measured. The optimal postoperative TPA
is considered to be 6◦ . The appropriate wedge
size will depend on the magnitude of the TPA,
the level of the osteotomy, and whether the
cranial cortices of the tibial will be aligned. If
the osteotomy is proximal and the cranial cortices are aligned, wedge sizes are usually 2–3◦
less than the TPA for TPAs of 25–32◦ . For a
TPA greater than 35◦ , the wedge size should be
the same as the TPA. The limb and the radiographs should be assessed to determine if there
is significant varus/valgus or tibial torsion that
should be addressed. Varus and valgus can be
corrected by adjusting the plane of one of the
osteotomies relative to the other. Torsion can
be corrected by rotation of the fragments at
the level of the osteotomy. The stabilizing plate
must be contoured appropriately to maintain
the intended rotation correction.
When planning corrections of large TPAs, it
may be helpful to print an image of the lateral
tibial radiograph, draw the planned wedge in
the anticipated location, cut out the wedge, and
reposition the ‘fragments’ to simulate reduction. The TPA can be measured on this paper
model, and the effect of the cranial shift on the
functional axis appreciated. If the final TPA is
not appropriate, the size of the wedge can be
adjusted accordingly and the exercise repeated.
This same process can be performed digitally
using some of the planning software packages
that allow the ‘cutting’ and repositioning of
image fragments (Figure 29.1).
A recent modification described by Frederick & Cross (2017) results in less length loss for
the same wedge size. The position of the proximal cut is planned similarly to that described
above. The level of the distal cut is adjusted
proximally such that the proximal and distal
osteotomies will be of equal length (Figure 29.2).
The cranial edges are aligned in the same way as
usual.
Technique: intraoperative
The medial aspect of the proximal tibia is
exposed and the muscles elevated caudally and
laterally at the proposed level of the osteotomy.
The joint level is identified and the planned
stabilizing implant positioned on the proximal fragment to assist in identifying the most
proximal level of the ostectomy. The proximal osteotomy line is scored, ensuring that it
is approximately parallel to the tibial plateau
and that it is 3–5 mm distal to the insertion of
the patella tendon. Using a goniometer, wedge
set, or custom wedge guide (sterilized radiographic film), the second osteotomy line is
scored, with the apex at the caudal cortex. The
two cuts are made ensuring that they are coplanar. The wedge is removed and the fragments
reduced, with the cranial cortices aligned. If
a large wedge was removed, the intact fibula
may prevent complete reduction. It should be
cut or fractured at the level of the osteotomy.
A Kirschner wire placed from cranial to caudal across the osteotomy may help to maintain reduction while the plate is contoured and
applied.
Patient selection
CCWO can be used to level the plateau of any
tibia. It has been superseded by TPLO based
VetBooks.ir
Closing Cranial Wedge Ostectomy and Triple Tibial Osteotomy
(A)
245
(B)
Figure 29.1 Closing cranial wedge ostectomy planning. (A) Lateral radiograph of the tibia of a dog with cranial cruciate
ligament rupture and a steep tibial slope. Lines depicting the functional axis of the tibia and the tibial plateau have been
positioned. The angle between these lines indicates a tibial plateau slope of 41◦ . The planned wedge (42◦ ) is outlined on
the proximal metaphysis of the tibia. (B) The radiographic image has been ‘cut’ and the proximal portion rotated to
simulate the surgical correction. Note the cranial shift of the redrawn functional axis (compared to the original axis
position, indicated by the light gray line). The resulting tibial plateau slope is 5◦ .
on concerns that it may lead to some shortening of the tibia and that, because it is a complete osteotomy of the tibial shaft, it is potentially more susceptible to failure of fixation than
a TPLO. It is, therefore, often reserved for situations where a TPLO may carry more risk. These
might include a steep TPA or small patient
size.
VetBooks.ir
246
Surgical Treatment
(A)
(B)
(C)
(D)
(E)
(F)
Figure 29.2 Illustration of modified cranial closing wedge ostectomy procedure steps. (A) The proximal osteotomy is
scored exiting the cranial cortex ∼3 mm distal to the patella tendon insertion point. (B) The distal osteotomy is scored
intersecting the proximal score at ∼2/3 the cranial-caudal point of the distal score. The intersection of these scores was
the planned osteotomy angle. (C) The distal osteotomy is completed. (D) The proximal osteotomy is completed exiting
through the distal osteotomy. (E) The osteotomy is reduced by rotating the segments. (F) Reduced osteotomy with
alignment of cranial cortices.
Implant selection
There are many factors that influence implant
selection, and considering all of these and their
interactions is important to reduce the potential
for complications. It is important to realize that
there are very strong forces acting to open the
osteotomy, and the chosen plate must be able
to counter these forces. The primary factor is
the level of the osteotomy; a low osteotomy will
result in a larger proximal fragment and, therefore, more screw purchase. To reduce the shift
of the functional axis, the osteotomy is moved
as proximal as is feasible. T-style plates, where
three or more screws are concentrated in an
expanded portion of plate, are helpful for this
purpose. However, plates designed specifically
for TPLO have the screws clustered close to
each other because of the small size of the fragment they must engage. In many of these plates
VetBooks.ir
Closing Cranial Wedge Ostectomy and Triple Tibial Osteotomy
the screws also converge slightly on the lateral aspect. These features reduce the ability of
this plate to counter the forces working to open
the osteotomy, and catastrophic failure of screw
purchase can occur. For this reason, a T-style
or cloverleaf plate with a wider screw distribution may provide greater stability. If a plate
designed for TPLO is used, it is essential to
add adjunct fixation. Options for adjunct fixation include a cranial tension band wire, small
plate or, with an angled osteotomy, a bone screw
lagged across the osteotomy (Figure 29.3).
(A)
247
Complications
The primary major complication specific to
CCWO is failure of fixation of the proximal
fragment. This risk is reduced if an appropriately sized plate is selected and adjunct fixation
is well placed.
Outcome
Outcome has been reported for a number of
small case series, usually with some defining
(B)
Figure 29.3 Lateral (A) and cranio-caudal (B) postoperative radiographs after a 41◦ closing cranial wedge ostectomy
(CCWO). The cranial cortices were aligned and the osteotomy stabilized with a 3.5 cloverhead plate with three locking
screws in the proximal fragment applied medially (Veterinary Orthopaedic Implants, St Augustine, FL, USA). A 2.7-mm
‘L’ plate (DePuy SynthesVet, Paoli, PA, USA) has been applied cranially as a ‘tension band’ to counter the quadriceps
force that tends to open the osteotomy.
VetBooks.ir
248
Surgical Treatment
feature such as steep slope (Read & Robins
1982) or small-sized patients (Macias et al. 2002).
Outcome after CCWO is similar to that after
TPLO (Corr & Brown 2007; Oxley et al. 2013). In
the Corr & Brown study the complication rates
were not different, but implant failure requiring
revision was seen more frequently with CCWO
treatment, although only a single TPLO plate
with standard screws was used for stabilization. Complication rates, including late meniscal tears and wound and joint infections, were
similar between procedures in the study conducted by Oxley et al. (TPLO 7.2%; CCWO
9.5%). The CCWO technique involved planning a wedge that was more proximally positioned, had equal length osteotomy surfaces,
and was caudally hinged. The wedge size was
adjusted for the anticipated cranial axis shift,
with a larger adjustment made for larger correction angles. A pre-contoured TPLO plate with
all proximal screws locked and a supporting
cranial wire was used for all CCWO cases, and
no implant failures were identified. A review of
300 CCWO surgeries found an overall complication rate of 31.7% (Kuan et al. 2009). Four dogs
(1.3%) required additional surgery to address
implant failure and osteotomy instability. The
type of plate and screws was not described, but
a cranially placed wire was used.
Conclusions
CCWO is an effective approach for leveling
the tibial plateau. Planning of the wedge size
must take into account the shift in the functional axis that occurs as the ostectomy is closed.
This shift can be minimized by locating the
osteotomy more proximally and by aligning the
cranial fragment edges. Adequate fixation must
be used to counter the strong forces that act on
the osteotomy. A cranial ‘tension band’ of some
form is recommended to minimize the risk of
failure of fixation.
Triple tibial osteotomy
Introduction
Triple tibial osteotomy (TTO) was first
described by Bruce et al. in 2007. While the
goal is similar to that of the TTA, namely to
create a 90◦ angle between the tibial plateau
slope and the patella tendon at a stifle angle
of 135◦ , this is achieved by a combination of a
closing wedge ostectomy (leveling of the tibial
plateau) and advancement of the tibial tuberosity which is pushed by the cranio-proximal
corner of the rotating proximal fragment. In the
initial report a geometric analysis suggested
that if the wedge were two-thirds of the correction angle, the other one-third would be
achieved by the tuberosity advancement. A retrospective analysis of the amount of correction
achieved indicated that this was insufficient,
and the formula was later revised to: Wedge
angle = Correction angle × 0.6 + 7 (TTO Technique Guide, Veterinary Instrumentation, Inc.,
Sheffield, UK). This adjustment is likely due
to the shift in the functional tibial axis, and
the fact that the tuberosity advances cranially
only and not proximally, necessitating a larger
correction.
Technique: planning
Planning is performed on a lateral radiograph
of the stifle at an angle of 135◦ . The length of
the patella tendon is determined and the tibial plateau–patella tendon (TP-PT) angle measured. The correction angle is the TP–PT angle
minus 90◦ , and the wedge angle is calculated
using the formula given above.
The wedge angle may need to be adjusted in
dogs with unusual tibial tuberosity morphology (Renwick et al. 2009). If the patella tendon insertion is very low, the correction may
be overestimated, and if it is very high it may
be underestimated. Also, if the tibia is cranially
subluxated, or the stifle is more flexed than recommended when the radiograph is taken, the
measured correction angle will be less. It is recommended that radiographs be critically evaluated for position, the TPA be measured, and
the tuberosity morphology considered before
deciding on a final wedge angle.
Technique: intraoperative
Specialized instrumentation is available that
simplifies a number of the steps in this
procedure (Veterinary Instrumentation, Inc.,
Sheffield, UK). First, the medial aspect of the
VetBooks.ir
Closing Cranial Wedge Ostectomy and Triple Tibial Osteotomy
CA
D
WA
B
Figure 29.4 Triple tibial osteotomy planning. The angle
between lines depicting the tibial plateau (TP) and the
patella tendon (PT) with the stifle at an approximately
135◦ angle is formed. The correction angle (CA) is
calculated as the TP-PT angle minus 90◦ . The length of
the PT is measured. The hole at the distal end of the tibial
tuberosity cut (B) is located by measuring the PT length
distal from the PT insertion. The first cut, depicted by the
black line extending proximad from the hole at B,
separates the tibial tuberosity from the tibial shaft. The
length of the cut is measured and a hole (D) is drilled
level with the mid-point, approximately 3 mm in from the
caudal edge of the tibia. The wedge angle (WA) is
calculated from the CA: WA = CA × 0.6 + 7. The wedge
is cut, and the ostectomy reduced and stabilized with a
plate.
tibia is exposed. Then, using the length of the
patella tendon measured during planning, a
point is marked distal to the insertion of the
patella tendon (Figure 29.4, point B). A 2-mm
hole is drilled from medial to lateral and a linear
saw guide inserted and aligned parallel to the
cranial edge of the tuberosity. The bone is cut,
the saw guide removed, and the cut completed.
249
The tuberosity fragment is held off the caudal
fragment by a spacer tool, called a wedgie. The
mid-point of the osteotomy is marked and a
2-mm hole is drilled at that level from medial
to lateral 2–3 mm in from the caudal edge of
the tibia (Figure 29.4, point D). The pin of the
combined osteometer and saw guide is placed
in the hole and the guide is positioned so that
the removed wedge is centered on the apex. It
is held in position with a purpose-made, selfretaining forceps (a clasper) or 1.6 mm K-wire
through a hole in the distal arm of the osteometer. The cuts are made in the medial cortex,
the guide is removed, and the cuts are completed through the lateral cortex. The popliteal
artery is retracted as the lateral cortex is cut.
The bone wedge is removed and used later as
a bone graft. The wedgie tool is moved distal
to the ostectomy to hold the tibial crest fragment in a cranial position so that the proximal
tibial fragment can be fully reduced. A large
pointed reduction forceps is placed on the proximal aspect of the proximal fragment and on
the base of the tibial tuberosity and is squeezed
until the ostectomy is reduced. A bone plate is
contoured to the medial aspect of the tibia and
secured with bone screws. The bone wedge is
cut into 2 mm-sized fragments and packed into
the defect between the tuberosity fragment and
the shaft.
Patient selection
TTO is more likely to develop complications if
used to manage excessive slope. With a bone
wedge larger than 20◦ , it is likely that one
or both bone bridges will fracture. In dogs
with unusual tibial tuberosity morphology, the
appropriate wedge size is harder to determine
and another technique may be more suitable.
While TTO can be performed in small dogs,
the osteotomies need to be very precise in dogs
weighing <10 kg.
Implant selection
Because the osteotomy is slightly lower than
where the TPLO osteotomy is usually located,
the pre-contoured locking TPLO plate will not
be suitable in all cases. Some tibias are relatively
flat, and removing the pre-contour may result
in screws being directed towards the osteotomy.
VetBooks.ir
250
Surgical Treatment
(A)
(B)
Figure 29.5 Lateral (A) and cranio-caudal (B) radiographs of a completed triple tibial osteotomy (TTO). A small amount
of the flare of the pre-contoured locking TPLO plate was removed. The plate is secured with two standard screws and
one locking screw above and below the ostectomy. Note that the tibial plateau angle has been reduced and the tibial
tuberosity advanced. A very small crack is evident extending distal from the hole at the distal end of the tibial tuberosity
osteotomy. A tension band was not considered necessary. The bone bridge caudal to the wedge is also cracked, but this
did not impact the reduction of the ostectomy. The removed bone wedge has been cut into 2-mm pieces and packed into
the defect behind the tibial tuberosity fragment.
In these cases, a cloverleaf-shaped TTO plate of
appropriate size or different TPLO plate (e.g.,
the SOPTM TPLO plate; Orthomed NA, Vero
Beach, FL, USA) can be contoured and applied
to stabilize the osteotomy (Figure 29.5).
Complications
During surgery it is possible that the bone
bridges may crack or fracture. If the base of the
tibial tuberosity fragment cracks, a tension band
wire is placed. If it fractures completely, a Kwire is used to maintain reduction and a tension
band wire (or, in large dogs, two tension band
wires) is placed. If there is concurrent medial
patella luxation (MPL), the tuberosity fragment
can easily be lateralized. The base will usually
fracture with this re-positioning, and the placement of one or two K-wires and a tension band
is indicated (Figure 29.6).
The caudal bone bridge also may crack during reduction. This may cause the proximal
fragment to be more difficult to reduce, but
the situation is usually easily managed and the
plate can be applied.
If the patient is too active, it is possible that
the tibial tuberosity fragment may fracture. If
251
VetBooks.ir
Closing Cranial Wedge Ostectomy and Triple Tibial Osteotomy
(A)
(B)
Figure 29.6 Treatment of combined cruciate ligament rupture and medial patella luxation. Immediate postoperative
radiographs of the proximal tibia after a triple tibial osteotomy (TTO) combined with lateral translation of the tibial
tuberosity fragment to re-align the quadriceps mechanism and position the patella in line with the trochlear groove. The
wedge ostectomy is stabilized with a pre-contoured TPLO plate. The tibial tuberosity position was maintained with two
K-wires and two tension band wires were placed to counter the pull of the quadriceps mechanism.
this is minimally displaced, and the patient is
not lame, conservative management is usually
successful. However, if it is unstable or the
patient is lame, then surgical stabilization with
a K-wire and tension band wire is indicated.
In a review of 121 TTO procedures, fracture
of the distal attachment of the tibial tuberosity fragment was observed in nine tibias, three
of which were managed surgically (Moles et al.
2009).
Other complications reported are similar to
those evident in other osteotomy procedures
(surgical site infection, late meniscal tears)
(Bruce et al. 2007; Moles et al. 2009; Renwick et al.
2009).
Outcome
When the tuberosity fragment is stable, healing
is usually adequate at 6–8 weeks after surgery.
Union between the cranio-proximal corner of
the plateau fragment and the tuberosity fragment likely protects the osteotomy.
Subjective assessments of outcome by owners indicated a good return to normal function
in the majority of cases (Bruce et al. 2007; Moles
et al. 2009; Renwick et al. 2009). No studies using
objective measures have been performed. Given
that the endpoint of the surgery is based on
similar principles to the TTA, similar outcomes
would be expected.
VetBooks.ir
252
Surgical Treatment
Conclusions
TTO represents another approach to modifying
the forces around the stifle in order to achieve
functional stability following cruciate ligament
rupture. About two-thirds of the adjustment
is achieved by leveling of the tibial plateau,
and one-third by advancing the tibial tuberosity. Because of this combined approach, the
overall morphology of the tibia is altered less
than with a CCWO. Also, because the tibial
tuberosity is separated from the plateau fragment, there is much less force acting on the
osteotomy, and complications of fixation are
therefore much reduced. The specialized instrumentation facilitates accurate wedge cutting.
For surgeons unfamiliar with TPLO and who
are unable to purchase a radial cut saw, the TTO
procedure is a viable alternative.
References
Apelt D, Pozzi A, Marcellin-Little DM, et al. Effect of
cranial tibial closing wedge angle on tibial subluxation: An ex vivo study. Vet Surg 2010;39:454–459.
Bailey CJ, Smith BA, Black AP. Geometric implications of the tibial wedge osteotomy for the treatment of cranial cruciate ligament disease in dogs.
Vet Comp Orthop Traumatol 2007;20:169–174.
Bruce W, Rose A, Tuke J, et al. Evaluation of the triple
tibial osteotomy. A new technique for the management of the canine cruciate-deficient stifle. Vet
Comp Orthop Traumatol 2007;20:159–168.
Corr SA, Brown C. A comparison of outcomes following tibial plateau levelling osteotomy and cranial tibial wedge osteotomy procedures. Vet Comp
Orthop Traumatol 2007;20:312–319.
Frederick SW, Cross AR. Modified cranial closing
wedge osteotomy for treatment of cranial cruciate
ligament insufficiency in dogs with excessive tibial
plateau angles: Technique and complications in 19
cases. Vet Surg 2017;46:403–411.
Kuan S, Smith B, Black A. Tibial wedge ostectomy:
complications of 300 surgical procedures. Aust Vet
J 2009;87:438–444.
Macias C, McKee WM, May C. Caudal proximal tibial
deformity and cranial cruciate ligament rupture in
small-breed dogs. J Small Anim Pract 2002;43:433–
438.
Moles AD, Hill TP, Glyde M. Triple tibial osteotomy
for treatment of the canine cranial cruciate
ligament-deficient stifle joint. Vet Comp Orthop
Traumatol 2009;22:473–478.
Oxley B, Gemmill TJ, Renwick AR, et al. Comparison
of complication rates and clinical outcome between
tibial plateau leveling osteotomy and a modified
cranial closing wedge osteotomy for treatment of
cranial cruciate ligament disease in dogs. Vet Surg
2013;42:739–750.
Read RA, Robins GM. Deformity of the proximal tibia
in dogs. Vet Rec 1982;111:295–298.
Renwick AI, McKee WM, Emmerson TD, et al. Preliminary experiences of the triple tibial osteotomy
procedure: tibial morphology and complications.
J Small Anim Pract 2009;50:212–221.
Slocum B, Devine T. Cranial tibial wedge osteotomy:
a technique for eliminating cranial tibial thrust in
cranial cruciate ligament repair. J Am Vet Med
Assoc 1984;184:564–569.
VetBooks.ir
30
Treatment of Excessive Tibial
Plateau Angle
Michael P. Kowaleski
Introduction
The proximal tibial articular surface is angulated distally with respect to the mechanical axis
of the tibia; the magnitude of this angulation is
termed the tibial plateau angle (TPA). The mean
TPA in dogs has been reported to range from
23.5◦ to 28.3◦ , with individual dogs having a
TPA as low as 12◦ or as high as 46◦ (Pacchiana
et al. 2003; Priddy et al. 2003; Reif & Probst 2003;
Moeller et al. 2006; Stauffer et al. 2006). The morphology of the proximal tibia in dogs with a
steep tibial plateau slope can be distinctly different than normal dogs (Figures 30.1A and 30.2A)
(Osmond et al. 2006). Affected dogs may have a
steep TPA and/or a proximal tibial shaft deformity in which the cranial border of the tibia
is angulated from caudal to cranial rather than
the more typical proximal to distal orientation
(Read & Robins 1982; Osmond et al. 2006).
Slocum1 defined excessive tibial plateau
angle (eTPA) as a TPA greater than 34◦ when
using a 24-mm radius tibial plateau leveling
osteotomy (TPLO) blade. However, this definition does not account for individual variation
1 Seminars
entitled “Tibial Plateau Leveling Osteotomy
for Cranial Cruciate Ligament Repair,” Slocum Enterprises, Inc.
in proximal tibial anatomy. After the TPLO procedure, the tibial plateau segment acts as a buttress to support the tibial tuberosity (Talaat et al.
2006; Hamilton et al. 2015). The point of insertion of the patellar tendon on the tibial tuberosity has been suggested as a safe point (maximum) for rotation (Figure 30.2A,B) to reduce
the risk of tibial tuberosity fracture (Talaat et al.
2006). This has been substantiated in a mechanical study on the effect of osteotomy position
and tibial plateau rotation on the tensile force
required for failure of the canine quadriceps
mechanism (Hamilton et al. 2015). This ex vivo
study revealed that rotation of the tibial plateau
segment below the patellar tendon insertion
decreased the force required for tibial tuberosity fracture, supporting the idea of a safe point,
with the tibial plateau providing buttress to the
tibial tuberosity (Hamilton et al. 2015).
Preoperative planning
Preoperative planning can be used to determine the chord length corresponding to the
safe rotation distance. A tibial osteotomy guide
is centered on the point dividing the intercondylar tubercles, at the intersection of the
tibial mechanical axis and tibial plateau axis
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
253
VetBooks.ir
254
Surgical Treatment
(A)
(B)
(C)
(D)
(E)
(F)
(G)
Figure 30.1 Tibial plateau leveling osteotomy (TPLO) and closing cranial wedge ostectomy (CCWO) for the treatment
of excessive tibial plateau angle (eTPA). Preoperative mediolateral (A) and caudocranial (B) views of a large-breed patient
with cruciate ligament rupture and eTPA. Preoperative planning for TPLO/CCWO (C); Note that the safe distance S has
been identified (black, double-ended arrow). Postoperative (D and E) and follow-up (F and G) radiographs taken 8 weeks
postoperatively revealing osteotomy healing with stable implants.
VetBooks.ir
Treatment of Excessive Tibial Plateau Angle
(A)
(B)
255
(C)
Figure 30.2 Safe and required rotation. The osteotomy is positioned (black dashed line) and a line perpendicular to the
tibial crest is drawn at the level of patellar tendon insertion (white line) (A). The safe distance, S (white double-ended
arrow), is the linear distance (chord) from the osteotomy exit at the cranial intercondyloid area to the intersection of the
line drawn perpendicular to the tibial crest at the patellar tendon insertion, referred to as the safe point (A). The tibial
plateau segment has been rotated to the safe point (safe rotation) (B). The tibial plateau segment has been rotated well
below the safe point (required rotation) to achieve a tibial plateau angle of 5◦ (C).
(proximal tibial joint reference line) or at
any location between these two points (Figure 30.2A). The location is selected that optimizes the tibial tuberosity and tibial plateau
size and shape. In cases of severe tibial deformity, alternate tibial osteotomy locations may
be needed (Figures 30.1C and 30.2A). Once the
tibial osteotomy is properly positioned, a line is
drawn caudally from the patellar tendon insertion on the tibial tuberosity, perpendicular to the
tibial crest to intersect with the osteotomy template (Figure 30.2A). The linear distance from
the point at which the osteotomy exits the tibia
within the cranial intercondyloid area to the
intersection of the line drawn perpendicular to
the tibial crest at the point of patellar tendon
insertion and the osteotomy template is the safe
rotation distance (S in Figure 30.2A).
The safe TPA (sTPA) is the tibial plateau
angle that can be treated by this magnitude of
VetBooks.ir
256
Surgical Treatment
rotation (Figure 30.2B), and this can be determined by identifying the safe rotation distance
in the appropriate saw blade size (radius) row
in the TPLO chart; the sTPA is the preoperative TPA that corresponds to this rotation
distance.
If the required rotation chord length (the rotation needed to achieve a TPA of 5◦ ) is significantly greater than the safe rotation cord length
(Figure 30.2C), a TPLO combined with a closing cranial wedge ostectomy (TPLO/CCWO)
should be considered (Talaat et al. 2006). The
angle of the CCWO is the difference between
the preoperative TPA and the sTPA. By utilizing the TPLO/CCWO procedure, the magnitude of both the TPLO and CCWO can be
adjusted to correct the TPA and proximal tibial deformity as needed, based on individual patient anatomy. In a retrospective study
evaluating treatment options for eTPA, outcome, based on owner assessment, was superior
with ‘full-rotation TPLO’ (correction of the TPA
to less than 14◦ ) compared to ‘under-rotated
TPLO’ (leveling to >14◦ ) (Duerr et al. 2008), and
supplemental fixation with additional implants
was associated with a lower complication rate
(Duerr et al. 2008). Additionally, this procedure
can be simultaneously combined with a medial
or lateral closing wedge ostectomy to address
moderate to severe proximal tibial varus or valgus, and/or moderate to severe tibial torsion
(Figure 30.3) (Weh et al. 2011).
(A)
(B)
(C)
(D)
(E)
Figure 30.3 Diagrammatic representation of a proximal tibial valgus deformity treated by tibial plateau leveling
osteotomy (TPLO) and a coplanar medial wedge ostectomy. The apex of the medial closing wedge is coincident with the
exit of the TPLO radial osteotomy at the caudolateral tibial cortex. Tibial torsion can be corrected at the level of the
medial closing wedge (arrows) without loss of apposition at the radial osteotomy. The inset depicts various closing wedge
configurations: (A) Coplanar cranial closing wedge. (B) Coplanar lateral closing wedge. (C) Coplanar medial closing
wedge. (D) Biplanar medial and cranial closing wedge. (E) Biplanar lateral and cranial closing wedge. Source: Weh et al.
2011. Reproduced with permission from John Wiley & Sons, Inc.
VetBooks.ir
Treatment of Excessive Tibial Plateau Angle
The case example illustrates a patient with a
TPA of 41◦ and a safe rotation of 11 mm (S in Figure 30.1C). Referring to the TPLO chart for a 30mm saw blade, a rotation of 10.8 mm is the correction for a TPA of 26◦ . Therefore, a CCWO of
15◦ combined with a TPLO rotation of 10.8 mm
(TPLO for 26◦ + 15◦ CCWO = correction for preoperative TPA of 41◦ ) would result in a postoperative TPA of approximately 5◦ with a safe
rotation; thus, a CCWO of 15◦ was chosen for
this patient (Figure 30.1C). The CCWO is positioned such that the apex is placed at the caudal
cortical exit of the TPLO (Figure 30.1C).
In cases with significant varus or valgus and
eTPA, the tibial wedge ostectomy can be performed as a biplanar CCWO, rather than as a
coplanar CCWO (Figure 30.3D,E) (Weh et al.
2011), to correct for the angular deformity in
the frontal plane. When performing a biplanar CCWO, the angular correction is typically
257
performed by angulating the distal limb of the
CCWO (rather than the proximal limb) to avoid
the angled osteotomy from entering into the
radial osteotomy of the TPLO. In cases with significant varus or valgus without eTPA, the tibial closing wedge ostectomy can be a coplanar
medial closing wedge (valgus correction) (Figure 30.3C) or lateral closing wedge (varus correction) (Figure 30.3B) (Weh et al. 2011). The distal jig pin beyond (i.e., medial to) the jig arm can
be bent to the angle of correction required, and
this bent pin can be used as a reference for saw
angulation while performing the osteotomy.
Alternatively, a Kirschner wire can be inserted
into the tibia at the desired angle, or an additional jig pin can be placed and used for a reference (Weh et al. 2011) (Figure 30.4). In cases with
concurrent tibial torsion, the correction can be
made at the opposing surfaces of the linear tibial
osteotomy; this results in a correction of torsion
(A)
(B)
(C)
(D)
(E)
(F)
(G)
Figure 30.4 Three-jig pin technique for tibial plateau leveling osteotomy (TPLO) with correction of significant tibial
valgus. The proximal and middle (articulated with distal jig arm) jig pins are placed parallel to the tibial plateau in the
frontal plane, and are parallel to each other (A and B). The third jig pin (distal-most jig pin, not articulated with TPLO jig)
is placed parallel to the talo-crural joint (A and B). The angle formed between the middle and distal jig pins is equal to
the correction angle (B). The TPLO (C) and proximal arm of the medial closing wedge (D) are performed parallel to the
proximal (and/or middle) jig pin. The distal limb of the medial closing wedge is performed parallel to the distal jig pin (E),
creating the medial closing wedge (F). The TPLO jig is re-articulated with the distal jig pin, reducing the medial closing
wedge ostectomy (G), and fixation is applied.
VetBooks.ir
258
Surgical Treatment
without any loss of bone apposition at the TPLO
(arrows in Figure 30.3) (Weh et al. 2011). In
cases with patella alta, the closing wedge can be
used to position the patella more distally in the
trochlear groove; the amount of change in patellar position is roughly equivalent to the distance
of cranial tibial cortex that is removed with the
CCWO (Talaat et al. 2006). Thus, the angle of the
CCWO can be adjusted to provide the necessary
change in patellar position, and the rotation at
the TPLO can be adjusted to provide the balance
of the tibial plateau leveling required achieving a postoperative TPA of 5◦ , without rotating
beyond the safe point.
Surgical technique
Slocum & Slocum (1993) were the first to
describe the TPLO/CCWO procedure utilizing
two radial osteotomies.2 However, this technique was shown to result in unpredictable
and inaccurate correction (Talaat et al. 2006),
and consequently it was modified to use linear
osteotomies at the CCWO (Talaat et al. 2006).
This was found to make preoperative planning and intraoperative execution more precise.
Once the radial osteotomy for the TPLO is made
partially through the tibia, the proximal limb
of the CCWO is scored on the medial cortex,
such that it intersects the radial osteotomy of
the TPLO at the caudal cortex of the tibia. The
CCWO can be accurately executed intraoperatively by using a sterile angle template, a sterile goniometer, or a simple geometric method.
If the geometric method is used, the proximal
limb of the CCWO must be placed such that it
is perpendicular to the cranial tibial cortex (Figure 30.1C). The length of the proximal limb of
the CCWO (base of a right-triangle) is measured
and the length of the opposite limb of the righttriangle (the limb of the triangle along cranial
border of the tibia) is calculated (Figure 30.1C),
determining the appropriate position of the distal limb of the CCWO (hypotenuse of the triangle), which is then scored. The TPLO is completed, the tibial plateau segment is rotated, and
2 Seminars
entitled “Tibial Plateau Leveling Osteotomy
for Cranial Cruciate Ligament Repair,” Slocum Enterprises, Inc.
two holding Kirschner wires are placed from
proximal to the patellar tendon attachment at
the tibial tuberosity into the tibial plateau segment. It should be noted that the plateau is not
leveled to 5◦ at this stage, and care must be taken
to ensure that the Kirschner wires do not penetrate the joint surface. These Kirschner wires
remain as part of the permanent fixation. The
CCWO is completed, reduced, and a holding
Kirschner wire is placed from craniodistal to
caudoproximal, avoiding the articular surface
(Figure 30.1D). Two large-gauge tension band
wires are applied to achieve cranial compression and apposition of the tibial closing wedge
osteotomy. The bone plate(s) are then applied in
compression to complete the stabilization (Figure 30.1D,E). Application of the implants in this
order seems to improve osteotomy apposition
and healing (Weh et al. 2011).
The CCWO wedge can be morselized and
placed as autogenous corticocancellous bone
graft at the osteotomy sites, particularly at the
CCWO site, as this is generally the area that
heals most slowly (Figure 30.1D,E). Torsional
correction at the CCWO (arrows in Figure 30.3)
and/or lateral translation of the tibial tuberosity segment can be accomplished before applying the fixation, facilitating limb alignment correction in complex cases, such as severe tibial
torsion or medial patellar luxation with cruciate ligament rupture in which tibial tuberosity
transposition is required.
Rigid fixation is required in cases treated with
TPLO/CCWO to mitigate the risk of implant
loosening, fixation failure, or prolonged healing. In particular, fixation of the cranial tibial
tuberosity segment must be rigid, since the distractive force of the patellar tendon is considerable. Therefore, in all cases, the Kirschner wires
placed to stabilize the TPLO and CCWO during the procedure are maintained as permanent
fixation, and two figure-of-eight tension band
wires are placed to counteract this strong distractive force. The Kirschner wires and tension
band wires should be of a suitably large gauge
(1/16′′ or 3/32′′ Kirschner wires/pins and 18-g
or 16-g cerclage wire in most patients), tightened adequately, and anchored in bone tunnels
as illustrated (Figure 30.1D,E). Double plate fixation is recommended if the tibial size is sufficient to place a second bone plate. In patients
weighing 30–40 kg an additional 2.4-mm or
VetBooks.ir
Treatment of Excessive Tibial Plateau Angle
2.7-mm straight bone plate can be added to
the standard 3.5-mm TPLO plate, or a 3.5-mm
broad TPLO plate can be used. In most patients
weighing >40 kg an additional 3.5-mm straight
bone plate can be added to the standard 3.5-mm
TPLO plate.
Outcome
A multicenter, case-control study compared the
surgical treatment options for cruciate ligament
rupture in larger-breed dogs with eTPA, and
found that surgical treatment had a higher complication rate but a comparable outcome to
that of dogs without eTPA. In addition, ownerperceived outcome was superior for eTPA dogs
when TPLO resulted in a TPA ≤14◦ , compared
to dogs with postoperative TPA >14◦ . Therefore,
TPLO/CCWO with a target TPA of 5◦ is the procedure of choice of the author. In a retrospective
study evaluating the TPLO/CCWO procedure
in 18 stifles of 15 dogs, postoperative complications included implant loosening or breakage
(27.8%), seroma formation (11.1%), and local
irritation due to implants (11.1%) (Talaat et al.
2006). Anecdotally, as more experience has been
gained with this technique, the complication
rate is considerably lower, and is now similar
to that reported for TPLO alone, with the occasional need for Kirschner or tension band wire
removal being the most common complication.
References
Duerr FM, Duncan CG, Savicky RS, et al. Comparison
of surgical treatment options for cranial cruciate
ligament disease in large-breed dogs with excessive tibial plateau angle. Vet Surg 2008;37:49–62.
Hamilton K, Tarlton J, Parsons K, et al. Effect of
osteotomy position and tibial plateau rotation on
259
the tensile force required for failure of the canine
quadriceps mechanism. Vet Surg 2015;44:763–771.
Moeller EM, Cross AR, Rapoff AJ. Change in tibial plateau angle after tibial plateau leveling
osteotomy in dogs. Vet Surg 2006;35:460–464.
Osmond CS, Marcellin-Little DJ, Harrysson OLA,
et al. Morphometric assessment of the proximal
portion of the tibia in dogs with and without cranial
cruciate ligament rupture. Vet Radiol Ultrasound
2006;47:136–141.
Pacchiana PD, Morris E, Gillings SL, et al. Surgical and
postoperative complications associated with tibial
plateau leveling osteotomy in dogs with cranial
cruciate ligament rupture: 397 cases (1998–2001).
J Am Vet Med Assoc 2003;222:184–193.
Priddy NH, Tomlinson JL, Dodam JR, et al. Complications with and owner assessment of the outcome
of tibial plateau leveling osteotomy for treatment of
cranial cruciate ligament rupture in dogs: 193 cases
(1997–2001). J Am Vet Med Assoc 2003;222:1726–
1732.
Read RA, Robins GM. Deformity of the proximal tibia
in dogs. Vet Record 1982;111:295–298.
Reif U, Probst CW. Comparison of tibial plateau
angles in normal and cranial cruciate deficient stifles of Labrador Retrievers. Vet Surg 2003;32:385–
389.
Slocum B, Slocum TD. Tibial plateau leveling
osteotomy for repair of cranial cruciate ligament
rupture in the canine. Vet Clin North Am Small
Anim Pract 1993;23:777–795.
Stauffer KD, Tuttle TA, Elkins AD, et al. Complications associated with 696 tibial plateau leveling
osteotomies (2001–2003). J Am Anim Hosp Assoc
2006;42:44–50.
Talaat MB, Kowaleski MP, Boudrieau RJ. Combination tibial plateau leveling osteotomy and cranial closing wedge osteotomy of the tibia for the
treatment of cranial cruciate ligament-deficient stifles with excessive tibial plateau angle. Vet Surg
2006;35:729–739.
Weh JL, Kowaleski MP, Boudrieau RJ. Combination
tibial plateau leveling osteotomy and transverse
corrective osteotomy of the proximal tibia for the
treatment of complex tibial deformity in 12 dogs.
Vet Surg 2011;40:670–686.
VetBooks.ir
VetBooks.ir
31
Surgical Management of
Cruciate Ligament Rupture
Combined with Patella
Luxation
Anke Langenbach and Denis J. Marcellin-Little
Pathophysiology
Cruciate ligament rupture (CR) predominantly
affects the cranial cruciate ligament (CrCL).
CR and patellar luxation (PL) are two common
causes of dysfunction and lameness in dogs
that are generally independent but can coexist
(Arthurs & Langley-Hobbs 2006). Medial and
lateral PL have been described as risk factors
for CR (Wright 1979; Willauer & Vasseur 1987).
Conversely, CR can predispose dogs to patellar
luxation, particularly in bow-legged dogs. The
prevalence of PL in dogs with CR ranged from
6% to 20% in two reports (Willauer & Vasseur
1987; Gibbons et al. 2006). Pelvic limb lameness
in dogs with combined CR and PL may be
more severe than pelvic limb lameness in dogs
with only CR or only PL. It has been speculated
that the increase in internal rotation resulting
from partial CrCL fiber rupture may increase
clinical signs in dogs with Grade 1 medial
PL and no previous clinical signs. Complete
CR leads to stifle instability, primarily with
cranial tibial thrust but also with an increase
in internal rotation and extension, potentially exacerbating the clinical consequences
of PL.
Patellae that track in an abnormally proximal
position (patella alta) are also a risk factor for
medial PL. In one report, large-breed dogs with
medial PL were found to have a more proximal patella than large-breed dogs with normal
stifle joints (Johnson et al. 2006). However, in
another report, patella alta was not identified
in toy poodles with medial PL (Yasukawa et al.
2016). PL has also been reported as an unusual
postoperative complication of CR stabilization
surgery. The proposed mechanism for postoperative PL included a failure of incisional closure
or tearing of the retinacular incision, potentially
combined with muscle atrophy with a resulting lack of muscular control. Additional predisposing factors include angulation of the proximal or distal portion of the femur, a shallow
trochlear sulcus with poorly developed ridges,
hypoplastic femoral condyles, and torsion of
the tibial tuberosity or bowing of the proximal tibia. PL after CR stabilization can be either
medial or lateral and can occur after extracapsular stabilization, intra-articular stabilization, tibial plateau leveling osteotomy (TPLO),
or closing cranial wedge ostectomy (Arthurs &
Langley-Hobbs 2007). An incidence of PL of
1.3% was documented during the development
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
261
VetBooks.ir
262
Surgical Treatment
period of the TPLO procedure (Slocum &
Slocum 1993). In two large studies, the reported
incidence of PL after a variety of CR stabilization methods was 0.18% and 0.3%, respectively
(Arthurs & Langley-Hobbs 2007; Fitzpatrick &
Solano 2010).
Patient evaluation
Clinical signs
Patients with combined CR and PL often have
no history of trauma and present with an acute
unilateral pelvic limb lameness after exercise.
In two studies, the mean age at presentation
was 19 and 24 months, respectively (Fitzpatrick
et al. 2010; Langenbach & Marcellin-Little 2010).
By comparison, dogs presenting because of CR
alone tend to be older: the median age at presentation for dogs with CR was 67 months in a
study involving 1000 dogs (Fitzpatrick & Solano
2010). Owners may report occasional to frequent skipping and hopping on the affected leg
before CR, suggesting that the PL preceded CR.
The duration of lameness varies from acute to
chronic lameness lasting several months. Combined CR and PL has been reported in several
breeds. Labrador Retrievers are the most commonly affected dogs. In the authors’ experience,
English Bulldogs and American Pit Bull Terriers
are also commonly affected. These two breeds
were also the most common in a study describing the management of combined medial PL
and CR using TTA (Yeadon et al. 2011).
Physical examination findings include cranial
tibial thrust, positive cranial drawer motion and
PL with varying degrees of luxation. Grades
2 and 3 are most common, but Grades 1 and
4 have also been reported. In dogs with combined CR and PL most luxations are medial,
but lateral PL is possible. In one report, two
lateral PL were described as a complication of
CR stabilization surgery: one in a Bull Mastiff and one in a sighthound cross (Lurcher)
(Arthurs & Langley-Hobbs 2007). However, in
a report of 65 dogs with lateral PL, no dog had
concurrent CR (Kalff et al. 2014). In that report,
a breed shift from large and giant breeds to
medium and large breeds was described: the
most commonly affected breed was the Cocker
Spaniel.
Palpation
The diagnosis of combined CR and PL is
made by palpation. Pelvic limb radiographs are
needed to provide an adequate understanding
of the condition and underlying deformities,
and to select treatment options. PL are graded
using Putnam’s grades: Grade 1 being manual dislocation of the patella with spontaneous
reduction upon release; Grade 2 being the spontaneous and frequent PL with self-reduction;
Grade 3 being a near-constant luxation that can
be manually reduced; and Grade 4 being a permanent luxation (Putnam 1968).
Imaging
For dogs with combined CR and PL, the focus
of assessment is to detect malalignment of the
quadriceps femoris extension apparatus. This
includes angulation and torsion of the femur,
tibial tuberosity malposition, and angulation
and torsion of the tibia. The minimum valgus or varus femoral or tibial angles leading
to medial or lateral PL are not known. Assessment of femoral and tibial geometry can be
made using radiographs or computed tomography (CT) scanning. Radiographs should ideally
be made under sedation or general anesthesia
to allow for correct alignment and positioning.
A change in distal femoral elevation influences
the measurement of mediolateral angulation
of the femoral shaft (Jackson & Wendelburg
2012). In that study, measurements of the
anatomic lateral distal femoral angle (aLDFA)
were increased when the distal aspect of the
femur was elevated by >5◦ . A 10◦ elevation led
to an increase in aLDFA of ∼1◦ . Radiographic
views of the femurs and tibias are warranted
because limb conformation is often abnormal,
and because the problem is generally bilateral.
For the femur and tibia, angulation in a frontal
plane is assessed by use of a craniocaudal (CC)
radiographic view by evaluating lateral deviation (valgus) or medial deviation (varus) of the
lower extremity relative to the proximal portion of the bone. This has been done using the
aLDFA and mechanical lateral distal femoral
angle (mLDFA) (Palmer et al. 2011). For the
tibia, angulation in a frontal plane is evaluated by measuring the relative orientation of
VetBooks.ir
Surgical Management of Cruciate Ligament Rupture Combined with Patella Luxation
the tibial plateau and distal articular surface
on a CC radiographic view (Jaeger et al. 2007).
The mechanical medial proximal tibial angle
(mMPTA) and mechanical medial distal tibial
angle (mMDTA) can be calculated for the tibia
on CC view after drawing the mechanical tibial
axis from the center of the intercondylar fossa
of the femur through the intertubercular eminence of the tibia and the distal intermediate
ridge of the tibia (Dismukes et al. 2007; Dismukes et al. 2008a). CC radiographic views of
the complete femur with coxofemoral and stifle joints and complete tibia with stifle and hock
joints are recommended. This may require two
radiographs, since many dogs are too large to
be imaged on one large radiographic plate. The
radiographic beam should be centered over the
stifle joint and the femoral cortices should bisect
the fabellae. However, it may be difficult to
accurately assess varus angulation of the femur
by use of CC radiographs (Aiken & Barnes
2014). In dogs with Grade 2, 3, or 4 medial PL,
the patella may luxate during imaging, making evaluation of the shape of the femur more
challenging because it is more difficult to orient the femur (Figure 31.1). Varus and valgus
femoral angulation is assessed on the CC view
of the femur. That assessment includes measurement of the anatomic long axis of the femur
and the aLDFA (Figure 31.2) (Tomlinson et al.
2007). The mean aLDFA reportedly is 97◦ in
Labrador Retrievers and 93◦ in German Shepherd dogs (Tomlinson et al. 2007). In one study,
the mean aLDFA, mLDFA and femoral varus
angle obtained using CT imaging in Toy Poodles with Grade 2 medial PL did not differ statistically from that of normal Toy Poodles, but they
were 15◦ larger for Toy Poodles with Grade 4
medial PL (Yasukawa et al. 2016). Hip dysplasia
with low femoral neck inclination (coxa vara)
and low femoral head anteversion angles has
been associated with medial PL (Roush 1993;
Kaiser et al. 2001). However, CT-based review
of femoral shape in Toy Poodles with medial
PL identified no association between medial PL
and hip dysplasia (Yasukawa et al. 2016). Varus
orientation of the tibia is determined by measuring the mMPTA and mMDTA on a CC view and
the mechanical cranial distal tibial angle and the
mechanical proximal tibial angle on the sagittal or mediolateral view (Dismukes et al. 2008b).
A mediolateral view of the entire femur with
263
Figure 31.1 Craniocaudal radiographic view of the
femur of 1-year-old male Akita Inu with medial patellar
luxation. The patella is medial to the medial trochlear
ridge, and it is therefore more challenging to determine
whether the view of the distal portion of the femur is truly
craniocaudal.
the coxofemoral joint and stifle joints included
and a mediolateral view of the tibia with stifle and hock joints included are also recommended. Mediolateral views with the femoral
condyles superimposed are recommended, but
these may be difficult to obtain in dogs with
torsional or angular deformities of the femur.
A ‘condylar offset sign’ may be seen in cases
of femoral torsion, in that in a mediolateral
projection one of the femoral condyles is offset cranially or distally in relation to the other.
Excessive femoral varus results in a distal offset, whereas femoral torsion or underdevelopment of the medial or lateral trochlear ridge
results in a cranial offset (Figure 31.3). Femoral
264
Surgical Treatment
VetBooks.ir
torsion is assessed using an axial radiographic
view of the femur (Dudley et al. 2006). This is
done by placing the patient in dorsal recumbency with the radiographic plate under the
hip region and by centering the radiographic
beam on the femur. CT scanning allows a tridimensional assessment of the femur and tibia
(Harrysson et al. 2003), and greatly enhances
the repeatability of the assessment of angulation and torsion of the femur and tibia, compared to radiographs (Dudley et al. 2006; Barnes
et al. 2015). The CT scan can be exported and
used to produce a replica of the bone to rehearse
surgery (Harrysson et al. 2003).
Management
Figure 31.2 Craniocaudal radiograph of a
Newfoundland with combined cruciate ligament rupture
and medial patella luxation. Femoral length is measured
as the distance from the proximal aspect of the
intercondylar fossa to the laterodistal aspect the femoral
neck (open circles). The anatomic axis of the femur is
drawn as the line connecting the center of two lines
drawn across of the femoral shaft at one-third and
one-half of femoral length. The distal joint reference line
is the line connecting the distal aspect of the medial and
lateral femoral condyles. The anatomic lateral distal
femoral angle (aLDFA) is the angle formed by the
anatomic axis of the femur (solid white line) and the
distal joint reference line. The mechanical axis of the
femur is drawn as the dotted line connecting the center of
the femoral head and the proximal aspect of the
intercondylar fossa. The mechanical lateral distal femoral
angle (mLDFA) is the angle formed by the mechanical
axis and the distal joint reference line. In this dog, the
aLDFA is 108◦ and the mLDFA is 105◦ . Both angles are
abnormally high.
Management options are either non-surgical or
surgical. For Grade 1 PL with partial or complete CR, focusing on quadriceps strengthening as part of a rehabilitation program could
be a viable option. A stifle brace may be considered, but little is known about the benefits
of braces. Braces are particularly challenging to
fit in small patients and in patients with short,
bulky limbs. Medium and large dogs can be fitted with a brace and can be managed with controlled activity and therapeutic exercises over a
period of 8–12 weeks. Physical rehabilitation of
dogs with CR is described in Chapter 42. Surgical treatment of dogs with Grade 2, 3, or 4
PL combined with complete CR with meniscal
injury is generally required to regain stability of
the stifle joint. Several treatment options have
been reported which focus on realignment of
the quadriceps mechanism while stabilizing the
CrCL-deficient stifle. The surgery should prevent cranial tibial thrust and torsional instability (pivot shift) while maintaining normal range
of motion of the stifle joint.
Stabilization of the CrCL-deficient stifle joint
combined with PL is challenging because technical steps from both surgical procedures must
be combined when joint stability is surgically
reestablished. The trochlear groove is often
shallow, with a compromised medial or lateral
trochlear ridge. This may be developmental
or the result of wear caused by friction of the
patella on the trochlear ridge (Figure 31.4). To
restore patellar tracking, the trochlear groove
may need to be deepened; this is ideally
265
VetBooks.ir
Surgical Management of Cruciate Ligament Rupture Combined with Patella Luxation
(A)
(B)
(C)
Figure 31.3 In dogs with normal femoral angulation and torsion (A), the condyles are often superimposed on
mediolateral radiographs of the femur. In contrast, in dogs with excessive femoral angulation or torsion and in dogs with
abnormal condylar development, the femoral condyles are often offset. A distal femoral condylar offset is present in dogs
with excessive femoral angulation (varus or valgus) (B). The extensor fossa at the origin of the long digital extensor
muscle on the lateral condyle is visible (arrowhead), indicating that the shorter condyle is the medial condyle and that
the dog has excessive varus. A cranial femoral condylar offset is present in dogs with femoral torsion (C). The extensor
fossa on lateral condyle (arrowhead) is more cranial than the medial condyle, indicating the presence of excessive
internal rotation of the distal portion of the femur.
achieved with minimal disruption to the articular surface using trochlear block or wedge
resection (Johnson et al. 2001). The groove
should be wide enough to allow the patella to
contact the trochlea, and deep enough for at
least half of the thickness of the patella to be caudal to the medial and lateral trochlear ridges.
(A)
(B)
The trochlear groove should also be proximally
extended to accommodate the potentially proximal patella in large-breed dogs with medial
PL. The cranial part of the sartorius muscle may
be released near its insertion site if the muscle
appears to promote internal rotation of the tibia,
or prevent stifle joint extension.
(C)
Figure 31.4 In these intraoperative pictures of a patient with Grade 3 MPL and CR made during arthroscopy, the
articular cartilage of the trochlea is slightly irregular (A, bottom). The articular cartilage of the patella is completely
eroded (B). Full-thickness articular cartilage wear is also visible on the medial aspect of the medial trochlear ridge, where
the patella rests in its luxated position (C).
VetBooks.ir
266
Surgical Treatment
Femoral torsion and angulation are routinely
abnormal in dogs with CR and PL. Bow-legged
dogs have varus angulation of the distal portion
of the femur combined with internal torsion
(genu varum) (Read & Robbins 1982). Knockkneed dogs have valgus angulation of the distal
portion of the femur combined with external
torsion (genu valgum) (Kalff et al. 2014). Correct patellar tracking requires realignment of
the trochlear groove. Minor trochlear groove
malalignment can be corrected by angling the
trochlear block or wedge, while major trochlear
groove malalignment is best managed with a
corrective ostectomy of the distal portion of
the femur (Swiderski & Palmer 2007), potentially combined with trochlear block or wedge
recession.
Stabilization of the CrCL-deficient stifle and
the correction of deformities of proximal portion of the tibia require a combination of
surgical procedures. If necessary, the quadriceps mechanism is realigned through transposition of the tibial tuberosity. In dogs with
medial PL, lateralization of the tuberosity is
(A)
(B)
often performed; conversely, in dogs with lateral luxation, the tuberosity is moved medially. The tuberosity is also displaced distally
in patients with patella alta. Distal transposition can be achieved with tibial tuberosity
osteotomy, angling the osteotomy and then
repositioning the tuberosity and securing it
using Kirschner wires or a tibial tuberosity
advancement (TTA) plate. If tibial anatomy is
within normal limits but rotational laxity of the
stifle joint is present, the tibial position can be
controlled using a fabellar-to-tibial crest suture,
which will also provide extracapsular stabilization of cranial tibial translation when CR is
present (see also Chapter 25).
TPLO can also be used to manage dogs with
combined CR and PL, particularly medial PL
in large dogs (Figure 31.5) (Fitzpatrick et al.
2010; Langenbach & Marcellin-Little 2010). A
medial skin incision, followed by a lateral
arthrotomy of the stifle joint, is performed to
allow for trochleoplasty or corrective closing
wedge femoral ostectomy, and inspection of
intra-articular structures including the CrCL
(C)
(D)
Figure 31.5 Mediolateral radiographs of the tibiae of a 3-year-old Bulldog with bilateral rupture of the cranial cruciate
ligament combined with medial patellar luxation. Tibial plateau leveling osteotomy (TPLO) has been performed on the
right (A and B) and left (C and D) legs. A ‘right-sided’ TPLO plate has been used to stabilize the tibial plateau of the left
leg (D) and synthetic bone graft is visible at the surgical site.
VetBooks.ir
Surgical Management of Cruciate Ligament Rupture Combined with Patella Luxation
Figure 31.6 Realignment of the
tibia when performing tibial
plateau leveling osteotomy
(TPLO) combined with patella
luxation correction includes
several steps performed while the
patella is in its reduced position
and the stifle joint is held in
extension and facing cranially.
First, an assistant stabilizes the
tibial plateau in its leveled
position while the surgeon
externally rotates the distal tibia
around its long axis to eliminate
internal torsion of the tibia.
Second, the surgeon slides the
tibial plateau 3–6 mm medially,
laterally translating the tibial
tuberosity and the entire distal
fragment. Third, to address genu
varum, the distal fragment is
moved abaxially against the
tibial plateau, creating a medial
gap of 1–3 mm (A). After the
procedure is completed, a
stabilizing Kirschner wire is
inserted from the tibial crest into
the tibial plateau (B). Source:
Adapted from Langenbach &
Marcellin-Little 2010.
(A)
and medial meniscus. A cranial sartorius muscle release and lateral retinacular imbrication
are then performed. A medial approach to the
proximal portion of the tibia is made and a
TPLO is performed. The appropriate osteotomy
position is measured on radiographs before
surgery (Mossman et al. 2015). Once the tibial
plateau is freed, the jig is removed to allow rotation of the plateau. An assistant stabilizes the
thigh while the surgeon carefully levels the tibial plateau and realigns the proximal and distal portions of the tibia to correct tibial torsion and varus (Figure 31.6). The construct is
secured with a 1.14 mm- or 1.55 mm-diameter
(0.045′′ or 0.062′′ ) Kirschner wire, depending on
patient size, placed from the craniolateral aspect
of the tibial crest into the central tibial plateau.
A stainless steel rod is used to check for correct alignment in surgery of the tibia and femur.
The patella is checked for stability. Once alignment is achieved, a TPLO plate is applied. A
pre-contoured locking TPLO plate can be used,
but this may need to be adjusted using bending
irons to fit the tibia. Plate contouring leads to
267
(B)
a change in the orientation of locking screws.
This may lead to an inappropriate screw orientation in the proximal bone fragment. Consequently, it may necessary to use non locking
screws in the proximal portion of the plate to
ensure appropriate screw orientation. In some
instances, a pre-contoured TPLO plate intended
for the opposite side can be used (Figure 31.5D).
An alternative approach is to perform a standard TPLO and then correct the patella luxaton
using a frontal plane tibial tuberosity transposition (Leonard et al. 2016). The tibial crest fragment is stabilized using pin and tension band
wire fixation (Leonard et al. 2016).
If a closing wedge ostectomy of the femur
is performed in the same patient, the wedge
can be morselized and used as graft in the
medial cortical defect. Alternatively, a synthetic bone graft can be used to fill the medial
defect between the distomedial aspect of the
tibial plateau and the proximomedial aspect
of the tibial shaft. The Kirschner wire can be
left in place to enhance stability, or it can be
removed.
VetBooks.ir
268
Surgical Treatment
TTA can also be used to manage CR combined with PL (Newman et al. 2014). The management of medial PL and CR often requires fixation of the tibial tuberosity in a more lateral
and distal position. A medial approach to the
stifle and proximal tibia is performed with lateral dissection and lateral arthrotomy of the stifle joint. Any CrCL remnants are removed, and
a block resection sulcoplasty is performed. A
tibial tuberosity osteotomy is performed as previously described (Lafaver et al. 2007). A standard TTA plate is used and the plate can be
adjusted by lateral bending of the plate proximal to the screw fixation. A recession in the
medial cortex of the tibia to accept the plate, and
a second recession in the proximal tibia for the
caudal cage screw, are made. A high-speed drill
can be used to make these adjustments. To aid in
the lateralized position of the TTA plate, a positional Kirschner wire can be placed from the tibial tuberosity to the principal tibial fragment. In
patients with patella alta, the TTA plate can be
moved distally as well as laterally. One report
described the use of TTA to manage patella alta
in nine dogs (Pugliese et al. 2015). The patella
to patellar ligament ratio will need to be calculated from a mediolateral projection and taken
into account. A mean distal translation of 14 mm
was required for the nine dogs described in this
case series.
The outcome of surgery for the management
of CR and PL is good or excellent for the
majority of patients. Complications include
those described for each individual procedure,
with potentially an increase in the likelihood of
failure of fixation and a loss for patellar reduction. In one report, the risk of loss of patellar
reduction after tibial tuberosity transposition
was increased in dogs with concurrent CR
(Stanke et al. 2014).
References
Aiken M, Barnes D. Are the fabellae bisected by
the femoral cortices in a true craniocaudal pelvic
limb radiograph? J Small Anim Pract 2014;55:465–
470.
Arthurs GI, Langley-Hobbs SJ. Complications associated with corrective surgery for patellar luxation in
109 dogs. Vet Surg 2006;35:559–566.
Arthurs GI, Langley-Hobbs SJ. Patellar luxation as
a complication of surgical intervention for the
management of cranial cruciate ligament rupture in
dogs. A retrospective study of 32 cases. Vet Comp
Orthop Traumatol 2007;20:204–210.
Barnes DM, Anderson AA, Frost C, et al. Repeatability and reproducibility of measurements of femoral
and tibial alignment using computed tomography
multiplanar reconstructions. Vet Surg 2015;44:85–
93.
Dismukes DI, Tomlinson JL, Fox DB, et al. Radiographic measurement of the proximal and distal
mechanical joint angles in the canine tibia. Vet Surg
2007;36:699–704.
Dismukes DI, Fox DB, Tomlinson JL, et al. Determination of pelvic limb alignment in the large-breed
dog: a cadaveric radiographic study in the frontal
plane. Vet Surg 2008a;37:674–682.
Dismukes DI, Tomlinson JL, Fox DB, et al. Radiographic measurement of canine tibial angles in the
sagittal plane. Vet Surg 2008b;37:300–305.
Dudley RM, Kowaleski MP, Drost WT, et al. Radiographic and computed tomographic determination
of femoral varus and torsion in the dog. Vet Radiol
Ultrasound 2006;47:546–552.
Fitzpatrick N, Johnson J, Hayashi K, et al. Tibial
plateau leveling and medial opening crescentic
osteotomy for treatment of cranial cruciate ligament rupture in dogs with tibia vara. Vet Surg
2010;39:444–453.
Fitzpatrick N, Solano MA. Predictive variables for
complications after TPLO with stifle inspection
by arthrotomy in 1000 consecutive dogs. Vet Surg
2010;39:460–474.
Gibbons SE, Macias C, Tonzing MA, et al. Patellar luxation in 70 large breed dogs. J Small Anim Pract
2006;47:3–9.
Harrysson OLA, Cormier DR, Marcellin-Little DJ,
et al. Rapid prototyping for treatment of canine
limb deformities. Rapid Prototyping J 2003;9:37–42.
Jackson GM, Wendelburg KL. Evaluation of the effect
of distal femoral elevation on radiographic measurement of the anatomic lateral distal femoral
angle. Vet Surg 2012;41:994–1001.
Jaeger GH, Marcellin-Little DJ, Ferretti A. Morphology and correction of distal tibial valgus deformities. J Small Anim Pract 2007;48:678–682.
Johnson AL, Probst CW, Decamp CE, et al. Comparison of trochlear block recession and trochlear
wedge recession for canine patellar luxation using
a cadaver model. Vet Surg 2001;30:140–150.
Johnson AL, Broaddus KD, Hauptman JG, et al. Vertical patellar position in large-breed dogs with clinically normal stifles and large-breed dogs with
medial patellar luxation. Vet Surg 2006;35:78–81.
Kaiser S, Cornely D, Golder W, et al. The correlation of
canine patellar luxation and the anteversion angle
as measured using magnetic resonance images. Vet
Radiol Ultrasound 2001;42:113–118.
Kalff S, Butterworth SJ, Miller A, et al. Lateral patellar
luxation in dogs: a retrospective study of 65 dogs.
Vet Comp Orthop Traumatol 2014;27:130–134.
VetBooks.ir
Surgical Management of Cruciate Ligament Rupture Combined with Patella Luxation
Lafaver S, Miller NA, Stubbs WP, et al. Tibial tuberosity advancement for stabilization of the canine cranial cruciate ligament-deficient stifle joint: surgical
technique, early results, and complications in 101
dogs. Vet Surg 2007;36:573–586.
Langenbach A, Marcellin-Little DJ. Management
of concurrent patellar luxation and cranial cruciate ligament rupture using modified tibial
plateau levelling. J Small Anim Pract 2010;51:97–
103.
Leonard KC, Kowaleski MP, Saunders WB, et al.
Combined tibial plateau levelling osteotomy and
tibial tuberosity transposition for treatment of cranial cruciate ligament insufficiency with concomitant medial patellar luxation. Vet Comp Orthop
Traumatol 2016;29:546-540.
Mossman H, von Pfeil DJ, Nicholson M, et al. Accuracy of three pre- and intra-operative measurement
techniques for osteotomy positioning in the tibial plateau levelling procedure. Vet Comp Orthop
Traumatol 2015;28:250–255.
Newman M, Bertollo N, Walsh W, et al. Tibial tuberosity transposition-advancement for lateralization of
the tibial tuberosity: an ex vivo canine study. Vet
Comp Orthop Traumatol 2014;27:271–276.
Palmer RH, Ikuta CL, Cadmus JM. Comparison
of femoral angulation measurement between
radiographs and anatomic specimens across a
broad range of varus conformations. Vet Surg
2011;40:1023–1028.
Pugliese LC, Pike FS, Aiken SW. Distal tibial tuberosity translation using TTA implants for the treatment of patella alta in large breed dogs. Surgical
technique and clinical outcome. Vet Comp Orthop
Traumatol 2015;28:274–281.
Putnam RW. Patellar luxation in the dog. University
of Guelph, 1968.
269
Read RA, Robins GM. Deformity of the proximal tibia
in dogs. Vet Rec 1982;111:295–298.
Roush JK. Canine patellar luxation. Vet Clin North
Am Small Anim Pract 1993;23:855–868.
Slocum B, Slocum TD. Tibial plateau leveling
osteotomy for repair of cranial cruciate ligament
rupture in the canine. Vet Clin North Am Small
Anim Pract 1993;23:777–795.
Stanke NJ, Stephenson N, Hayashi K. Retrospective risk factor assessment for complication following tibial tuberosity transposition in 137 canine
stifles with medial patellar luxation. Can Vet J
2014;55:349–356.
Swiderski JK, Palmer RH. Long-term outcome of
distal femoral osteotomy for treatment of combined distal femoral varus and medial patellar luxation: 12 cases (1999–2004). J Am Vet Med Assoc
2007;231:1070–1075.
Tomlinson J, Fox D, Cook JL, et al. Measurement
of femoral angles in four dog breeds. Vet Surg
2007;36:593–598.
Willauer CC, Vasseur PB. Clinical results of surgical
correction of medial luxation of the patella in dogs.
Vet Surg 1987;16:31–36.
Wright JR. Combined patellar luxation-cruciate
repair. J Am Anim Hosp Assoc 1979;15:85–91.
Yasukawa S, Edamura K, Tanegashima K, et al. Evaluation of bone deformities of the femur, tibia, and
patella in Toy Poodles with medial patellar luxation
using computed tomography. Vet Comp Orthop
Traumatol 2016;29:29–38.
Yeadon R, Fitzpatrick N, Kowaleski MP. Tibial
tuberosity transposition-advancement for treatment of medial patellar luxation and concomitant
cranial cruciate ligament disease in the dog. Surgical technique, radiographic and clinical outcomes.
Vet Comp Orthop Traumatol 2011;24:18–26.
VetBooks.ir
VetBooks.ir
32
Biomechanics of the Cranial
Cruciate Ligament-Deficient
Stifle Treated by Tibial
Osteotomies
Antonio Pozzi, Stanley E. Kim, and Selena Tinga
Introduction
Normal tibiofemoral motion is constrained by
articular surfaces, ligaments, joint capsule and
menisci. Cruciate ligament rupture (CR), particularly rupture of the cranial cruciate ligament (CrCL), alters these constraints and causes
abnormal motion between the articular surfaces
(Anderst & Tashman 2009). Modification in cartilage loading caused by the altered surface
interaction initiates progressive osteoarthritis
(Tashman et al. 2004; Anderst & Tashman 2009;
Kim et al. 2009a). Thus, the goal for CrCL reconstruction should be the restoration of normal
stifle mechanics, to reestablish biomechanical
homeostasis, and to halt the progression of
osteoarthritis.
Much of the current knowledge regarding
CrCL repair biomechanics in dogs has been
derived from ex vivo studies evaluating normal, CrCL-deficient and surgically treated stifles under controlled conditions or theoretical
analysis. However, ex vivo and theoretical studies cannot replicate functional loading, and represent only the ‘time-zero’ condition, immediately after surgical fixation (Warzee et al. 2001;
Shahar & Milgram 2006; Apelt et al. 2007). More
recent investigations conducted in vivo suggest
that the results of ex vivo studies should be
interpreted with much caution as stabilization
techniques fail to provide joint stability in up to
70% of cases (Kim et al. 2012; Skinner et al. 2013;
Rey et al. 2014).
Most clinical and experimental studies evaluating surgical techniques for CR adopt static
stability as a measure of the success of the
surgical technique to reestablish normal joint
mechanics (Gambardella et al. 1981; Slocum &
Slocum 1993; Warzee et al. 2001). For example,
a persistent positive cranial drawer test after an
extracapsular technique has been traditionally
considered a sign of stifle instability and an
indication of failure of the procedure. A neutralized cranial tibial thrust after tibial plateau
leveling osteotomy (TPLO) has generally been
used as an indication of a ‘stable’ stifle after
reduction of the tibial plateau slope. However,
in both cases, static stability (palpable stability
on orthopaedic examination) may not necessarily correlate with dynamic stability (controlled
alignment of the stifle during activity in vivo).
A key concept is that stifle stability is a
dynamic phenomenon, describing the response
of the neuromusculoskeletal system to a complex combination of body position, muscle
forces, external loads and sensory inputs.
The limited value of palpation tests, such as
cranial drawer and tibial compression tests, for
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
271
VetBooks.ir
272
Surgical Treatment
predicting clinical function is likely a reflection
of the discrepancy between measures of joint
laxity versus measures of dynamic stability.
Laxity tests measure the maximum displacement of the joint in response to an applied
external load, in the absence of muscle forces.
Simple laxity elicited by palpation cannot
simulate the complexity, directions and rate of
application of muscular forces produced at the
stifle during movement. Even the tibial compression test, which attempts to simulate
weight-bearing, fails to replicate significant
loads transmitted across the stifle, such as a
quadriceps force. For this reason, it would be
more correct to use the term ‘laxity’ when static
stability is evaluated, and consider dynamic
stability only if stifle kinematics can be evaluated in the whole range of motion during
different gait patterns in vivo.
Single-plane fluoroscopy is frequently used
for the accurate non-invasive kinematic evaluation of human knees, and the technique has
been validated for dog stifles (Jones et al. 2014).
While biplanar fluoroscopy is considered the
most accurate modality for determining joint
kinematics, the lateral single plane modality
was accurate to within 1.28 mm for translations
and 1.58◦ for rotations (Jones et al. 2014). This
technique allows for evaluation during locomotion in vivo in clinical cases, and has since been
used to determine normal dog stifle kinematics during treadmill walking and trotting, stair
climbing, and sitting (Kim et al. 2015).
Biomechanics of tibial osteotomies
In 1983 Slocum described the cranial tibial
thrust as a tibiofemoral shear force occurring
during weight-bearing (Slocum & Devine 1983).
Slocum also presented a theoretical model
which proposed that the magnitude of cranial
tibial thrust was dependent on the degree of
the caudal slope of the tibial plateau (Slocum
& Slocum 1993). The compressive forces of
weight-bearing, assumed to be parallel to the
axis of the tibia, can be resolved into a cranially directed component responsible for cranial tibial translation, and a joint-compressive
force (Figure 32.1). In the normal stifle the cranial shear component is opposed by the CrCL
and by muscle forces. In the CrCL-deficient
stifle, the uncontrolled cranial shear force
results in cranial tibial subluxation.
Based on his model, Slocum proposed that
the tibial plateau angle (TPA) was a major
factor in stifle biomechanics influencing the
magnitude of cranial shear force. In an attempt
to dynamically decrease the uncontrolled
shear force in the CrCL-deficient stifle, Slocum
described in 1984 the closing cranial wedge
ostectomy (CCWO) for the treatment of CR
in dogs (Slocum & Devine 1984). This technique was intended to eliminate cranial tibial
thrust during the weight-bearing phase of the
stride by reducing the TPA. Its mechanism has
been recently investigated in an ex vivo study
evaluating the size of the wedge ostectomy
necessary to neutralize the tibial thrust (Apelt
et al. 2010). An ostectomy with a wedge angle
equal to TPA +5◦ resulted in a stable stifle at
a TPA of approximately 6◦ . Other factors that
influence the postoperative TPA after CCWO
include the position of the ostectomy and the
cortical alignment after reduction (Bailey et al.
2007). These variables may be responsible for
the discrepancies in TPA reported after CCWO
(Macias et al. 2002).
A large CCWO can shorten the tibia cranially
and alter the femoro-patellar joint, lowering the
patella relative to the femur and leading to
hyperextension of the stifle joint (Corr & Brown
2007). Kinematic gait analysis after the CCWO
procedure has shown an increase in extension
during the swing phase of the stifle and talocrural joints, and an increase in limb extension at
paw contact, but no changes occurred in the stifle and talocrural joint angles at the stance phase
(Lee et al. 2007).
The goal of TPLO is also to neutralize cranial tibial thrust and prevent tibial subluxation
(Slocum & Slocum 1993). Biomechanical studies
have demonstrated that after tibial plateau rotation, the tibiofemoral shear force shifts from cranial to caudal when the limb is loaded (Warzee
et al. 2001; Reif et al. 2002). Thus, it has been
postulated that joint stability is dependent on
the caudal cruciate ligament (CaCL) neutralizing caudal tibial translation after TPLO (Warzee
et al. 2001; Reif et al. 2002). TPLO has a significant effect on CrCL strain, which decreases as
the tibial plateau is rotated (Haynes et al. 2015).
This protective effect of TPLO on CrCL strain
is the basis for recommending TPLO in dogs
273
VetBooks.ir
Biomechanics of the Cranial Cruciate Ligament-Deficient Stifle Treated by Tibial Osteotomies
(A)
(B)
Figure 32.1 Slocum theorized that, during weight-bearing, the joint reaction force (magenta arrow) is approximately
parallel the longitudinal axis of the tibia. In the cranial cruciate ligament-deficient stifle (A), the joint reaction force can
be resolved into a cranially directed tibiofemoral shear component (parallel to tibial plateau) and a joint-compressive
force (perpendicular to tibial plateau). By leveling the tibial plateau (B), the joint reaction force is perpendicular to the
tibial plateau, and thus can only be resolved into a joint-compressive force; cranial tibial thrust is eliminated. Source:
Kim et al. 2008. Reproduced with permission from John Wiley & Sons, Inc.
presenting with early partial CR (Hulse et al.
2010).
The integrity of the CaCL must be assessed
at the time of arthrotomy or arthroscopy before
performing TPLO. In the authors’ experience,
CaCL abnormalities of varying severity can
occur concurrently with CR (see also Chapter 17). The underlying cause of CaCL degeneration and rupture is also unknown, but it may
be secondary to osteoarthritic change, or due to
the same pathologic processes that causes CrCL
fiber damage and rupture. TPLO increases
loads on the CaCL during weight-bearing
(Warzee et al. 2001), which may accelerate
any pre-existing CaCL degeneration postoperatively. While rare, complete rupture of the CaCL
has been documented (Slocum & Slocum 1993).
This complication will result in severe stifle
instability. Hence, CaCL abnormalities may preclude the use of TPLO in CrCL-deficient stifles.
Another biomechanical theory argues that
the tibia is not axially loaded as proposed by
Slocum. Rather, Tepic suggests that the total
femorotibial joint forces in vivo are directed parallel to the patellar tendon (Tepic et al. 2002).
Cranial tibial thrust, according to this model,
is then dependent on the angle between the
tibial plateau and the patellar tendon (Figure 32.2). This model also predicts that cranial tibial translation should not occur when a
CrCL-deficient stifle is flexed beyond 90◦ . The
role of the flexion angle in stifle biomechanics
has been investigated in ex vivo studies. As the
joint approaches 90◦ of flexion, the quadriceps
mechanism becomes a stabilizer and effectively
unloads the CrCL by pulling the tibia caudally
(Pozzi et al. 2008; Kim et al. 2009b). Likewise, tibial tuberosity advancement aims to impart functional stability by moving the patellar tendon
angle to approximately 90◦ when the stifle is
Surgical Treatment
VetBooks.ir
274
(A)
(B)
Figure 32.2 An alternate theory, proposed by Tepic, suggests that the joint reaction force (magenta arrow) is
approximately parallel to the patella tendon, not the tibial long axis. In the cranial cruciate ligament-deficient stifle (A),
the joint reaction force can be resolved into a cranially directed tibiofemoral shear component and a joint-compressive
force (yellow arrows). By advancing the tibial tuberosity cranially, the patella tendon is perpendicular to the tibial plateau
during stance phase of gait (B). The joint reaction force, therefore, becomes perpendicular to the tibial plateau during
weight-bearing, thus can only be resolved into a joint-compressive force; cranial tibial thrust is eliminated. Source: Kim
et al. 2008. Reproduced with permission from John Wiley & Sons, Inc.
positioned at a standing angle (Montavon et al.
2002). Ex vivo studies demonstrated that stifle
stability after CrCL transection is attained by
TTA when the patellar tendon angle is 90 ± 9◦
(Apelt et al. 2007).
The proposed theoretical mechanism of
action of the TTA may also explain the mechanism of action for TPLO (Tepic et al. 2002;
Drygas et al. 2010; Sathya et al. 2014). The Tepic
model takes into consideration both extensor
mechanism anatomy and the geometry of the
articulating surfaces of the stifle, and differs
from Slocum’s theory in that the direction of
the joint reaction force is dependent on the
inclination of the patellar tendon. By changing
the orientation of the tibial plateau relative to
the patellar tendon, TPLO may achieve a patellar tendon angle of about 90◦ in a different way
from the TTA (Drygas et al. 2010). These results
were confirmed in a clinical study reporting
the preoperative and postoperative TPA and
patellar tendon angles after TPLO (Sathya et al.
2014).
Given that craniocaudal stability is directly
related to the patellar tendon angle and, therefore, the flexion angle of the stifle, it is possible that the degree of cranial tibial subluxation
may vary between different activities, or even
different breeds. When the stifle is loaded in
deep (90◦ or greater) flexion, cranial tibial subluxation does not occur, as the patellar tendon
angle also reaches 90◦ (Kim et al. 2009b). Hence,
it could be argued that tibial osteotomies may
not benefit dogs with crouched postures, or during activities such as stair-climbing. A recent
ex vivo study demonstrated that TPLO did not
improve joint mechanics when CrCL-deficient
stifles were loaded in deep flexion (Kim et al.
VetBooks.ir
Biomechanics of the Cranial Cruciate Ligament-Deficient Stifle Treated by Tibial Osteotomies
2010). Differing stifle joint excursions over a gait
cycle may also mean that the amount of tibial plateau rotation (TPLO) or advancement of
the patellar tendon insertion (TTA) necessary to
neutralize subluxation varies between individual dogs. Firm evidence to support specific ‘tailoring’ of postoperative TPAs or patellar tendon
angles is lacking. It is unlikely that the reported
optimal angles (e.g., TPA of 6◦ ) are universal for
every dog with CR.
Traditional surgical techniques that involve
the placement of a passive stabilizing structure, such as lateral suture stabilization, have
the advantage of decreasing rotational instability, but they hinder full stifle flexion and
restrict normal axial rotational motion of the stifle, as placement of the implant cannot be not
perfectly isometric in all three planes. Flexion–
extension range of motion in stifles treated
with TPLO and TTA should not be as diminished when compared to the traditional procedures (Chailleux et al. 2007). Full flexion may be
slightly decreased after TPLO and CCWO when
compared to normal, as they move the distal
tibial segment (i.e., the longitudinal axis of the
tibia) into slight extension.
The biomechanical models on which TPLO
and TTA are based upon are two-dimensional.
Therefore, tibial osteotomies do not directly
attempt to address axial rotational instability
caused by CR (Kim et al. 2008). Axial rotation
of the tibia relative to the femur remains unrestricted, and the control of internal–external
rotational motion must then rely on muscular
forces about the stifle and joint adaptation. It
Figure 32.3 Representative image from
shape-matching software of a stifle after tibial
plateau leveling osteotomy. Three-dimensional
computed tomography-derived bone models are
superimposed over lateral projection
fluoroscopic images that are acquired during
activity, and the relative positions of the bones
are calculated using custom-written software.
275
is uncertain whether this muscular compensation occurs in dogs, or whether abnormal axial
rotation is a clinically significant factor in stifles
treated by tibial osteotomies. Persistent axial
rotational instability may be one explanation for
the progression of osteoarthritis and the subsequent meniscal tears in stifles treated by tibial osteotomies (Lazar et al. 2005; Lafaver et al.
2007). When treating clinical cases with severe
internal rotation, consideration should be given
to combining extracapsular stabilization with
osteotomies. On the other hand, extracapsular
techniques create constant external rotation and
abduction of the stifle over a range of motion,
which may also be detrimental to joint homeostasis (Chailleux et al. 2007).
The primary kinematic abnormality of CR is
an increase in cranial tibial translation. Tibial
osteotomies have been showed to successfully
neutralize cranial tibial thrust and reestablish
normal alignment of the stifle in ex vivo models.
However, in vivo studies have shown that TPLO
may not consistently provide stability in all
dogs (Kim et al. 2012). A currently unpublished
in vivo investigation of clinical dogs, using
lateral fluoroscopy (Figure 32.3), has shown
that TPLO resolves cranial tibial translation and
internal tibial rotation in the majority of dogs,
but creates a static caudal tibial displacement
that is present throughout the gait cycle (Figure 32.4) (Tinga et al. 2015). When cranial tibial
subluxation is resolved, internal tibial rotation
is resolved, but when cranial tibial subluxation
is not resolved, neither is internal tibial rotation. Presumptively, the resolution of instability
276
Surgical Treatment
VetBooks.ir
15
Cranial Tibial Translation
Millimeters
10
5
0
(A)
–5
Swing
Stance
Control
Post-Op TPLO - Persistent Subluxation
CrCL-Deficient
Post-Op TPLO - Caudal Tibial Displacement
10
Internal Tibial Rotation
Degrees
5
0
–5
–10
(B)
–15
Stance
Swing
relieves pain, although concern exists that
abnormal force transmission due to this caudal
tibial displacement likely continues to promote osteoarthritis development. Additional
studies, particularly in vivo investigations,
are required to further elucidate the mechanism by which tibial osteotomies improve
clinical lameness in dogs.
References
Anderst WJ, Tashman S. The association between
velocity of the center of closest proximity on
subchondral bones and osteoarthritis progression.
J Orthop Res 2009;7:71–77.
Apelt D, Kowaleski MP, Boudrieau RJ. Effect of tibial tuberosity advancement on cranial tibial subluxation in canine cranial cruciate-deficient stifle
joints: an in vitro experimental study. Vet Surg
2007;36:170–177.
Apelt D, Pozzi A, Marcellin-Little DJ, et al. Effect of
cranial tibial closing wedge on tibial subluxation:
an ex vivo study. Vet Surg 2010;39;454–459.
Figure 32.4 Craniocaudal tibial translation (A)
and axial rotation (B) during a representative
treadmill gait cycle from two dogs of equivalent
size and conformation, treated by tibial plateau
leveling osteotomy (TPLO). The x-axis represents
progression through the gait cycle from the
beginning of stance phase through to the end of
swing phase. Higher values represent increased
cranial tibial subluxation (A) and higher internal
tibial rotation (B). The averaged curves for both
dogs of the cranial cruciate ligament-deficient
stifle before surgery (red) and the contralateral
normal stifle (black) demonstrate marked cranial
tibial subluxation and internal rotation of the
affected stifle. At 6 months after TPLO, one dog
developed mild caudal subluxation (blue) and
mild external tibial rotation. The other dog
(yellow) had mild persistent cranial tibial
subluxation during stance phase, which
coincided with excessive internal tibial rotation.
Bailey CJ, Smith BA, Black AP. Geometric implications of the tibial wedge osteotomy for the treatment of cranial cruciate ligament disease in dogs.
Vet Comp Orthop Traumatol 2007;20:169–174.
Chailleux N, Lussier B, De Guise J, et al. In vitro 3dimensional kinematic evaluation of 2 corrective
operations for cranial cruciate ligament-deficient
stifle. Can J Vet Res 2007;71:175–180.
Corr SA, Brown C. A comparison of outcomes following tibial plateau levelling osteotomy and cranial tibial wedge osteotomy procedures. Vet Comp
Orthop Traumatol 2007;20:312–319.
Drygas KA, Pozzi A, Goring RL, et al. Effect of tibial plateau leveling osteotomy on patellar tendon
angle: a radiographic cadaveric study. Vet Surg
2010;39:428–424.
Gambardella PC, Wallace LJ, Cassidy F. Lateral
suture technique for management of anterior cruciate ligament rupture in dogs: a retrospective study.
J Am Anim Hosp Assoc 1981;17:33–38.
Haynes KH, Biskup J, Freeman A, et al. Effect of tibial
plateau angle on cranial cruciate ligament strain: an
ex vivo study in the dog. Vet Surg 2015;44:46–49.
Hulse D, Beale B, Kerwin S. Second look arthroscopic
findings after tibial plateau leveling osteotomy. Vet
Surg 2010;39:350–354.
VetBooks.ir
Biomechanics of the Cranial Cruciate Ligament-Deficient Stifle Treated by Tibial Osteotomies
Jones SC, Kim SE, Banks SA, et al. Accuracy of
noninvasive, single-plane fluoroscopic analysis for
measurement of three-dimensional femorotibial
joint poses in dogs. Am J Vet Res 2014;75:477–
485.
Kim SE, Pozzi A, Kowaleski MP, et al. Tibial
osteotomies for cranial cruciate ligament insufficiency in dogs. Vet Surg 2008;37:111–125.
Kim SE, Pozzi A, Banks SA, et al. Effect of tibial
plateau leveling osteotomy on femorotibial contact mechanics and stifle kinematics. Vet Surg
2009a;38:33–39.
Kim SE, Pozzi A, Banks SA, et al. Effect of tibial tuberosity advancement on femorotibial contact mechanics and stifle kinematics. Vet Surg
2009b;38:23–32.
Kim SE, Pozzi A, Banks SA, et al. Effect of cranial
cruciate ligament deficiency, tibia plateau leveling
osteotomy, and tibial tuberosity advancement on
contact mechanics and alignment of the stifle in
flexion. Vet Surg 2010;39:363–370.
Kim SE, Lewis DD, Pozzi A. Effect of tibial plateau
leveling osteotomy on femorotibial subluxation: in vivo analysis during standing. Vet Surg
2012;41:465–470.
Kim SE, Jones SC, Lewis DD, et al. In vivo threedimensional knee kinematics during daily activities in dogs. J Orthop Res 2015;33:1603–1610.
Lafaver S, Miller NA, Stubbs WP, et al. Tibial tuberosity advancement for stabilization of the canine cranial cruciate ligament-deficient stifle joint: surgical
technique, early results, and complications in 101
dogs. Vet Surg 2007;36:573–586.
Lazar TP, Berry CR, de Haan JJ, et al. Long-term
radiographic comparison of tibial plateau leveling osteotomy versus extracapsular stabilization
for cranial cruciate ligament rupture in the dog. Vet
Surg 2005;34:133–141.
Lee JY, Kim G, Kim JH, et al. Kinematic gait analysis of the hind limb after tibial plateau levelling
osteotomy and cranial tibial wedge osteotomy in
ten dogs. J Vet Med A Physiol Pathol Clin Med
2007;54:579–584.
Macias C, McKee WM, May C. Caudal proximal tibial
deformity and cranial cruciate ligament rupture in
small-breed dogs. J Small Anim Pract 2002;43:433–
438.
Montavon PM, Damur DM, Tepic S. Advancement
of the tibial tuberosity for the treatment of cranial
cruciate deficient canine stifle. 1st World Orthopedic Veterinary Congress; 2002; Munich, Germany,
p. 152.
277
Pozzi A, Kim SE, Banks SA, et al. Ex vivo pathomechanics of the Pond-Nuki model. Proceedings of
the Veterinary Orthopedic Society Scientific Meeting, Big Sky, MT, 2008.
Reif U, Hulse DA, Hauptman JG. Effect of tibial
plateau leveling on stability of the canine cranial
cruciate-deficient stifle joint: an in vitro study. Vet
Surg 2002;31:147–154.
Rey J, Fischer MS, Böttcher P. Sagittal joint instability
in the cranial cruciate ligament insufficient canine
stifle. Caudal slippage of the femur and not cranial
tibial subluxation. Tierarztl Prax Ausg K Kleintiere
Heimtiere 2014;42:151–156.
Sathya S, Gilbert P, Sharma A, et al. Effect of tibial plateau levelling osteotomy on patellar tendon angle: a prospective clinical study. Vet Comp
Orthop Traumatol. 2014;27:346–350.
Shahar R, Milgram J. Biomechanics of tibial plateau
leveling of the canine cruciate-deficient stifle joint:
a theoretical model. Vet Surg 2006;35:144–149.
Skinner O, Kim SE, Lewis DD, et al. In vivo femorotibial subluxation during weight-bearing after tibial
tuberosity advancement. Vet J 2013;196:86–91.
Slocum B, Devine T. Cranial tibial thrust: a primary
force in the canine stifle. J Am Vet Med Assoc
1983;183:456–459.
Slocum B, Devine T. Cranial tibial wedge osteotomy:
a technique for eliminating cranial tibial thrust in
cranial cruciate ligament repair. J Am Vet Med
Assoc 1984;184:564–569.
Slocum B, Slocum TD. Tibial plateau leveling
osteotomy for repair of cranial cruciate ligament
rupture in the canine. Vet Clin North Am Small
Anim Pract 1993;23:777–795.
Tashman S, Anderst W, Kolowich P, et al. Kinematics
of the ACL-deficient canine knee during gait: serial
changes over two years. J Orthop Res 2004;22:931–
941.
Tepic S, Damur DM, Montavon PM. Biomechanics
of the stifle joint. Proceedings, 1st World Orthopedic Veterinary Congress, Munich, Germany, 2002,
pp. 189–190.
Tinga S, Kim SE, Banks SA, et al. In vivo 3-dimensional
kinematics of cranial cruciate ligament-deficient
stifles treated with tibial plateau leveling
osteotomy. Veterinary Orthopedic Society, Sun
Valley, ID, 4 March, 2015.
Warzee CC, Dejardin LM, Arnoczky SP, et al. Effect
of tibial plateau leveling on cranial and caudal
tibial thrusts in canine cranial cruciate-deficient
stifles: an in vitro experimental study. Vet Surg
2001;30:278–286.
VetBooks.ir
VetBooks.ir
33
Arthroscopic Follow-Up
after Surgical Stabilization
of the Stifle
Brian S. Beale and Donald A. Hulse
Introduction
Cruciate ligament rupture (CR) is a common
cause of pelvic limb lameness in dogs (Aragon
& Budsberg 2005). The majority of veterinary
surgeons agree that return to optimal function is
best accomplished through surgical treatment.
A variety of surgical techniques have been
described to stabilize the cruciate-deficient stifle, including extracapsular stabilization, intraarticular cranial cruciate ligament (CrCL) reconstruction, and techniques designed to reduce
the force causing cranial tibial translation
(cranial tibial thrust) during weight-bearing
(Warzee et al. 2001; Reif et al. 2002; Jerram &
Walker 2003). Extracapsular stabilization and
tibial plateau leveling osteotomy (TPLO) are
the most common techniques used by veterinary surgeons to treat CR. Although deemed
clinically successful in most cases, complications associated with these techniques have
been described (Pacchiana et al. 2003; Priddy
et al. 2003; Stauffer et al. 2006). Follow-up arthroscopic evaluation of the stifle after surgical stabilization has provided important evidence to
assess outcome after surgical treatment (Whitney 2003; Rayward et al. 2004; Hulse et al. 2010).
Surgical recommendations should ideally be
made by applying the principles of evidence-
based medicine (Aragon & Budsberg 2005).
Follow-up arthroscopic evaluation of intraarticular structures is performed as an outcome measurement in experimental studies or
in client-owned dogs with clinical signs after a
previous surgical procedure. Follow-up arthroscopic evaluation is also occasionally used to
assess outcome in patients without clinical
signs. Advocates of follow-up arthroscopy in
this group of patients cite the low morbidity
associated with the technique, the frequent discovery of unknown pathology, and the ability to better understand the patient’s true outcome after surgery as justification. Follow-up
arthroscopy is typically only performed if the
patient is having clinical problems or is undergoing general anesthesia for another reason,
usually another surgical procedure. A common
example would be follow-up arthroscopy performed on a stifle after previous CR stabilization at the time of treatment of the contralateral stifle for CR. Evidence of changes
seen within the joint can influence treatment
and activity recommendations for the patient.
In addition, simultaneous implant removal
can be performed, eliminating the potential
necessity for implant removal in the future.
Follow-up arthroscopy of the stifle has been
used most commonly to assess TPLO patients,
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
279
Surgical Treatment
VetBooks.ir
280
CaCL
CaCL
CaCL
CrCL
***
(A)
CrCL
CrCL
(B)
(C)
Figure 33.1 (A) The insertion of the craniomedial band is torn (∗∗∗ ) in this dog with a partial tear of the cranial cruciate
ligament (CrCL). This patient has a normal amount of cranial tibial translation. The caudal cruciate ligament (CaCL) is
also visible. (B) The torn fibers of the ligament have been carefully debrided before performing a tibial plateau leveling
osteotomy. The intact fibers of the CrCL were probed and found to have normal integrity and were left intact. (C) The
CrCL appears healthy and functional at a follow-up arthroscopic examination of the same patient 2 years later.
but its use has also provided valuable information in patients undergoing extracapsular or
intra-articular CR stabilization and treatment of
OCD of the femoral condyle.
Follow-up arthroscopic examination
after TPLO
Follow-up arthroscopic examination of the stifle is performed using standard arthroscopic
techniques (Beale et al. 2003). Typically, the
same portals are used as the initial arthroscopy.
Exploration of the intra-articular structures is
performed, starting in the proximal aspect of
the joint with the stifle held in an extended
position. Periarticular osteophytes, cartilage
integrity and synovial membrane appearance
are evaluated. The intercondylar notch region
is evaluated with the stifle positioned in flexion. The CrCL and caudal cruciate ligament
(CaCL) are assessed for fiber damage, inflammation, remodeling, and vascular proliferation.
The menisci are carefully observed and probed
for the presence of fiber rupture or wear. A
Hohmann retractor can be inserted into the joint
just lateral to the proximal aspect of the patellar
tendon through an accessory instrument portal
to separate the joint surfaces and improve the
view and access to the menisci. Alternatively,
a stifle distractor can be used to improve
examination (see also Chapter 23). Bucket-
handle tears of the medial meniscus are the
most common type of meniscal tear seen, and
are typically treated by partial meniscectomy.
Radial tears are also common and are treated
by partial meniscectomy at the discretion of
the surgeon. Large radial tears are generally
treated, while small radial tears and small frays
are left untreated. Small frays of the axial border of the lateral meniscus are common in normal dogs without clinical signs. Small frays
may increase the susceptibility to larger radial
tears in the future in stifles experiencing instability. A medial meniscal release (MR) can
also be performed if deemed necessary by the
surgeon.
Follow-up arthroscopy was found to be
valuable in assessing patients treated with
TPLO (Hulse et al. 2010). Hulse et al. (2010)
used a second-look arthroscopic examination
to evaluate dogs with CrCL fiber rupture of
varying degrees after TPLO. Intra-articular
structures appeared normal or near-normal at
long-term follow-up after a TPLO procedure
in early partial tears of the CrCL (Hulse et al.
2010). The CrCL did not continue to rupture
after the plateau was leveled to approximately
6◦ (Figure 33.1). The blocking of CrCL fiber
tearing may be a consequence of decreased
loading of the CrCL after rotation of the tibial
plateau (Warzee et al. 2001; Reif et al. 2002;
Wolf et al. 2008; Haynes et al. 2015; Barger et al.
2016). When the tibial plateau is rotated to
approximately 6◦ relative to the weight-bearing
VetBooks.ir
Arthroscopic Follow-Up after Surgical Stabilization of the Stifle
the longest interval from initial surgery to
second-look arthroscopy in this group of dogs.
Conversely, the majority of dogs with a partial tear with an incompetent remaining CrCL
and cranial drawer or a completely ruptured
CrCL ligament had significant intra-articular
changes. Of interest were articular cartilage
lesions involving the medial or lateral femoral
condyle or tibial plateau (Figure 33.3). Lesions
included chondromalacia, fibrillation, and erosion (Figure 33.4). The lesions may arise from
abnormal joint contact mechanics or increased
contact with cranial soft tissue after rotation
of the tibial plateau to eliminate cranial tibial
thrust. Some 85% of the stifles in this group
(39/46) had visible cartilage lesions, with the
majority (28/39 stifles) having Grade 3 or Grade
4 lesions (see Beale et al. 2003 for grading system). Cartilage lesions appeared in the medial
femoral condyle (13 joints), lateral femoral
condyle (12 joints), and tibial plateau (three
joints) (Figure 33.5). Abaxial non-articular cartilage abrasion was most common, but axial
lesions of the weight-bearing surface were also
noted (Figures 33.6 and 33.7). In most dogs, mild
fraying of the CaCL was noted; in three dogs
there was complete rupture of the CaCL. In
one of these three dogs there was over-rotation
of the tibial plateau at revision surgery (initial postoperative slope 6◦ ; postoperative slope
after revision 0◦ ); in the other two dogs the tibial
plateau was rotated to 7◦ in one case and to 10◦
in the other case. The history and acute nature
of lameness in the latter two dogs was suggestive of a traumatic episode. Eight dogs developed a bucket-handle tear in the caudal horn
of the medial meniscus (postliminary meniscal
MFC
MM
CrCL
Figure 33.2 The cartilage of the medial femoral condyle
(MFC) and tibial plateau and the medial meniscus (MM)
appear healthy in dogs with early partial tears of the CrCL
at follow-up arthroscopy.
axis, cranial tibial thrust is transformed to a
caudal tibial thrust (Warzee et al. 2001; Reif et al.
2002). Eliminating cranial tibial thrust would
likely lower strain within the CrCL, reducing
the possibility of further fiber tearing. This
supports other clinical work which suggests
that TPLO has a protective effect on the CrCL
in dogs having an early partial CR (Wolf et al.
2008). As such, the authors do not recommend
the debridement of intact functional CrCL
fibers due to good functional outcome and the
potential protective effect on the menisci and
cartilage. The articular cartilage of the femur
and tibia, the medial and lateral menisci, and
synovial joint capsule all appeared normal in all
joints in this group of dogs (Figure 33.2). These
observations were true at 4 years after surgery,
Figure 33.3 (A) The cartilage of
the medial femoral condyle (MFC)
and tibial plateau (TP) and the
medial meniscus (MM) appear
normal at the time of tibial plateau
leveling osteotomy in this patient
with an unstable partial CrCL tear.
(B) The cartilage of the MFC and TP
has fibrillation at the time of
follow-up arthroscopy in this
patient 12 months later. The medial
meniscus also has small radial tears.
MFC
MFC
MM
TP
MM
TP
(A)
281
(B)
VetBooks.ir
282
Surgical Treatment
MFC
MFC
MM
TP
MM
TP
***
(A)
(B)
LFC
LFC
LM
LM
TP
***
(C)
TP
(D)
***
femur
lateral central abrasion
Figure 33.5 Abrasion of the cartilage (∗∗∗ ) of the central
weight-bearing region of the lateral femoral condyle can
be seen in this tibial plateau leveling osteotomy patient
28 months after surgery.
MFC
MFC
JC
(A)
***
***
abaxial medial condyle
abrasion
cranial capsule
(B)
Figure 33.4 (A) The cartilage of the
medial femoral condyle (MFC) and
tibial plateau (TP) appears healthy in
this patient with a complete CrCL tear.
Small radial tears of the medial
meniscus (MM) are present in this
patient treated with a tibial plateau
leveling osteotomy. (B) The majority of
the cartilage of the medial
compartment continues to appear
healthy in this patient 18 months later.
A focal area of fibrillation is seen at the
cranial aspect of the tibial plateau (∗∗∗ ).
Small radial tears of the medial
meniscus have progressed slightly. (C)
The cartilage of the lateral femoral
condyle (LFC) and tibial plateau (TP)
appears healthy in this patient with a
complete CrCL tear. Lateral meniscus
(LM). (D) The majority of the cartilage
of the lateral compartment continues to
appear healthy in this patient at
follow-up arthroscopy. A focal area of
fibrillation is seen at the caudal aspect
of the tibial plateau (∗∗∗ ).
tear). Commonly, the only clinical finding was
the onset of decreased limb function. Without
specific intra-articular inspection, clinical findings in these cases may be mistakenly diagnosed with overuse injury or progression of
osteoarthritis.
Arthur et al. (2005) evaluated the synovium,
CrCL, CaCL, medial meniscus, lateral meniscus, femoral trochlea, femoral condyles and
tibial plateau using follow-up arthroscopy in
40 dogs (45 stifles) previously treated with
TPLO. Pathologic changes were identified at
the time of initial surgery and followed over
time. Radiographic evidence of periarticular
osteophytes was unchanged or only minimally
increased at the time of follow-up in 36 stifles, and markedly increased in nine stifles.
Figure 33.6 (A,B) Abrasion of the
cartilage (∗∗∗ ) of the abaxial non
weight-bearing region of the medial
femoral condyle (MFC) adjacent to the
cranial joint capsule (JC) can be seen in
these tibial plateau leveling osteotomy
patients at long-term follow-up
arthroscopy. The joint capsule is
thickened and has increased stiffness in
both patients.
VetBooks.ir
Arthroscopic Follow-Up after Surgical Stabilization of the Stifle
similar meniscal tears left untreated. The treatment of small radial tears of the lateral meniscus with radiofrequency partial meniscectomy
was associated with a greater frequency of progressive cartilage wear compared to no treatment of the meniscus. Cartilage wear was evident arthroscopically in eight stifles without
radiographic evidence of increased osteoarthritis. Synovitis was unchanged in 15, increased
in two, and decreased in 18 stifles. Medial and
lateral meniscal tears were present at follow-up
in 16 and eight stifles, with increased cartilage
wear in eight stifles (Figures 33.8 and 33.9). Sites
of partial meniscectomies at initial arthroscopy
were intact and unchanged in 12 cases, while
further meniscal tearing had developed in six
cases. The CaCL was initially intact in all stifles. However, lesions such as hyperemia and
mild fraying were seen at this time in 13 stifles and progressed in nine cases (Figure 33.10).
With the exception of one case of complete
rupture, lesions at follow-up were limited
to mild increases in fraying, stretching, and
hyperemia (Figures 33.11–33.13). In 10 dogs,
gross lesions such as fraying, remodeling, or
hyperemia of the CaCL developed subsequent
to a grossly normal appearance at the time
of TPLO.
LFC
***
JC
lateral femoral condyle
grade 5 lesion
Figure 33.7 Abrasion of the cartilage (∗∗∗ ) of the abaxial
non weight-bearing region of the lateral femoral condyle
(LFC) adjacent to the cranial joint capsule (JC) can be
seen in this tibial plateau leveling osteotomy patient at
follow-up arthroscopy.
Progression of osteophytes was evident arthroscopically in 25% of stifles at follow-up. Cartilage wear was unchanged in 15 stifles and
increased in 20 stifles. Stifles with small radial
tears of the lateral meniscus treated by radiofrequency partial meniscectomy had increased cartilage wear in 67% of treated joints. Increased
cartilage wear was evident in 50% of stifles with
MFC
MFC
Figure 33.8 (A) The medial
femoral condyle (MFC), tibial
plateau (TP) and medial meniscus
(MM) appear normal at the time of
tibial plateau leveling osteotomy. (B)
The MFC and TP appear normal, but
the cranial horn of the medial
meniscus has mild radial tears at
follow-up arthroscopic examination
(∗∗∗ ).
MM
MM
TP
TP
(A)
***
(B)
medial condyle
Figure 33.9 (A) The medial
meniscus of this patient with a
complete CrCL tear has a latent
bucket-handle meniscal tear at
follow-up arthroscopy. (B) The
meniscal tear is not visible until
probed.
**********
probe medial meniscus
(A)
283
Hohmann retraction
bucket-handle tear
(B)
Surgical Treatment
VetBooks.ir
284
CaCL
CaCL
***
***
(A)
Figure 33.10 (A) The caudal
cruciate ligament (CaCL) shows mild
wear (∗∗∗ ) before tibial plateau
leveling osteotomy and mild
progression of wear at 20 months
after surgery (B).
(B)
after TPLO (Figure 33.15). Synovitis was generally decreased at follow-up examination (Figure 33.16). Cases in which gross changes in the
appearance of the CaCL were present lend credence to the potentially detrimental increases in
caudal translation after TPLO. Small radial tears
of the lateral meniscus may not require treatment, and the use of radiofrequency for partial
meniscectomy should be used judiciously.
Canine meniscal injuries are often found in
conjunction with CR or after surgical stabilization of the CrCL-deficient stifle. Meniscal tears
may be displaced and easily identified. Others
Important findings in the study included
the observation that arthroscopic evaluation
of the stifle allowed a diagnosis of joint disease not evident radiographically. The CrCL
remained intact when early partial tears were
treated with TPLO in patients having no palpable instability. Partial tears of the CrCL having instability at the time of TPLO typically
remained intact at follow-up, but the ligament remained stretched (Figure 33.14). Arthroscopic and radiographic evidence of increased
osteophyte formation indicates the potential
for progressive osteoarthritis in some cases
CaCL
(A)
CaCL
(B)
CaCL
CaCL
***
***
(A)
Figure 33.11 (A) The caudal
cruciate ligament (CaCL) appears
normal before tibial plateau leveling
osteotomy (TPLO), and normal at 22
months after TPLO (B).
(B)
Figure 33.12 (A) The caudal
cruciate ligament (CaCL) appears
inflamed with loss of detail (∗∗∗ ) at
the time of tibial plateau leveling
osteotomy. Normal longitudinal
fibers of the CaCL can be seen at the
femoral attachment of the ligament.
(B) The CaCL appears to have
progressive inflammation and loss
of fiber detail (∗∗∗ ) 11 months after
surgery. No normal-appearing CaCL
fibers are visible.
VetBooks.ir
Arthroscopic Follow-Up after Surgical Stabilization of the Stifle
CaCL
***
CrCL
Figure 33.13 The caudal cruciate ligament (CaCL) has
substantial tearing (∗∗∗ ) in this patient with an incompetent
cranial cruciate ligament (CrCL) tear treated with
a tibial plateau leveling osteotomy. This is an uncommon
finding at follow-up arthroscopic examination.
may be latent and require careful palpation
with a probe to identify. Meniscal tears that
occur subsequent to treatment of CR are termed
postlimimary tears. Follow-up arthroscopy has
CrCL
Figure 33.14 Appearance of an incompetent partial
cranial cruciate ligament (CrCL) 2 years after tibial
plateau leveling osteotomy (TPLO) surgery. Instability of
the stifle was present due to stretching of the CrCL before
TPLO. The ligament continues to have mild laxity, but
inflammation has subsided and no further damage to the
ligament is seen after TPLO. The TPLO procedure appears
to have protected the CrCL from progressive damage.
285
provided valuable information towards the
understanding of the impact of progressive
cruciate ligament fiber rupture and its treatment on the menisci over time. MR at the time
of stabilization of the CrCL-deficient stifle has
been recommended to prevent further injury
to the caudal pole of the medial meniscus after
TPLO. Conversely, MR may result in joint
instability and impairment of load transmission, which may accelerate the progression of
osteoarthritis (Pozzi et al. 2008). Meniscectomy,
which has similar mechanical results as MR on
the stifle, leads to osteoarthritis in both humans
and animals. Kim et al. (2009) suggested that
the risk of postliminary meniscal injury is
smaller after TPLO due to the neutralization of
cranial tibial thrust, and thus the need for MR
is controversial. In addition, Luther et al. (2009)
reported that MR alone in CrCL-intact stifles
was associated with articular cartilage loss
and further meniscal pathology. These studies
would tend to suggest that MR is contraindicated at the time of surgical stabilization of a
CR stifle. These findings, however, are based
on in vitro or ex vivo studies or in dogs that
had intact CrCL. Aman & Beale (2009) used
follow-up arthroscopy to assess clinical patients
with CR. This study compared CrCL-deficient
stifles of dogs having undergone TPLO with
MR to dogs having undergone TPLO with no
MR. Follow-up arthroscopy was used to assess
the stifles at long-term follow-up. The findings
of this study suggested that there may not be
a significant difference in the progression of
osteoarthritis between dogs receiving TPLO
with MR and dogs receiving TPLO without
MR. The group found a risk of postliminary
meniscal injury with or without MR, but severe
meniscal injury was much more likely without
MR. A higher incidence of bucket-handle tears
was seen in dogs not receiving a MR. Small
radial tears were the predominant type of tear
seen if MR was performed. Meniscal tears were
more common in the dogs having MR at the
meniscotibial ligament as compared to a midbody incision. MR at the meniscotibial ligament
or mid-body appeared to remain functional
in all dogs having the procedure performed.
The meniscotibial ligament did not appear to
reattach. The mid-body MR incisions appeared
to heal with great variation (Figure 33.17). Some
of the mid-body MR incisions healed with a
Surgical Treatment
VetBooks.ir
286
MFC
JC
JC
MFC
***
***
(A)
(B)
(A)
Figure 33.15 (A) Periosteal osteophytes
typically remain the same size or become
slightly larger over time after tibial
plateau leveling osteotomy (TPLO). This
patient with a complete CrCL tear had
mild osteophyte formation (∗∗∗ ) in the
medial gutter at the time of TPLO. (B) The
osteophytes increased a little in size over
34 months. Joint capsule (JC), medial
femoral condyle (MFC).
Figure 33.16 Some degree of synovitis
was typically seen at follow-up
arthroscopy in patients after tibial plateau
leveling osteotomy. These patients had
mild (A) and moderate (B) synovitis,
although both patients were subclinical.
(B)
MFC
MFC
MFC
***
MR
TP
***
TP
TP
(A)
(B)
(C)
MFC
***
MFC
TP
***
TP
(D)
(E)
Figure 33.17 (A) A mid-body medial meniscal release (MR) is performed under arthroscopic observation. Follow-up
arthroscopic evaluation revealed inconsistent findings at the MR incision site. (B,C) The site of MR healed (∗∗∗ ) with a
smooth axial border in most patients. (D) The gap at the MR incision filled with irregular fibrous tissue (∗∗∗ ) or showed no
signs of healing in other patients (∗∗∗ ) (E). Interestingly, minimal signs of cartilage wear of the medial femoral condyle
(MFC) and tibial plateau (TP) were seen. The MR appears to remain functional despite variation in healing patterns.
Evidence of continued function of the MR includes the caudal position of the medial meniscus and the dramatic
reduction in prevalence of postliminary meniscal tears.
VetBooks.ir
Arthroscopic Follow-Up after Surgical Stabilization of the Stifle
287
lateral femoral condyle
femur
lateral femoral condyle
normal lateral meniscus
(A)
lateral
meniscus
(B)
lateral meniscus
(C)
Figure 33.18 The cartilage of the femoral condyle and tibial plateau had an inconsistent appearance at the time of
follow-up arthroscopic examination after extracapsular stabilization amongst patients with cruciate ligament rupture.
The cartilage appeared to be normal (A), have mild wear (B), or have moderate wear (C).
smooth axial border, others healed with irregular fibrous tissue, and some showed no healing
response. The MR appears to remain functional
despite variation in healing patterns. Evidence
of continued function of the MR includes the
caudal position of the medial meniscus and a
dramatic reduction in the prevalence of postliminary meniscal tears. The caudal horn of the
medial meniscus appeared to sit in a more caudal position, and the meniscus did not appear to
shift forward during a tibial compression test or
cranial drawer test while viewing the meniscus
arthroscopically.
Follow-up arthroscopic examination
after extracapsular stabilization
Follow-up arthroscopy has also been used
to assess the stifle joint after extracapsular
stabilization of the CrCL-deficient stifle. Most
of the dogs examined in this group had undergone complete debridement of the CrCL at the
Figure 33.19 Some patients show
severe cartilage damage at
follow-up evaluation after
extracapsular stabilization. Erosion
of the lateral femoral condyle (∗∗∗ )
in the region opposite the lateral
tibial eminence is seen in this
patient (A). This lesion is thought to
occur due to excessive shear force.
Full-thickness erosion (∗∗∗ ) of
weight-bearing regions of the
medial femoral condyle are
occasionally seen (B).
time of stabilization. Periarticular osteophytes
typically enlarge over time. Mild to moderate
synovitis is seen. Cartilage erosion is variable
(Figure 33.18). Some dogs show progressive
cartilage erosion of the medial and lateral
compartment (Figure 33.19). Erosion primarily
involves the articular cartilage of the weightbearing regions of the medial and lateral
femoral condyle and tibial plateau. Cartilage
damage is often more severe in the lateral
compartment. Increased cartilage damage in
the lateral compartment may be secondary to
increased forces generated by the placement of
a lateral extracapsular suture. Cartilage erosion
does not appear to commonly involve non
weight-bearing regions, unlike that seen after
TPLO. Some dogs show very little evidence of
articular cartilage damage. Meniscal tears are
also common at the time of follow-up arthroscopic examination in this group of patients
(Figure 33.20). Interestingly, many dogs identified as having bucket-handle tears of the medial
meniscus were not observed to have significant
lameness by the owners. However, physical
femur
***
****
shear lesion
Grade 4 cartilage lesion
medial femoral condyle
tibial
spine
(A)
(B)
Surgical Treatment
VetBooks.ir
288
medial femoral condyle
*************
2nd tear in meniscus
torn medial meniscus
(A)
(B)
Figure 33.20 Bucket-handle tears of the medial meniscus were commonly seen at follow-up arthroscopic examination
of patients treated with extracapsular stabilization of cranial cruciate ligament tears in dogs with clinical signs, and in
dogs thought to be without clinical signs. (A) Some meniscal tears were displaced and easily identified. Other
bucket-handle tears were latent and identified only after careful probing. This patient had two bucket-handle tears of the
medial meniscus. The first tear was displaced and easily identified. Partial menisectomy was performed. The second
bucket-handle tear was latent and was identified after carefully probing the medial meniscus after removal of the first
tear (B).
examination tended to show a stiff pelvic limb
gait, a reluctance to sit square, or a slight click
when flexing the stifle. It appears that some
dogs are quite effective in minimizing the clinical signs of pain associated with a meniscal tear.
Medial patellar luxation has also been observed
at the time of follow-up arthroscopic examination after extracapsular stabilization. Arthroscopic evaluation of infected joints secondary to
an infected extracapsular suture provides valuable information regarding the intensity of the
synovitis and the degree of cartilage damage.
a high rate of failure. Follow-up arthroscopy
has found ruptured ligament fibers leading to
stretching, partial tear, or complete tear of the
prosthetic ligament. Biological replacement ligaments have also been found to experience fiber
tearing at follow-up arthroscopic examination.
Fibers of the ligament are often stretched, or the
ligament may have a partial or complete tear. A
minority of patients have a healthy-appearing
replacement ligament (Figure 33.21). Meniscal
tears are also common at the time of followup arthroscopic examination in this group
of patients. Intra-articular repairs are most
Follow-up arthroscopic examination
after intra-articular stabilization
Follow-up arthroscopy after intra-articular
stabilization has revealed similar findings
to extracapsular stabilization. Periarticular
osteophytes typically enlarge over time. Mild
to moderate synovitis is seen, and cartilage
erosion is variable. Some dogs show progressive cartilage erosion of the medial and lateral
compartment. Erosion is seen to involve the
articular cartilage of the weight-bearing regions
of the medial and lateral femoral condyle and
tibial plateau. On the other hand, some dogs
show very little change in the appearance of
the articular cartilage. Intra-articular stabilization techniques may be performed using
a prosthetic or a biological ligament replacement. Prosthetic ligament replacements have
CaCL
CrCL graft
Figure 33.21 The fascial lata graft appears healthy and
functional at follow-up arthroscopic examination in this
patient treated with intra-articular stabilization after
cruciate ligament rupture. Caudal cruciate ligament
(CaCL), cranial cruciate ligament (CrCL).
VetBooks.ir
Arthroscopic Follow-Up after Surgical Stabilization of the Stifle
commonly performed in medium- and largebreed dogs; this group of dogs typically has
persistent or intermittent lameness, and often
will have a meniscal click if a bucket-handle
tear of the medial meniscus is present.
Conclusions
Follow-up arthroscopy has provided muchneeded evidence of outcome after cruciate
stabilization surgery. Follow-up arthroscopy
was associated with minimal morbidity. Many
changes in the intra-articular environment of
the stifle have been identified, including meniscal tears, CaCL fiber wear, chronic synovitis,
cartilage wear, and osteophyte formation. Many
of the pathological changes were evident in
dogs that were thought to be without clinical
signs. Many of the arthroscopic findings are not
easily assessed by imaging techniques. Followup arthroscopy is an excellent method of assessing the intra-articular condition of the canine
stifle joint months to years after stifle surgery.
References
Aman A, Beale BS. Follow-up arthroscopic evaluation
of canine stifles having undergone tibial plateau
leveling osteotomy with and without meniscal
release. Proceedings of the 36th Annual Conference
Veterinary Orthopedic Society, 2009, p. 21.
Aragon CL, Budsberg SC. Applications of evidencebased medicine: Cranial cruciate ligament injury
repair in the dog. Vet Surg 2005;34:93–98.
Arthur EG, Beale BS, Whitney WO. Second-look
arthroscopic evaluation of the canine stifle following tibial plateau osteotomy. Proceedings of the
32nd Annual Conference Veterinary Orthopedic
Society, 2005, p. 45.
Barger B, Piazza A, Muir P. Treatment of stable partial
cruciate rupture (Grade I sprain) in five dogs with
tibial plateau levelling osteotomy. Vet Rec Case Rep
2016;4:e000315.
Beale BS Hulse DA, Schulz KS, et al. Small Animal
Arthroscopy. Philadelphia, WB Saunders, 2003.
Haynes KH, Biskup J, Freeman A, et al. Effect of tibial plateau angle on cranial cruciate ligament strain:
An ex vivo study in the dog. Vet Surg 2015;44:46–49.
289
Hulse DA, Beale BS, Kerwin S. Second look arthroscopic findings after tibial plateau leveling
osteotomy. Vet Surg 2010;39:350–354.
Jerram RM, Walker AM. Cranial cruciate ligament
injury in the dog: pathophysiology, diagnosis and
treatment. N Z Vet J 2003;51:149–158.
Kim S, Pozzi A, Banks SA, et al. Effect of tibial
plateau leveling osteotomy on femorotibial contact mechanics and stifle kinematics. Vet Surg
2009;38:23–32.
Luther JK, Cook CR, Cook JL. Meniscal release in cruciate ligament intact stifles causes lameness and
medial compartment cartilage pathology in dogs
12 weeks postoperatively. Vet Surg 2009;38:520–
529.
Pacchiana PD, Morris E, Gillings SL, et al. Surgical and
postoperative complications associated with tibial
plateau leveling osteotomy in dogs with cranial
cruciate ligament rupture: 397 cases (1998–2001).
J Am Vet Med Assoc 2003;222:184–193.
Pozzi A, Litsky AS, Field J, et al. Pressure distributions
on the medial tibial plateau after medial meniscal
surgery and tibial plateau levelling osteotomy in
dogs. Vet Comp Orthop Traumatol 2008;21:8–14.
Priddy NH, Tomlinson JL, Dodam JR, et al. Complications with and owner assessment of the outcome
of tibial plateau leveling osteotomy for treatment of
cranial cruciate ligament rupture in dogs: 193 cases
(1997–2001). J Am Vet Med Assoc 2003;222:1726–
1732.
Rayward RM, Thomson DG, Davies JV, et al. Progression of osteoarthritis following TPLO surgery:
a prospective radiographic study of 40 dogs. J Small
Anim Pract 2004;45:92–97.
Reif U, Hulse DA, Hauptman JG. Effect of leveling on
stability of the canine cranial cruciate-deficient stifle joint: an in vitro study. Vet Surg 2002;31:147–154.
Stauffer K, Tuttle T, Elkins D. Complications associated with 696 tibial plateau leveling osteotomies
(2001–2003). J Am Anim Hosp Assoc 2006;42:44–50.
Warzee CC, Dejardin LM, Arnoczky SP, et al. Effect
of tibial plateau leveling on cranial and caudal
tibial thrusts in canine cranial cruciate-deficient
stifles: an in vitro experimental study. Vet Surg
2001;30:278–286.
Whitney WO. Arthroscopically assisted surgery of
the stifle joint. In: Small Animal Arthroscopy, Beale
BS, Hulse DA, Schulz KS, Whitney WO, eds.
Philadelphia, WB Saunders, 2003.
Wolf R, Beale BS, Whitney WO. Effect of debridement
of the cranial cruciate ligament in dogs having early
partial tears of the cranial cruciate ligament at the
time of TPLO. Vet Surg 2008;37:E2.
VetBooks.ir
VetBooks.ir
34
Cranial Cruciate Ligament
Debridement
David E. Spreng
Introduction
Historically, total debridement of the torn
ends of the cranial cruciate ligament (CrCL)
was considered necessary to decrease inflammatory responses during the postoperative
period. Some investigators also advocated that
partially ruptured ligaments should be completely removed, again to decrease postoperative inflammation. Meanwhile, current information published on the function of the CrCL
has led to new developments in the approach
to ligament debridement.
The CrCL has a primarily mechanical function. It is the main restraint mechanism for cranial tibial translation throughout complete stifle
range of motion. It is also responsible for limitation of the internal rotation of the tibia (Vasseur
2002). Most surgeons consider ligaments only
to be passive stabilizers of the joint. However,
there is good evidence that the CrCL plays an
important role in proprioception and neuromuscular function, and it has been shown that
the residual portion of the CrCL maintains its
blood flow (Bray et al. 2002), providing potential
support for the healing process after joint stabilization.
Mechanoreceptors within the CrCL might be
responsible for signaling muscle stiffness of the
pelvic limb and contribute to the proprioceptive
function of the stifle (Adachi et al. 2002). Many
human patients who have had an injury of
the lower extremity describe vague symptoms
such as unsteadiness (giving-way) of the joint
(Noyes et al. 1989). It seems likely that at least
some aspects of these symptoms are related to
mechanoreceptors. However, this is difficult to
document due to the lack of sufficiently sensitive, yet measurable, parameters. A tear or
removal of the anterior cruciate ligament (ACL)
in humans has been associated with neuromuscular changes such as loss of proprioception,
alterations in muscle reflexes initiated by the
ligament, alterations in muscle stiffness, deficits
in quadriceps strength and changes in gait and
electromyographic measurements (DeFranco &
Bach 2009). It is not clear whether these changes
are caused by the loss of mechanoreceptors in
the ruptured ligament or by an altered stimulation of the remaining receptors in other articular
tissue such as the joint capsule.
Mechanoreceptors have been identified
within the canine CrCL. The receptors are
pressure-sensitive corpuscles and include
Ruffini and Pacini receptors, as well as free
nerve endings which are responsible for pain
perception and autonomic nervous system
regulation of blood flow (Cole et al. 1996).
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
291
VetBooks.ir
292
Surgical Treatment
Considering the innervation of the entire stifle,
the receptors in the CrCL constitute only a small
minority. It seems, however, that the canine
CrCL has more mechanoreceptors than other
species. According to Arcand et al. (2000), more
than 450 receptors could be identified in the
canine CrCL compared to very few receptors in
humans (<20) (Hogervost & Brand 1998) and
cats (<50) (Madey et al. 1997). The comparison
should be interpreted with caution due to different study designs and detection techniques.
It is, however, an interesting observation, as cats
and humans produce less severe osteoarthritis
after CrCL rupture compared to dogs. Free
nerve endings are mainly nociceptors, which
react to inflammation and pain stimuli (Cole
et al. 1996). Vasoactive neuropeptides, such
as substance P, have been reported in free
nerve endings and are thought to behave as
vasoactive substances. Free nerve endings do,
therefore, not only transfer information but
also have effector functions such as vasodilation, vascular permeability, and effects on the
immune system (Hogervost & Brand 1998). In
considering this information, and the fact that
the CrCL helps to maintain joint stability and is
beneficial in preventing meniscal tears, it seems
that total debridement of the partially ruptured
CrCL should be used cautiously.
Since the introduction of arthroscopy, diagnosis and surgical treatment of cruciate ligament rupture has been performed much earlier
during the disease process. Early detection of
anatomic partial ruptures of the CrCL has consequently increased. This is documented by the
fact that before the introduction of arthroscopy
in CR treatment an incidence of 8% of partially
ruptured CrCL diagnosed during surgery was
reported during the 1990s (Scavelli et al. 1990)
compared to 21% in 2000 (Ralphs & Whitney
2002) and 41% observed during a period in
which arthroscopy has become a routine procedure (Gatineau et al. 2011). With this evolution in mind, it has become very important to assess the different possibilities of CrCL
debridement. Intraoperative decisions of how
much to debride can be very difficult. Accurate
visual grading of the percentage of torn CrCL is
difficult because ligament tissue that appears to
be intact may mask a substantial injury. Plastic
deformation is possible and leads to a lax nonfunctional ligament. Electrothermal shrinkage
of collagen fibers of a lax ligament is potentially
possible, and has been used in the treatment of
lax ACLs in humans (Lamar et al. 2005). After
initial promising results, however, a multicenter study showed a high failure rate for thermal
shrinkage, with the conclusion that this was not
an appropriate treatment (Smith et al. 2008).
Ligament debridement for complete
CrCL rupture
It is well known that ruptured cruciate ligaments do not heal spontaneously (Hefti et al.
1991), and mechanoreceptors probably do not
regenerate and have a questionable function without physiologic tension (Hogervost &
Brand 1998). Further, some believe that remnants of the ligament might be an inflammatory trigger and increase osteoarthritis. Experimentally, it has been shown that CrCL remnants
disappear 3 months after CrCL transection
in rabbits (Hefti et al. 1991). In canine clinical and experimental cases, resorption of the
torn ligament is also possible. However, in
contrast nodular, vascularized swellings (Figure 34.1A,B) or drumstick formations of the free
(A)
(B)
Figure 34.1 Macroscopic view of two canine stifle
joints after experimental cranial cruciate ligament (CrCL)
transection 12 months earlier. Note the marked cartilage
degeneration, meniscal damage and (A) CrCL resorption
versus (B) CrCL vascularized proliferation.
293
VetBooks.ir
Cranial Cruciate Ligament Debridement
Figure 34.2 Arthroscopic view of a chronic partially
ruptured cranial cruciate ligament with visible torn fibers.
Note the formation of a ‘drumstick’ proliferation of the
ruptured fibers.
ends of the torn ligament (Figure 34.2) are also
often present and might disturb normal motion.
Therefore, the debridement of totally ruptured
ligaments is still an appropriate and indicated
therapy that is usually performed before meniscal inspection, using a motorized shaver during
arthroscopy. Advances in human primary ACL
repair, including stabilization of the repaired
ligament with an internal dynamic femur to
tibia suture, is likely to be protective and may
allow healing (Kohl et al. 2013). The provision of a suitable biological environment by
the addition of collagen matrix-embedded stem
cells or platelet-rich plasma (PRP) to a primary
repair (Joshi et al. 2009), in combination with an
internal stabilizing implant, are possible future
directions that will change the debridement discussion in complete CrCL rupture.
Ligament debridement for partial CrCL
rupture
The debridement of torn fibers in partially ruptured CrCL is indicated (Figure 34.2). Shortterm negative consequences of partial debridement compared to total debridement could not
be demonstrated (Wolf et al. 2008). Especially
with small partial tears, it is indicated to debride
visibly torn fibers using a motorized shaver
(Figure 34.3). A radiofrequency energy probe
can be used if shaver debridement is not satisfactory. Application using the lowest possible
Figure 34.3 Arthroscopic view of a partially ruptured
cranial cruciate ligament during debridement of torn
fibers with a motorized shaver using a 2.0 mm full radius
resector blade. The blade is positioned with the back of
the shaver lying against the intact ligament part to protect
viable intact fibers.
energy and an appropriate application velocity
is advised to reduce the risk of thermal injury
in the remaining tissue (Lu et al. 2007). During
debridement of the partially ruptured CrCL it
is important to save the fat pad as much as possible, as this is one of the major origins of the
vascular supply of the CrCL (Kobayashi et al.
2006).
Dogs with partial cruciate ligament rupture
have a lesser incidence of meniscal injury compared to dogs with complete rupture (Ralphs &
Whitney 2002). One reason for this could be that
the remaining ligament inhibits tibial translation to a certain degree, which in turn decreases
the risk of meniscal injury. Clinical observations
have shown that surgical interventions which
dynamically stabilize the stifle joint have an
influence on the remnants of the ligament (Eggli
et al. 2015). Dogs with palpably stable stifle
joints that have an arthroscopically diagnosed
partial CrCL rupture seem to benefit from the
debridement of visible torn fibers, followed by
a dynamic stabilization procedure such as tibial plateau leveling osteotomy (TPLO). Subsequent meniscal injuries seem to be uncommon
in this patient group, supporting the theory that
CrCL remnants maintain a better stability of the
joint. Second-look arthroscopies have shown
an improved appearance of the intact part of
the CrCL, most likely because the TPLO procedure reduces the strain on the CrCL (Hulse
VetBooks.ir
294
Surgical Treatment
et al. 2010). As with complete ruptures, there are
novel interesting studies showing the potential
of biological products such as PRP to promote
CrCL healing (Cook et al. 2016).
References
Adachi N, Ochi M, Uchio Y, et al. Mechanoreceptors in the anterior cruciate ligament contribute
to the joint position sense. Acta Orthop Scand
2002;73:330–334.
Arcand MA, Rhalmi S, Rivard CH. Quantification of
mechanoreceptors in the canine anterior cruciate
ligament. Int Orthop 2000;24:272–275.
Bray RC, Leonard CA, Salo PT. Vascular physiology
and long-term healing of partial ligament tears.
J Orthop Res 2002;20:984–989.
Cole KJ, Daley BJ, Brand RA. The sensitivity of
joint afferents to knee translation. Sportverletz
Sportschaden 1996;10:27–31.
Cook JL, Smith PA, Bozynski CC, et al. Multiple injections of leukoreduced platelet rich plasma reduce
pain and functional impairment in a canine model
of ACL and meniscal deficiency. J Orthop Res
2016;34:607–615.
DeFranco MJ, Bach BR, Jr. A comprehensive review of
partial anterior cruciate ligament tears. J Bone Joint
Surg 2009;91A:198–208.
Eggli S, Kohlhof H, Zumstein M, et al. Dynamic
intraligamentary stabilization: novel technique for
preserving the ruptured ACL. Knee Surg Sports
Traumatol Arthrosc 2015;23:1215–1221.
Gatineau M, Dupuis J, Planté J, et al. Retrospective
study of 476 tibial plateau levelling osteotomy procedures. Rate of subsequent ‘pivot shift’, meniscal tear and other complications. Vet Comp Orthop
Traumatol 2011;24:333–341.
Hefti FL, Kress A, Fasel J, et al. Healing of the transected anterior cruciate ligament in the rabbit.
J Bone Joint Surg 1991;73A:373–383.
Hogervorst T, Brand RA. Mechanoreceptors in
joint function. J Bone Joint Surg 1998;80A:1365–
1378.
Hulse D, Beale B, Kerwin S. Second look arthroscopic
findings after tibial plateau leveling osteotomy. Vet
Surg 2010;39:350–354.
Joshi SM, Mastrangelo AN, Magarian EM, et al.
Collagen-platelet composite enhances biomechanical and histologic healing of the porcine anterior
cruciate ligament. Am J Sports Med 2009;37:2401–
2410.
Kobayashi S, Baba H, Uchida K, et al. Microvascular system of anterior cruciate ligament in dogs.
J Orthop Res 2006;24:1509–1520.
Kohl S, Evangelopoulos DS, Kohlhof H, et al. Anterior crucial ligament rupture: self-healing through
dynamic intraligamentary stabilization technique.
Knee Surg Sports Traumatol Arthrosc 2013;21:599–
605.
Lamar DS, Bartolozzi AR, Freedman KB, et al. Thermal modification of partial tears of the anterior cruciate ligament. Arthroscopy 2005;21:809–814.
Lu Y, Meyer ML, Bogdanske JJ, et al. The effects
of radiofrequency energy probe speed and application force on chondrocyte viability. Vet Comp
Orthop Traumatol 2007;20:34–37.
Madey SM, Cole KJ, Brand RA. Sensory innervation of the cat knee articular capsule and cruciate ligament visualised using anterogradely transported wheat germ agglutinin-horseradish peroxidase. J Anat 1997;190:289–297.
Noyes FR, Mooar LA, Moorman CT, 3rd, et al. Partial
tears of the anterior cruciate ligament. Progression
to complete ligament deficiency. J Bone Joint Surg
1989;71B:825–833.
Ralphs SC, Whitney WO. Arthroscopic evaluation
of menisci in dogs with cranial cruciate ligament
injuries: 100 cases (1999–2000). J Am Vet Med Assoc
2002;221:1601–1604.
Scavelli TD, Schrader SC, Matthiesen DT, et al. Partial
rupture of the cranial cruciate ligament of the stifle
in dogs: 25 cases (1982–1988). J Am Vet Med Assoc
1990;196:1135–1138.
Smith DB, Carter TR, Johnson DH. High failure rate
for electrothermal shrinkage of the lax anterior
cruciate ligament: a multicenter follow-up past 2
years. Arthroscopy 2008;24:637–641.
Vasseur PB. Stifle joint. In: Textbook of Small Animal
Surgery, Slatter D, ed. Third edition. Philadelphia
PA, WB Saunders, 2002, pp. 2090–2132.
Wolf R, Beale B, Whitney W. Effect of debridement of
the cranial cruciate ligament in dogs having early
partial tears of the cranial cruciate ligament at the
time of TPLO. Vet Surg 2008;37:E2.
VetBooks.ir
35
Surgical Treatment of
Concurrent Meniscal Injury
Samuel P. Franklin, James L. Cook, and Antonio Pozzi
Introduction
Meniscal pathology in conjunction with cruciate ligament rupture (CR) is common and is
recognized in up to 83% of cases (Ritzo et al.
2014). When CR is present in dogs, the caudal
aspect of the medial meniscus is most predisposed to clinically important injury because
the femoral condyle subluxates caudally in the
unstable stifle (Rey et al. 2014). The types of
injury commonly seen in dogs include longitudinal, bucket-handle, radial, horizontal, caudal
peripheral and complex tears (Figure 35.1). It
is imperative that meniscal problems are diagnosed and treated at the time of initial surgery
in order to ensure optimal relief of pain,
the debridement of abnormal tissue causing
inflammation and degradation, patient recovery, and functional outcomes while minimizing
morbidity and the potential need for additional
surgeries.
Diagnosis
The preoperative diagnosis of meniscal pathology, including complete physical examination, joint palpation, and imaging, should be
comprehensively pursued. These diagnostic
approaches are addressed in Chapters 15, 18,
19, 20, 21, and 22. Arthroscopy with probing is reported to be the ‘gold standard’ for
a definitive diagnosis of meniscal pathology
because it allows for complete examination with
magnification, manipulation of the tissue, is
minimally invasive with low morbidity, and
enables the identification of meniscal pathology more commonly than arthrotomy (Thieman et al. 2006; Pozzi et al. 2008a; Ritzo et al.
2014). Arthrotomy via medial, lateral, or caudomedial approaches with probing is recommended if arthroscopy of the stifle is not possible. Various instruments are available to aid
in exposure and access for meniscal assessment
and treatment for both arthroscopic and open
approaches to stifle surgery. These instruments
include probes, Hohmann retractors, micropicks, self-retaining retractors, and distraction
devices. There is evidence that these instruments can improve observation and identification of meniscal tears, and so are highly recommended (Pozzi et al. 2008a; Winkels et al. 2016).
In addition, assessment of the menisci with the
joint in flexion and extension, with varus and
valgus stress of the joint, and with internal and
external rotation of the stifle can improve diagnostic accuracy. An accurate and comprehensive assessment of the menisci is the critical first
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
295
Surgical Treatment
VetBooks.ir
296
(A)
(B)
(C)
JC
(D)
(E)
(F)
Figure 35.1 Illustrations of longitudinal (A), bucket-handle (B), radial (C), horizontal (D), caudal peripheral (E), and
complex (F) tears. JC, Joint capsule. Copyright © Samantha J. Elmhurst at www.livingart.org.uk.
step in the appropriate surgical treatment of
meniscal pathology in dogs. Indeed, at least two
studies have demonstrated that dogs in which
meniscal pathology is identified have a greater
likelihood of a successful outcome than dogs in
which meniscal pathology has not been identified (Ertelt & Fehr 2009; Ritzo et al. 2014).
Treatment
Once meniscal pathology is identified and characterized, three major treatment options can be
considered, namely repair, resection, or release
(radial transection). The repair of longitudinal,
bucket-handle, and horizontal tears is technically feasible by open or arthroscopic placement
of sutures, can restore normal contact mechanics in the stifle ex vivo, and may be indicated in
selected cases (Cook & Fox 2007; Luther et al.
2007; Thieman et al. 2009; Thieman et al. 2010).
However, the majority of meniscal pathology
in dogs is still treated via resection or release
because meniscal repair is perceived as being
prone to failure in most dogs, based on both biologic and biomechanical factors. The primary
biologic factors involved are:
1. The majority of tears occur in the axial
(inner) 75% of the meniscus, which has no
or poor inherent blood supply and low cell
density.
2. The majority of dogs with CR and meniscal
pathology have active osteoarthritis with
associated inflammation and degradation
processes at work.
3. Meniscal tears in dogs are typically chronic,
with associated microstructural changes
present in the tissue.
The biomechanical issues center on an inability to restore normal joint kinematics to the
cranial cruciate ligament (CrCL)-deficient stifle. Combined, these detriments to successful
healing and restoration of function to damaged
menisci suggest that careful decision-making
regarding meniscal repair in dogs is needed,
even when it is technically feasible to accomplish. As surgical techniques become more
refined and developed to be more effective and
consistent in stabilizing the CrCL-deficient stifle, the role of meniscal repair may become more
pertinent.
The resection of pathologic meniscal tissue
is the most commonly recommended and performed treatment for meniscal injuries in dogs
at this time. Partial meniscectomy, segmental
meniscectomy (caudal hemimeniscectomy),
and total meniscectomy are the three types of
resection procedure typically used for dogs
(Table 35.1). These can be accomplished arthroscopically or after arthrotomy. Scalpel blades
(#11, #15, or Beaver blades), meniscal knives,
and arthroscopic basket forceps, scissors,
meniscal cutting tools designed specifically
for meniscus removal in dogs, and shavers
can be used to perform the resections.
VetBooks.ir
Surgical Treatment of Concurrent Meniscal Injury
297
Table 35.1 Meniscal resection procedures used in dogs.
Procedure
Illustration
Indication
Partial meniscectomy
All meniscal tears that allow for a
peripheral rim to be preserved
Segmental meniscectomy
(caudal hemimeniscectomy)
Caudal meniscal tears where a
functional rim cannot be preserved
Total meniscectomy
All meniscal tears involving more
than caudal aspect and the rim
cannot be preserved
Note: Images have been reproduced from Johnson et al. (2004), with permission from the American Veterinary Medical
Association.
Partial meniscectomy is indicated for longitudinal, bucket-handle, radial, horizontal, and
complex tears for which an intact rim (peripheral circumferential collagen fiber integrity) can
be preserved after resection. Segmental meniscectomy is indicated for all types of tears in the
caudal aspect of the meniscus when an intact
rim cannot be preserved in conjunction with
complete resection of pathologic tissue. Total
meniscectomy is indicated for tears extending
beyond the caudal aspect of the meniscus, and
for which an intact rim cannot be maintained.
There are several key factors to consider
in order to optimize meniscal resection procedures. First, exposure and access must be
achieved, such that adjacent structures (articular cartilage, ligaments, etc.) are not damaged
during resection. Instrumentation specifically
designed for meniscal surgery is recommended
for minimizing iatrogenic damage to the articular cartilage during assessment and treatment. Two important goals must then be balanced in performing the resection: (i) remove
all grossly damaged, displaced, and pathologic
meniscal tissue; and (ii) preserve as much functional meniscal tissue as possible. Damaged,
displaced, unstable, and pathologic meniscal
tissue can cause mechanical dysfunction in the
joint, direct articular cartilage damage, inflammation and degradation, and resultant pain,
lameness, and progression of osteoarthritis.
However, loss or removal of meniscal tissue,
especially the peripheral rim, severely diminishes load-bearing, shock absorption, congruency, stability, lubrication, tissue nutrition, and
the chondroprotection functions of the meniscus for the joint (see Chapter 4). Clearly, the
two goals for treatment of meniscal injuries
can be at odds to one another, and so careful evaluation and decision-making with judicious resection are critical to striking the optimal balance for the patient. The evaluation is
based on preoperative imaging, in conjunction
with a careful inspection of the entirety of the
meniscus, probing and palpation of meniscal
tissue and its attachments, and an assessment
of the articular cartilage of the femoral condyle
and tibial plateau. Healthy, functional meniscal
Surgical Treatment
VetBooks.ir
298
1
2
3
(A)
(B)
Figure 35.2 Illustrations of caudal (A) and central radial (B) transections of the medial meniscus for meniscal release in
dogs. 1, Gerdy’s tubercle; 2, popliteal tendon; 3, caudal menisco-tibial ligament of the medial meniscus. The radial
incision for the central release is made just behind the medial collateral ligament, with the blade aligned with Gerdy’s
tubercle. Copyright © Samantha J. Elmhurst at www.livingart.org.uk.
tissue should appear smooth, white, and glistening and not be readily displaced, folded,
separated, or penetrated with a blunt arthroscopic probe. Abnormal meniscal tissue is typically soft, fibrillated, discolored and abnormal
in location, architecture, and integrity, and is
often associated with local articular cartilage
damage. Taken together, these variables help to
distinguish pathologic from functional meniscal tissue and guide the surgeon in determining
what to resect and what to preserve.
Meniscal release, or radial transection, is the
other procedure commonly performed in dogs
for the treatment or attempted prevention of
meniscal injuries. The rationale behind meniscal release is that the surgeries performed to stabilize CrCL-deficient stifles do not consistently
restore normal kinematics, and, therefore, the
medial meniscus remains at risk of subsequent
damage with intermittent or periodic caudal
femoral subluxation (Kim et al. 2012). Accordingly, the meniscus can be released at the time of
the stifle stabilization procedure, allowing it to
displace caudally with the femoral condyle and
prevent subsequent damage, tearing, and associated lameness. In this way, the need for additional surgery to treat post stifle-stabilization
meniscal tears can be minimized. Importantly, it
has been suggested that many meniscal injuries
diagnosed after the initial surgery for CR may
instead be tears that were present, but undetected, at the original surgery (Metelman et al.
1995; Thieman et al. 2006). This further highlights the importance of careful inspection and
probing of the menisci during the first surgical
procedure.
Radial transection for medial meniscal release
can be performed at the caudal meniscal horn–
caudal meniscotibial ligament junction (caudal
release), or at the mid-body of the meniscus
(central release) via arthroscopy or arthrotomy
using scalpel blades (#11, #15, or Beaver blades)
or meniscal knives (Figure 35.2). While meniscal releases can be associated with a significantly lower risk for clinically apparent subsequent meniscal tears (Thieman et al. 2006;
Ritzo et al. 2014), radial transection of the meniscus, regardless of location, completely disrupts
the circumferential collagen fiber integrity (rim)
and destroys critical meniscal functions (Pozzi
et al. 2006; Pozzi et al. 2008b; Luther et al.
2009). The released menisci will not functionally heal and will remain biomechanically deficient (Cook et al. 2016). Meniscal release alone
in CrCL-intact stifles in dogs results in articular cartilage loss, further meniscal pathology,
osteoarthritis, and lameness within 12 weeks
(Luther et al. 2009). In clinical patients with
CR, however, clinically significant differences
in outcome between groups receiving or not
receiving meniscal release have not been noted
based on subjective assessments (Thieman et al.
2006; Ritzo et al. 2014). As such, the present
authors suggest that meniscal release can be justified when the meniscus cannot be full assessed
for pathology, cannot be sufficiently resected
safely, or the subsequent meniscal tear rate is
unacceptably high to the surgeon or the client.
VetBooks.ir
Surgical Treatment of Concurrent Meniscal Injury
299
Table 35.2 Current best evidence for and against use of meniscal release in dogs.
Evidence FOR meniscal release
Evidence AGAINST meniscal release
Significantly reduces the rate of subsequent meniscal
tears (Thieman et al. 2006; Ritzo et al. 2014)
Does not eliminate subsequent tears (Thieman et al. 2006)
No clinically significant differences in subjective
outcome (Thieman et al. 2006; Ritzo et al. 2014)
Eliminates biomechanical functions of meniscus
equivalent to total meniscectomy (Pozzi et al. 2006;
Pozzi et al. 2008)
Released menisci will not functionally heal (Luther et al.
2009; Cook et al. 2016)
Release alone associated with full-thickness cartilage
loss, radiographic osteoarthritis, and lameness (Luther
et al. 2009)
The authors suggest that the options, decisionmaking process, and ramifications associated
with meniscal release should be discussed with
the client during the preoperative consultation
and consent to treatment (Table 35.2).
Conclusion
Meniscal injuries concurrent with CR in dogs
are very common. As a good rule of thumb, if
meniscal pathology is not recognized in at least
50% of patients with CR, it is very likely that
tears are being missed. Preoperative assessment
by palpation and imaging, combined with careful and meticulous intraoperative assessment
with probing and palpation of meniscal tissue,
are the keys to a comprehensive diagnosis of
meniscal pathology. Once accurate and complete assessment has been performed, a treatment algorithm for meniscal injury concurrent
with CR can be applied based on the location and severity of the pathology, the technical aspects of the various procedures, and
Cruciate ligament rupture
Preoperative Diagnostics
(Palpation, Radiographs, Ultrasound, MRI)
Surgical Assessment
(Arthroscopy or Arthrotomy with Probing)
Meniscal Pathology Present
No Meniscal Pathology Seen
Resection
Damaged tissue accessible
Document and leave intact
Low subsequent tear rate
Release
Damaged tissue inaccessible
Release
Cannot fully assess
High subsequent tear rate
Client communication
Repair
In vascular zone
Functional tissue
Kinematics restored
Technically feasible
Client communication
Figure 35.3
Algorithm for decision-making regarding the surgical treatment of meniscal injuries in dogs.
VetBooks.ir
300
Surgical Treatment
subsequent tear rates for the surgeries performed in the individual practice setting (Figure 35.3). Informing the client of the risks and
benefits associated with the various options,
and involving them in the decision-making
process, is not only appropriate but is also
imperative for optimal delivery of care in a
patient- and client-based approach to small animal orthopaedic surgery.
References
Cook JL, Fox DB. A novel bioabsorbable conduit augments healing of avascular meniscal tears in a dog
model. Am J Sports Med 2007;35:1877–1887.
Cook JL, Smith PA, Bozynski CC, et al. Multiple injections of leukoreduced platelet rich plasma reduce
pain and functional impairment in a canine model
of ACL and meniscal deficiency. J Orthop Res
2016;34:607–615.
Ertelt J, Fehr M. Cranial cruciate ligament repair in
dogs with and without meniscal lesions treated by
different minimally invasive methods. Vet Comp
Orthop Traumatol 2009;22:21–26.
Kim SE, Lewis DD, Pozzi A. Effect of tibial plateau
leveling osteotomy on femorotibial subluxation: in vivo analysis during standing. Vet Surg
2012;41:465–470.
Luther JK, Cook CR, Constantinescu IA, et al. Clinical
and anatomical correlations of the canine meniscus.
J Exp Med Surg Res 2007;14:5–14.
Luther JK, Cook CR, Cook JL. Meniscal release in cruciate ligament intact stifles causes lameness and
medial compartment cartilage pathology in dogs
12 weeks postoperatively. Vet Surg 2009;38:520–
529.
Metelman LA, Schwarz PD, Salman M, et al. An evaluation of three different cranial cruciate ligament
surgical stabilization procedures as they relate to
postoperative meniscal injuries. Vet Comp Orthop
Traumatol 1995;8:118–123.
Pozzi A, Kowaleski MP, Apelt D, et al. Effect of medial
meniscal release on tibial translation after tibial
plateau leveling osteotomy. Vet Surg 2006;35:486–
494.
Pozzi A, Hildreth BE, 3rd, Rajala-Schultz PJ. Comparison of arthroscopy and arthrotomy for diagnosis
of medial meniscal pathology: an ex vivo study. Vet
Surg 2008a;37:749–755.
Pozzi A, Litsky AS, Field J, et al. Pressure distributions
on the medial tibial plateau after medial meniscal surgery and tibial plateau levelling osteotomy
in dogs. Vet Comp Orthop Traumatol 2008b;21:8–
14.
Rey J, Fischer MS, Böttcher P. Sagittal joint instability
in the cranial cruciate ligament insufficient canine
stifle. Caudal slippage of the femur and not cranial tibial subluxation. Tierarztl Prax 2014;42:151–
156.
Ritzo ME, Ritzo BA, Siddens AD, et al. Incidence
and type of meniscal injury and associated longterm clinical outcomes in dogs treated surgically
for cranial cruciate ligament disease. Vet Surg
2014;43:952–958.
Thieman KM, Tomlinson JL, Fox DB, et al. Effect of
meniscal release on rate of subsequent meniscal
tears and owner-assessed outcome in dogs with
cruciate disease treated with tibial plateau leveling
osteotomy. Vet Surg 2006;35:705–710.
Thieman KM, Pozzi A, Ling H, et al. Contact mechanics of simulated meniscal tears in cadaveric canine
stifles. Vet Surg 2009;38:803–810.
Thieman KM, Pozzi A, Ling H, et al. Comparison of
contact mechanics of three meniscal repair techniques and partial meniscectomy in cadaveric dog
stifles. Vet Surg 2010;39:355–362.
Winkels P, Pozzi A, Cook R, et al. Prospective evaluation of the Leipzig stifle distractor. Vet Surg
2016;45:631–635.
VetBooks.ir
36
Meniscal Release
Antonio Pozzi and James L. Cook
Introduction
Meniscal pathology is commonly reported in
conjunction with cruciate ligament rupture
(CR) (Flo 1993; Williams et al. 1994; Ralphs &
Whitney 2002; Luther et al. 2007), or at some
point after surgical treatment of the cranial
cruciate ligament (CrCL)-deficient stifle joint
(Metelman et al. 1995; Thieman et al. 2006;
Lafaver et al. 2007; Case et al. 2008). Chronic
stifle instability resulting from CR causes supraphysiologic loading of the menisci, particularly
shear and compression of the caudal pole of the
medial meniscus, resulting in meniscal tears.
When surgical treatments do not fully restore
stifle kinematics, as is the case for the majority
of surgical procedures, the menisci are still at
risk after treatment. Meniscal pathology noted
at the time of initial surgery is termed ‘concurrent’ or ‘coincident,’ and when diagnosed after
surgery it is said to be ‘subsequent,’ ‘latent,’ or
‘postliminary.’ Concurrent meniscal pathology
is recognized in between 20% and 77% of cases
(Flo 1993; Williams et al. 1994; Ralphs & Whitney 2002; Mahn et al. 2005; Luther et al. 2007),
while subsequent meniscal injury is recognized
in between 3% and 100% of cases (Metelman
et al. 1995; Slocum & Slocum 1998; Thieman
et al. 2006; Lafaver et al. 2007; Case et al. 2008). It
has been suggested that some cases diagnosed
as subsequent meniscal tears may in fact have
been concurrent tears that were misdiagnosed
(latent tears). The rest of the subsequent tears
that occur after CR surgery are called postliminary tears. Because subsequent tears are often
associated with pain and lameness and necessitate a second surgery, veterinary surgeons have
aimed for improved diagnostic approaches to
meniscal disease in dogs (see Chapters 18, 19,
20, and 21) and strategies for prevention of subsequent meniscal pathology in a comprehensive
approach to treatment of CR.
One strategy designed to prevent subsequent meniscal injuries is release of the medial
meniscus by radial transection at the caudal
meniscotibial ligament of the medial meniscus (caudal release) or at the midbody of the
medial meniscus. Medial meniscal release is
theorized to free the caudal pole from exposure to the abnormal loads delivered during
weight-bearing in the CrCL-deficient canine
stifle joint (Slocum & Slocum 1998; Kennedy
et al. 2005; Pozzi et al. 2006). The clinical
goal of meniscal release is to eliminate any
impingement of the meniscus between the
femoral and tibial condyles, described as the
‘wedging phenomenon’ (see Chapter 4), and in
doing so decrease the likelihood of subsequent
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
301
VetBooks.ir
302
Surgical Treatment
meniscal pathology. The theoretical mechanism
and clinical goal seem to be realized in general.
However, the biomechanical and biological consequences are significant and the procedure is
not always effective in accomplishing its objective. Therefore, the pros and cons of meniscal
release should be carefully weighed in determining indications and communicating options
and prognoses to clients.
Effect of meniscal release on joint
biomechanics and biology
Medial meniscal release involves a complete
radial transection of the tissue. Several studies have investigated the effects of release on
meniscal function to determine if this procedure
has detrimental effects on the joint (Pozzi et al.
2006; Pozzi et al. 2008; Luther et al. 2009; Pozzi
et al. 2010). The complex material properties
and functional anatomy of the meniscus allows
it to absorb energy by undergoing constrained
elongation, as a load is applied through the stifle (see Chapter 4). As the joint compresses, the
wedge-shaped meniscus will normally slightly
extrude peripherally as its circumferentially
oriented collagen fibers elongate. Extrusion and
elongation are limited by the large tensile hoop
stress developed within the strong circumferential collagen fibers bundles of the menisci
and their cranial and caudal attachments to
tibial bone. This hoop stress is critical to normal
meniscal functions and joint health. Meniscal
release eliminates the ability of the meniscus
to develop necessary hoop tension. Similar to
a hammock that has lost its anchor points, a
released meniscus ‘collapses’ and undergoes
unconstrained extrusion under weight-bearing
because of the lack of continuous circumferential fibers with cranial and caudal attachments
(see also Chapter 4; Figure 4.4). The radial
transection renders the meniscus functionally
equivalent to a hemi- or a complete meniscectomy (Pozzi et al. 2008). Ex vivo studies have
shown that radial transections at various locations redistribute and concentrate the weightbearing load to a small area in the caudal aspect
of the femoro-tibial articulation (Figure 36.1)
(Pozzi et al. 2008; Pozzi et al. 2010). As expected,
complete radial transection, release, at any
(A)
(B)
Figure 36.1 Illustration of contact pressures obtained
from the Tekscan software in the tibial plateau leveling
osteotomy-treated cranial cruciate ligament-deficient
stifle with an intact meniscus (A) and after transection of
the caudal menisco-tibial ligament (B). The caudal
meniscal release resulted in a reduced area and increased
pressure; the load across the medial compartment shifted
completely to the caudal half of the compartment. The
caudal meniscotibial ligament release and the mid-body
release are equivalent because they eliminate the hoop
tension and the ability of the meniscus to control the
radially directed force developing from axial
compression. Source: Pozzi et al. 2009. Reproduced with
permission from John Wiley & Sons, Inc.
point in the meniscus causes a 50% decrease in
contact area and a 40% increase in magnitude of
articular surface stress in the medial compartment of CrCL-deficient stifles treated with a
TPLO (Pozzi et al. 2010). The contribution of the
meniscus to joint stability is also crucial (Pozzi
et al. 2006). By effectively deepening the tibial
contact surface, the meniscus improves joint
congruity and acts as a secondary stabilizer.
This role of the intact meniscus is especially
VetBooks.ir
Meniscal Release
important after surgical treatment of the
CrCL-deficient stifle, since no current modality
affords the restoration of normal stifle kinematics (Kim et al. 2012). Functional menisci may
contribute to improved stifle kinematics and
contact mechanics after surgery, while meniscal
release effectively eliminates the stabilizing
properties of the tissue. Loss of these critical
functions after meniscal release has severe
ramifications for the health and function of the
stifle joint. Since meniscal release is functionally
equivalent to meniscectomy, severe cartilage
degeneration can be expected (Fairbank 1948),
and an in vivo experimental study in dogs
showed that meniscal release in CrCL-intact
stifles resulted in severe articular cartilage
pathology as early as 12 weeks after surgery
(Luther et al. 2009) (Figures 36.2 and 36.3). In
addition, meniscal release alone was associated
with lameness, radiographic changes consistent
with osteoarthritis, and further meniscal damage in these dogs (Luther et al. 2009). The effect
of meniscal release in a CrCL-deficient stifle
may be less evident, considering the abnormal
joint biomechanics caused by CrCL rupture.
However, it could be argued that for this reason
the meniscus should be preserved at any cost,
despite the risk of reoperation because of a
subsequent meniscal tear.
Surgical technique
Two types of meniscal release are routinely
performed. The abaxial or mid-body or central
meniscal release is performed by radial transection of the meniscus immediately caudal
to the medial collateral ligament. The axial
or menisco-tibial ligament or caudal meniscal
release is characterized by a radial transection
at the junction of the menisco-tibial ligament
and the caudal pole of the medial meniscus
(Kennedy et al. 2005) (see Chapter 35). Meniscal
release can be performed either through an
open approach or arthroscopically (Slocum &
Slocum 1998; Luther et al. 2009). Regardless
of approach, the basic principles of meniscal
surgery should be followed: (i) optimize exposure and joint distraction before performing the
release; 2) use atraumatic surgical technique.
Exposure and assessment of the meniscus
is a crucial step in performing any meniscal
303
M
(A)
M
(B)
Figure 36.2 Photograph of right tibial plateau of
disarticulated right stifle 12 weeks after experimental
caudal menisco-tibial release (MR) in a stifle with an
intact cranial cruciate ligament (A) and sham surgery (B).
The metallic probe indicates the junction of the caudal
horn and the caudal meniscal ligament of the medial
meniscus, where MR was performed. Healing of the
caudal horn MR site was minimal and limited to the
abaxial region. Note the gross articular fibrillation on the
medial aspect of the tibial plateau. Medial meniscus (M).
Source: Luther et al. 2009. Reproduced with permission
from John Wiley & Sons, Inc.
treatment, including meniscal release. For
arthrotomy and arthroscopy, the combination
of joint distraction, femoro-tibial subluxation,
varus and valgus stress applied to the stifle
allows examination of the entire meniscus in
some cases (Pozzi et al. 2008). Improved exposure can be achieved by using stifle distractors.
Exposure of the meniscus is more challenging
in the stable stifle with partial CR. In these
cases, debridement of the entire CrCL or exposure of the caudal pole of the meniscus through
a caudo-medial approach should be considered
(Pozzi et al. 2008). After exposure, every region
of the meniscus is accurately probed to evaluate
its firmness, smoothness, and for the presence
of tears (Pozzi et al. 2008). Latent tears may
Surgical Treatment
VetBooks.ir
304
(A)
(B)
(C)
(D)
Figure 36.3 Representative gross appearances of India ink-stained articular cartilage surfaces in meniscal release (MR)
(A,B) and sham-operated (C,D) stifle joints. The photographs were taken immediately after tracings of the articular
surfaces and lesions were made. The percentage area of cartilage damage was significantly greater in MR stifles than in
sham stifles, as indicated here by the darkly stained regions on the medial femoral condyle and tibial plateau. Source:
Luther et al. 2009. Reproduced with permission from John Wiley & Sons, Inc.
occur due to misdiagnosis at the time of the initial joint evaluation (Thieman et al. 2006; Case
et al. 2008). Therefore, complete and careful
inspection for all types of pathology potentially
present is mandatory for comprehensive management of CR in dogs. Meticulous surgical
technique with an optimal view of the meniscus
(arthroscopy, head-lamp, appropriate surgical
lights) is also necessary to avoid iatrogenic damage to the cartilage, the medial collateral ligament and the caudal cruciate ligament (Austin
et al. 2007).
The mid-body release can be performed
using an inside-to-outside or an outside-toinside technique. For the inside-to-outside
technique, a needle is inserted into the joint
from outside at the level of the caudal edge
of the medial collateral ligament. The needle
guides the blade inserted from inside the joint
through the entire meniscus. In the outside-toinside technique, the #11 blade is inserted just
caudal to the medial collateral ligament in a
direction towards the Gerdy tubercle. Aiming
at the Gerdy tubercle should allow the surgeon
to transect the meniscus at a 30◦ cranio-medial
angle, which is necessary to accomplish a
complete release (Slocum & Slocum 1998). To
confirm that a complete release has been performed, a probe is used to evaluate the extent
of radial transection.
Menisco-tibial release is used more commonly in conjunction with cranio-medial
arthrotomy or arthroscopy. This is the preferred
method of the present authors because of the
lower risk of cartilage damage during transection. The menisco-tibial ligament can be transected with a #11, #15, or Beaver scalpel blade,
meniscal knives, or arthroscopic basket forceps
or scissors. Radiofrequency probes and electrosurgery devices have also been used but are
not recommended by the present authors due
to the potential for thermal damage to adjacent
tissues. The meniscal probe can be used while
releasing the meniscus to ensure that the whole
ligament is transected. The tip of the probe is
hooked onto the ligament and the probe is used
as a guide for the blade (Figure 36.4). An incomplete release is recognized using this technique
if the tip of the probe remains hooked after
transection. Another technique entails using
a pull-meniscal knife. This instrument allows
‘hooking’ and transecting the whole ligament
VetBooks.ir
Meniscal Release
(A)
(B)
Figure 36.4 (A) Photograph of right tibial plateau
illustrating the caudal menisco-tibial release using a
meniscal probe as a guide for the blade. The meniscal
release is completed as the tip of the probe is freed from
under the meniscal ligament. (B) Photograph of right
tibial plateau illustrating the caudal menisco-tibial release
using a pull-meniscal-knife. After hooking the ligament
with the knife, traction is applied until the ligament is
transected. Care should be taken to avoid hooking the
caudal cruciate ligament. The meniscal-tibial ligament
should be probed to confirm that the meniscal release is
complete. Both techniques can be performed via
arthrotomy or arthroscopy.
(Figure 36.4), and facilitates performing a complete release, potentially decreasing the risk of
iatrogenic damage to the joint.
Clinical decision-making
The optimal treatment of meniscal injury
should alleviate pain while preserving meniscal
305
function. If this principle is applied to clinical
decision-making regarding an intact meniscus,
meniscal release should not be performed
because of its impact on meniscal function and
consequently joint function (Pozzi et al. 2006;
Thieman et al. 2006; Pozzi et al. 2008; Luther
et al. 2009; Pozzi et al. 2010). This conservative
approach is further supported by the evidence
that dogs without meniscal injury and without
release have a better short- and long-term outcome (Innes et al. 2000; Luther et al. 2009). The
type of meniscal treatment may have a greater
impact on clinical outcome than does the CrCL
stabilization technique. Cases diagnosed and
treated for concurrent meniscal tears were 1.3fold more likely to have a successful long-term
outcome than cases in which a concurrent tear
was not identified (Ritzo et al. 2014). These
results would support a recommendation of
meniscal release to decrease the likelihood of
postoperative meniscal tears (Ritzo et al. 2014)
in selected cases when some postoperative
stifle laxity is to be expected.
A thorough evaluation of the meniscus
should be performed, especially if the meniscus is not released. Latent tears represent a failure of diagnosis at surgery and may result in
persistent lameness and require additional surgical treatment. To decrease the risk of latent
tears, arthroscopy and meniscal probing are recommended for their high sensitivity and specificity (Mahn et al. 2005; Pozzi et al. 2008). By
improving the diagnosis of tears at the initial
joint exploratory surgery, it may be possible to
decrease the incidence of late injuries to a point
that a release procedure may not be necessary.
Subsequent meniscal tears cause discomfort
to the patient and may require costly reoperation. Meniscal release decreases the rate
of these tears, thus eliminating the need for
revision surgeries in some dogs (Thieman et al.
2006). For this reason, meniscal release could be
considered in cases of high rates of subsequent
meniscal injury and when a revision surgery
is not acceptable for the owner. However, in
these cases consideration should be given to
hemimeniscectomy in place of meniscal release
because meniscal tears may still occur despite
a meniscal release. The decision of releasing
an intact meniscus is complex and should be
made after considering several factors that
include the diagnostic approach, the type of
VetBooks.ir
306
Surgical Treatment
CrCL stabilization technique, and client communication (see also Chapter 35; Table 35.1 and
Figure 35.3).
References
Austin B, Montgomery RD, Wright J, et al. Evaluation
of three approaches to meniscal release. Vet Comp
Orthop Traumatol 2007;20:92–97.
Case JB, Hulse D, Kerwin SC, et al. Meniscal injury
following initial cranial cruciate ligament stabilization surgery in 26 dogs (29 stifles). Vet Comp
Orthop Traumatol 2008;21:365–367.
Fairbank TJ. Knee joint changes after meniscectomy.
J Bone Joint Surg 1948;30B:664–670.
Flo GL. Meniscal injuries. Vet Clin North Am 1993;
23:831–843.
Innes JF, Bacon D, Lynch C, et al. Long-term outcome
of surgery for dogs with cranial cruciate ligament
deficiency. Vet Rec 2000;147:325–328.
Kennedy SC, Dunning D, Bischoff MG, et al. The
effect of axial and abaxial release on meniscal displacement in the dog. Vet Comp Orthop Traumatol
2005;18:227–234.
Kim SE, Lewis DD, Pozzi A. Effect of tibial plateau
leveling osteotomy on femorotibial subluxation:
in vivo analysis during standing. Vet Surg 2012;41:
465–470.
Lafaver S, Miller NA, Stubbs WP, et al. Tibial tuberosity advancement for stabilization of the canine cranial cruciate ligament-deficient stifle joint: surgical
technique, early results, and complications in 101
dogs. Vet Surg 2007;36:573–586.
Luther JK, Cook CR, Constantinescu IA, et al. Clinical
and anatomical correlations of the canine meniscus.
J Exp Med Surg Res 2007;14:5–14.
Luther JK, Cook CR, Cook JL. Meniscal release in cruciate ligament intact stifles causes lameness and
medial compartment cartilage pathology in dogs.
Vet Surg 2009;38:520–529.
Mahn MM, Cook JL, Cook CR, et al. Arthroscopic verification of ultrasonographic diagnosis of meniscal
pathology in dogs. Vet Surg 2005;34:318–323.
Metelman LA, Schwarz PD, Salman M, et al. An evaluation of three different cranial cruciate ligament
surgical stabilization procedures as they relate to
postoperative meniscal injuries. Vet Comp Orthop
Traumatol 1995;8:118–123.
Pozzi A, Litsky AS, Field J, et al. Pressure distributions
on the medial tibial plateau after medial meniscal surgery and tibial plateau levelling osteotomy
in dogs. Vet Comp Orthop Traumatol 2008;21:
8–14.
Pozzi A, Kowaleski MP, Apelt D, et al. Effect of medial
meniscal release on tibial translation after tibial
plateau leveling osteotomy. Vet Surg 2006;35:486–
494.
Pozzi A, Kim SE, Lewis DD. Effect of transection
of the caudal menisco-tibial ligament on medial
femorotibial contact mechanics. Vet Surg 2010;39:
489–495.
Ralphs SC, Whitney WO. Arthroscopic evaluation
of menisci in dogs with cranial cruciate ligament
injuries: 100 cases (1999–2000). J Am Vet Med Assoc
2002;221:1601–1604.
Ritzo ME, Ritzo BA, Siddens AD, et al. Incidence and
type of meniscal injury and associated long-term
clinical outcomes in dogs treated surgically for cranial cruciate ligament disease. Vet Surg 2014;43:
952–958.
Slocum B, Slocum TD. Meniscal Release. In: Current
Techniques in Small Animal Surgery, M Bojrab, ed.,
4th edn. Williams & Wilkins, Baltimore, MD, 1998,
pp. 1197–1199.
Thieman KM, Tomlinson JL, Fox DB, et al. Effect of
meniscal release on rate of subsequent meniscal
tears and owner-assessed outcome in dogs with
cruciate disease treated with tibial plateau leveling
osteotomy. Vet Surg 2006;35:705–710.
Williams J, Tomlinson J, Constantinescu GM. Diagnosing and treating meniscal injuries in the dog. Vet
Med 1994;89:42–47.
VetBooks.ir
37
Progression of Osteoarthritis
after Stifle Stabilization
Surgery
Susannah J. Sample
Introduction
The relationship between cruciate ligament
rupture (CR) and osteoarthritis (OA) is complex, dynamic, and poorly understood. Historically, development of OA in clinical patients
was perceived to be a consequence of a loss
of joint stability associated with cranial cruciate ligament (CrCL) fiber rupture. More recent
studies have indicated that, while joint instability resulting from CrCL fiber tearing increases
development of OA, initiation of OA within a
diseased stifle joint actually precedes clinically
detectable joint instability. This suggests that
CrCL fiber disruption is, at least in part, a consequence, rather than a cause, of the disease process that leads to stifle OA.
Use of cranial cruciate ligament
transection as a model of osteoarthritis
The historic view that OA in canine patients
with naturally occurring CR is purely a consequence of stifle instability is, in part, based on
dog model studies of CrCL transection. While
the development of OA in patients with naturally occurring disease is likely more complex,
it is important to consider the consequences of
stifle joint instability on the development and
progression of OA.
After transection of the CrCL, changes occur
throughout the tissues of the synovial joint.
The articular cartilage undergoes a dramatic
anabolic response, with increased cellular activity and mitosis resulting in increased matrix
synthesis and an overall increase in tissue mass
(Adams & Brandt 1991). However, this anabolic
activity is countered by increased catabolic
activity with degradation of the collagen network (Fernandes et al. 1998) and increased activity of enzymes degrading the major proteoglycan, aggrecan (Innes et al. 2005). The result of
this proteolytic activity is to deplete the cartilage of aggrecan, initially in the superficial zone,
and to disrupt the collagen network. Thus, the
compressive stiffness and the tensile strength
of the cartilage are both reduced. In a stifle
affected by CR, the consequences of cartilage
degradation can often be seen during arthroscopic assessment, as reflected by a decrease in
cartilage stiffness and eventual fraying (Figure
37.1). Continued enzymatic activity over many
months leads to loss of tissue, such that there
may be full-thickness cartilage lesions within 3
to 5 years (Brandt et al. 1991).
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
307
Surgical Treatment
VetBooks.ir
308
(A)
(B)
Osteoarthritis precedes stifle
instability associated with cruciate
ligament rupture
Some of the most pivotal findings identified
while investigating the association between
development of OA and its relationship to CR
have come from studies of contralateral stable stifles of dogs with unilateral complete
CR. Given that the risk of contralateral CR is
between 40% and 60% within 18 months of CR
diagnosis (Doverspike et al. 1993; de Bruin et al.
2007), use of the contralateral stable stifle in
dogs with unilateral stifle instability is advantageous in providing a model to study the natural
history of CR disease progression.
Based on results of investigations of clinically stable contralateral stifles in dogs with
unilateral CR, it has been established that radiographically detectable OA precedes CR (Doverspike et al. 1993; de Bruin et al. 2007; Bleedorn
et al. 2011; Chuang et al. 2014). This observation
has led to investigations into the use of radiographic OA as a means of prediction of complete CR risk in stifles with partial CR (see also
Chapter 22). Indeed, in contralateral stable stifles of dogs with unilateral CR, both the progression of OA over time (Innes et al. 2004; de
Bruin et al. 2007) and the degree of OA at the
time of diagnosis (Chuang et al. 2014) (see Chapter 22; Figures 22.2 and 22.3) are predictive of
risk of contralateral CR.
Interestingly, the presence of radiographically detectable OA in a contralateral stable stifle does not inevitability lead to complete CR,
highlighting that there is incomplete understanding of the initiating factors that result in
OA and cruciate ligament fiber rupture, and
Figure 37.1 Arthroscopic views of
medial femoral condyles in stifle
joints with cranial cruciate ligament
rupture. Note the cartilage
pathology present in both these
stifles. (A) Cartilage damage can
result in minor fibrillation that does
not result in full-thickness loss.
(B) However, in severe cases,
cartilage loss can extend to the
subchondral bone. The white arrows
highlight cartilage fibrillation.
the factors associated with progression of disease within affected stifle joints. However, one
important clue derives from studies showing
that arthroscopically assessed synovitis and
radiographic arthritis are correlated in both
unstable and contralateral stifle joints of dogs
with naturally occurring CR (Bleedorn et al.
2011), suggesting that synovitis is a key feature
of early disease. Ultimately, further studies are
required to understand the natural history of
CR. For further information regarding the role
of synovitis in cruciate ligament rupture pathology, see Chapter 12.
Progression of osteoarthritis after stifle
stabilization procedures
It is now well established that OA progresses
in the face of stifle stabilization procedures.
Numerous studies have documented this progression (Table 37.1). Currently there is no
standardized method by which radiographic
OA is quantified in the stifle joint. In the
reported literature, methods for measurement
of radiographic OA, times to follow up evaluation, and use of meniscal release concurrently
with stabilization, are highly variable between
studies.
Cause of osteoarthritis progression after
stifle stabilization procedures
The cause of OA progression after stifle stabilization surgery is likely multifactorial. Theories presented within the literature include continued stifle instability and altered joint contact
VetBooks.ir
Progression of Osteoarthritis after Stifle Stabilization Surgery
309
Table 37.1 Summary of studies reporting radiographic progression of osteoarthritis (OA) after surgical stabilization of
the stifle.
Author(s)
Elkins et al.
(1991)
Number
of dogs
15
17
Surgical
technique
Time to follow-up
(mean)
OA progression from
time of surgery
Intra-articular
stabilization
Extracapsular
stabilization
2–96 months (26)∗
100% of dogs with follow up
>6 months had OA
progression
Vasseur & Berry
(1992)
21
Intra-articular
stabilization
1–46 months (14.8)
100% of dogs had OA
progression
Innes et al.
(2004)
45
Intra-articular
stabilization
7 months
Significantly increased
osteophyte score
Significantly increased
global OA score
13 months
Rayward et al.
(2004)
40
TPLO
6 months
40% of dogs had OA
progression
Lazar et al.
(2005)
44
22
TPLO
Extracapsular
stabilization
≥12 months
OA significantly increased
with both techniques.
Boyd et al.
(2007)
29
TPLO
≥12 months
76% of dogs had OA
progression
Hurley et al.
(2007)
295
TPLO
2 months
OA significantly increased
Cook et al.
(2010)
23
24
TPLO
Extracapsular
(TightRope)
6 months
OA progression not
significant but noted to
progress over time
Au et al. (2010)
16
14
TPLO
Extracapsular
stabilization
24 months
OA significantly increased
for both techniques
Morgan et al.
(2010)
35
TTA
4–16 months (5.9)
55% of dogs had OA
progression
DeLuke et al.
(2012)
60
TPLO
12–36 months
100% of dogs had OA
progression
MacDonald et al.
(2013)
24
TTA
Each dog evaluated
at 0.5, 6, and 12
months
OA significantly increased at
all time points
Berger et al.
(2015)
15
TPLO
15
Extracapsular
stabilization
14–43.3 months
(29.4)
6.3–23.7 months
(15)
Mild OA progression for
both techniques
(significance not reported)
∗ Each
dog had between one and four follow-up time points.
TPLO, tibial plateau leveling osteotomy; TTA, tibial tuberosity advancement.
mechanics resulting from both the stabilization method and potential meniscal removal or
release (Kim et al. 2009a; Kim et al. 2009b; Tonks
et al. 2010; Pozzi et al. 2010a; Pozzi et al. 2010b).
Meniscal release, meniscal tearing, and meniscectomy are known to result in the development
of OA in experimental dogs with intact cruciate ligaments (Cox & Cordell 1977; Luther et al.
2009). While these factors appear to be influential in the continued progression of OA, extrapolation of results from studies of contralateral
stable stifles with early disease suggest that
VetBooks.ir
310
Surgical Treatment
continued synovitis is also a likely contributor
to postoperative OA progression.
Comparison of osteoarthritis progression
between stabilization methods
Currently, few studies have been reported in
the veterinary literature that have compared
progression of OA between various stabilization methods with a strict follow-up timeframe.
Most studies have highly variable ranges from
the time of surgery to follow-up. Cook et al.
(2010) reported OA progression at 6 months
after TPLO surgery and the TightRope extracapsular technique, noting that while OA
progressed with both methods, the progression
was not significantly different between stabilization methods or between time of surgery
and the 6-month recheck. Lazar et al. (2005)
also evaluated OA progression between TPLO
and an extracapsular stabilization technique,
with follow-up within 1 year of surgery. OA
progression was noted with both stabilization
methods, although dogs with a more severe OA
progression were more likely to have undergone an extracapsular stabilization method
rather than a TPLO.
Conclusions
Over the past few years, strong evidence
regarding the relationship between OA and
development of stifle instability in the stifle
joint of dogs has indicated that development of
radiographic OA precedes clinically detectable
joint instability from CR. This suggests that OA
is not only a result of stifle instability and altered
contact mechanics, but is also related to the
joint inflammation that contributes to cruciate
ligament fiber rupture and matrix degeneration. Stabilization procedures are not diseasemodifying, as these procedures do not directly
address the inflammatory environment within
CR stifle joints. Stifle synovitis should be considered a contributing factor in OA progression
over time, and a focus of future research.
References
Adams ME, Brandt KD. Hypertrophic repair of
canine articular cartilage in osteoarthritis after
anterior cruciate ligament transection. J Rheumatol
1991;18:428–435.
Au KK, Gordon-Evans WJ, Dunning D, et al. Comparison of short- and long-term function and radiographic osteoarthrosis in dogs after postoperative
physical rehabilitation and tibial plateau leveling
osteotomy or lateral fabellar suture stabilization.
Vet Surg 2010;39:173–180.
Berger B, Knebel J, Steigmeier-Raith S, et al. Longterm outcome after surgical treatment of cranial
cruciate ligament rupture in small breed dogs.
Tierärztl Prax (K) 2015;43:373–380.
Bleedorn JA, Greuel EN, Manley PA, et al. Synovitis in
dogs with stable stifle joints and incipient cranial
cruciate ligament rupture: a cross-sectional study.
Vet Surg 2011;40:531–543.
Boyd DJ, Miller CW, Etue SM, et al. Radiographic
and functional evaluation of dogs at least 1 year
after tibial plateau leveling osteotomy. Can Vet J
2007;48:392–396.
Brandt KD, Myers SL, Burr D, et al. Osteoarthritic
changes in canine articular cartilage, subchondral
bone, and synovium fifty-four months after transection of the anterior cruciate ligament. Arthritis
Rheum 1991;34:1560–1570.
Chuang C, Ramaker MA, Kaur S, et al. Radiographic
risk factors for contralateral rupture in dogs with
unilateral cranial cruciate ligament rupture. PLoS
One 2014;9:e106389.
Cook JL, Luther JK, Beetem J, et al. Clinical comparison of a novel extracapsular stabilization procedure and tibial plateau leveling osteotomy for
treatment of cranial cruciate ligament deficiency in
dogs. Vet Surg 2010;39:315–323.
Cox JS, Cordell LD. The degenerative effects of
medial meniscus tears in dogs’ knees. Clin Orthop
Relat Res 1977;125:236-242.
de Bruin T, de Rooster H, Bosmans T, et al.
Radiographic assessment of the progression of
osteoarthrosis in the contralateral stifle joint of
dogs with a ruptured cranial cruciate ligament. Vet
Rec 2007;161:745–750.
DeLuke AM, Allen DA, Wilson ER, et al. Comparison of radiographic osteoarthritis scores in dogs
less than 24 months or greater than 24 months following tibial plateau leveling osteotomy. Can Vet J
2012;53:1095–1099.
Doverspike M, Vasseur PB, Harb MF, et al. Contralateral cranial cruciate ligament rupture: incidence in
114 dogs. J Am Anim Hosp Assoc 1993;29:167–170.
Elkins AD, Pechman R, Karney MT, et al. A retrospective study evaluating the degree of degenerative
joint disease in the stifle joint of dogs following surgical repair of anterior cruciate ligament rupture. J
Am Anim Hosp Assoc 1991;27:533–540.
Fernandes JC, Martel-Pelletier J, Lascau-Coman V,
et al. Collagenase-1 and collagenase-3 synthesis
in normal and early experimental osteoarthritic
canine cartilage: an immunohistochemical study.
J Rheumatol 1998;25:1585–1594.
VetBooks.ir
Progression of Osteoarthritis after Stifle Stabilization Surgery
Hurley CR, Hammer DL, Shott S. Progression of
radiographic evidence of osteoarthritis following tibial plateau leveling osteotomy in dogs
with cranial cruciate ligament rupture: 295 cases
(2001–2005). J Am Vet Med Assoc 2007;230:1674–
1679.
Innes JF, Costello M, Barr FJ, et al. Radiographic
progression of osteoarthritis of the canine stifle
joint: a prospective study. Vet Radiol Ultrasound
2004;45:143–148.
Innes JF, Little CB, Hughes CE, et al. Products resulting from cleavage of the interglobular domain of
aggrecan in samples of synovial fluid collected
from dogs with early- and late-stage osteoarthritis.
Am J Vet Res 2005;66:1679–1685.
Kim SE, Pozzi A, Banks SA, et al. Effect of tibial
plateau leveling osteotomy on femorotibial contact
mechanics and stifle kinematics. Vet Surg 2009a;38:
23–32.
Kim SE, Pozzi A, Banks SA, et al. Effect of tibial
tuberosity advancement on femorotibial contact
mechanics and stifle kinematics. Vet Surg 2009b;38:
33–39.
Lazar TP, Berry CR, de Haan JJ, et al. Long-term
radiographic comparison of tibial plateau leveling osteotomy versus extracapsular stabilization
for cranial cruciate ligament rupture in the dog. Vet
Surg 2005;34:133–141.
Luther JK, Cook CR, Cook JL. Meniscal release in cruciate ligament intact stifles causes lameness and
medial compartment cartilage pathology in dogs
311
12 weeks postoperatively. Vet Surg 2009;38:520–
529.
MacDonald TL, Allen DA, Monteith GJ. Clinical
assessment following tibial tuberosity advancement in 28 stifles at 6 months and 1 year after
surgery. Can Vet J 2013;54:249–254.
Morgan JP, Voss K, Damur DM, et al. Correlation of radiographic changes after tibial
tuberosity advancement in dogs with cranial
cruciate-deficient stifles with functional outcome.
Vet Surg 2010;39:425–432.
Pozzi A, Kim SE, Lewis DD. Effect of transection
of the caudal menisco-tibial ligament on medial
femorotibial contact mechanics. Vet Surg 2010a;39:
489–495.
Pozzi A, Tonks CA, Ling HY. Femorotibial contact
mechanics and meniscal strain after serial meniscectomy. Vet Surg 2010b;39:482–488.
Rayward RM, Thomson DG, Davies JV, et al. Progression of osteoarthritis following TPLO surgery:
a prospective radiographic study of 40 dogs. J Small
Anim Pract 2004;45:92–97.
Tonks CA, Pozzi A, Ling HY, et al. The effects of extraarticular suture tension on contact mechanics of
the lateral compartment of cadaveric stifles treated
with the TightRope CCL® or lateral suture technique. Vet Surg 2010;39:343–349.
Vasseur PB, Berry CR. Progression of stifle
osteoarthrosis following reconstruction of the
cranial cruciate ligament in 21 dogs. J Am Anim
Hosp Assoc 1992;28:129–136.
VetBooks.ir
VetBooks.ir
38
Clinical Outcomes after
Surgical Treatment of Cruciate
Ligament Rupture
Mary Sarah Bergh and Steven C. Budsberg
Introduction
Surgical therapy has been recommended as the
optimal treatment to manage pain, discomfort,
and stifle instability secondary to canine cruciate ligament rupture (CR), due to the belief
that it will provide a provide a more rapid
return to function of the limb as compared
to non-surgical management. Interestingly, relatively limited data are available to support
this idea (Pond & Campbell 1972; Vasseur 1984;
Wurcherer et al. 2013). Wucherer and coworkers prospectively documented that dogs undergoing tibial plateau leveling osteotomy (TPLO)
had improved subjective and objective outcome scores compared to dogs undergoing nonsurgical management (weight loss, physiotherapy, and pain management with nonsteroidal
anti-inflammatory drugs) at 24 and 52 weeks
after surgery. Their surgical group had a higher
probability of a successful outcome at the 12-,
24-, and 52-week evaluation time points.
While hundreds of studies have been published describing various surgical procedures
to treat CR in dogs, relatively few report clinical outcomes for naturally occurring disease,
and even fewer compare surgical therapies or
compare a surgical treatment to non-surgical
treatment (Bergh et al. 2014). At the present
time, the most commonly performed surgical procedures, including TPLO, lateral extracapsular suture stabilization (LS), and tibial
tuberosity advancement (TTA), are all reported
to improve clinical function in dogs postoperatively (Slocum & Slocum 1993; Lafaver et al.
2007; Voss et al. 2008; Gordon-Evans et al.
2013; Duerr et al. 2014). A clear consensus
on the amount of clinical improvement with
each procedure is difficult to ascertain because
study designs, follow-up time frame and outcome assessment methods are highly variable
between studies. From an evidence-based perspective, the most useful data are generated
from prospective, randomized blinded clinical
trials, utilizing objective (i.e., kinetic or kinematic gait analysis) or validated subjective outcome data. Unfortunately, these types of study
are scarce in veterinary medicine.
Early postoperative clinical outcomes
(<6 months)
Most studies report an initial decrease in limb
function, followed by a progressive increase
in limb function, which generally plateaus
around 6 months after surgery, regardless of the
surgical procedure employed (Au et al. 2010;
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
313
Surgical Treatment
Gordon-Evans et al. 2013; MacDonald et al. 2013;
Nelson et al. 2013; Krotscheck et al. 2016). There
is conflicting evidence whether TTA results in
less lameness than the TPLO or LS in the early
postoperative period (<6 weeks) (Ferreira et al.
2016; Krotscheck et al. 2016).
Mid- and long-term clinical outcomes
(>6 months)
A contemporary systematic review evaluated
the scientific evidence on clinical outcomes for
all surgical procedures with at least 6 months
postoperative follow-up, published through
September 2013, to determine if there was evidence to support whether one or more surgical
procedures consistently return a dog to normal
clinical function (Bergh et al. 2014). While there
were relatively few studies that met the inclusion criteria, many of them offered high-quality
evidence and, therefore, allowed assessments
of some procedures to be made. Although the
data were not homogeneous, the strength of the
evidence evaluated strongly supported the ability of the TPLO to allow dogs to regain normal function postoperatively. In addition, the
evidence supported a superior clinical outcome
after TPLO as compared to LS (Gordon-Evans
et al. 2013; Berger et al. 2015) (Figure 38.1).
A recent prospective clinical trial comparing TTA, TPLO, LS, and normal dogs using
force plate analysis at a walk and trot at 2 and
8 weeks, and 6 and 12 months postoperatively,
was reported (Krotscheck et al. 2016). The TPLO
group gained normal limb use at the 6- and
12-month time points at both a walk and trot,
whereas the TTA regained normal function only
at a walk at the 12-month time point. The LS
group did not regain normal function at the
walk or trot at any time point (Figure 38.2).
Very few studies have reported clinical outcomes at greater than 1 year after surgery.
However, data suggest that clinical benefits
of surgery persist. Longer-term postoperative
follow-up is important, as surgical procedures
may have either positive or negative long-term
effects on joint biology and biomechanics, and
outcomes may be significantly different than in
the short or intermediate postoperative period.
Mölsä and colleagues (2014) found that a combined group of osteotomy techniques (TPLO,
TTA, triple tibial osteotomy), but not intraarticular repair techniques, allowed a return to
normal loading (peak vertical force; PVF) at a
minimum of 1.5 years (mean 2.8 years) after
surgery. Au et al. (2010) reported similar PVF
values for the LS and TPLO at 6 and 24 months
after surgery, suggesting that function does not
decline.
60
PVF(%BW)
50
40
LS
30
TPLO
20
10
on
th
s
m
12
6
m
on
th
s
ee
ks
w
ee
ks
w
6
12
e-
op
er
at
iv
e
0
Pr
VetBooks.ir
314
Figure 38.1 Canine pelvic limb use at the trot (mean peak vertical force (PVF) × % body weight) measured by a
pressure mat before and after unilateral lateral suture (LS) and tibial plateau leveling osteotomy (TPLO) in a prospective
randomized blinded clinical study. Asterisks indicate significant differences between groups. Data from Gordon-Evans
et al. 2013.
Clinical Outcomes after Surgical Treatment of Cruciate Ligament Rupture
315
VetBooks.ir
0.8
0.7
PVF(%BW)
0.6
0.5
Normal dogs
0.4
LS
0.3
TPLO
TTA
0.2
0.1
s
on
12
m
on
m
6
th
s
th
ks
ee
w
8
ks
ee
w
2
Pr
e-
op
er
at
iv
e
0
Figure 38.2 Canine pelvic limb use at the trot (mean peak vertical force (PVF) × % body weight) measured by dual
force plates in normal dogs and before and after unilateral lateral suture (LS), tibial plateau leveling osteotomy (TPLO),
and tibial tuberosity advancement (TTA) in prospective clinical studies. The black boxes indicate a lack of significant
difference between values. Data from Nelson et al. 2013 and Krotscheck et al. 2016.
Factors affecting clinical outcome
Patient, owner, and surgeon factors may affect
clinical outcome. Currently, the evidence supports similar clinical outcomes for small-, large-,
and giant-breed dogs after LS and TPLO
(Gordon-Evans et al. 2013; Nelson et al. 2013;
Berger et al. 2015). Postoperative TTA complications decrease PVF, although with appropriate treatment PVF returns to a level similar to
dogs without complications (Voss et al. 2008).
Data suggest that the method of joint exploration (arthrotomy versus arthroscopy) and
meniscal treatment do not affect the speed or
extent of recovery in naturally occurring canine
CR (Thieman et al. 2006; Nelson et al. 2013).
However, arthroscopic evaluation does provide
improved examination of the menisci, which
may potentially affect outcome, as failure to
identify a meniscal tear at the time of initial
surgery leads to lameness in the postoperative
period (Thieman et al. 2006; Pozzi et al. 2008).
Stifle osteoarthritis is progressive regardless
of treatment, though the severity of osteoarthritis is not reported to affect clinical function in
dogs (Au et al. 2010; MacDonald et al. 2013;
Berger et al. 2015). However, in the intermediate
or long term, progressive osteoarthritis and
periarticular fibrosis may account for the
observed reduction in stifle range of motion
after some techniques (MacDonald et al. 2013;
Mölsä et al. 2014). Physical rehabilitation
improves the speed and extent of recovery
in the early postoperative time period, and
some evidence suggests that there may also be
long-term benefits (Au et al. 2010; Romano &
Cook 2015).
Conclusions
Scientific evidence supports an improvement in
clinical function after surgical therapy for CR
in dogs. However, not all surgical procedures
offer an equivalent level of recovery. At the current time, the best available evidence provides
strong support that TPLO allows dogs to regain
normal clinical function. The evidence suggests
that the clinical outcome after TPLO is superior to the LS and TTA. Data do not support the
ability of the TTA to consistently allow dogs to
return to normal clinical function. Longer-term
studies are necessary to evaluate clinical function following all surgical procedures.
VetBooks.ir
316
Surgical Treatment
References
Au KK, Gordon-Evans WJ, Dunning D et al. Comparison of short- and long-term function and radiographic osteoarthrosis in dogs after postoperative
physical rehabilitation and tibial plateau leveling
osteotomy or lateral fabellar suture stabilization.
Vet Surg 2010;39:173–180.
Berger B, Knebel J, Steigmeier-Raith S, et al. Longterm outcome after surgical treatment of cranial
cruciate ligament rupture in small breed dogs.
Comparison of tibial plateau leveling osteotomy
and extra-articular stifle stabilization. Tierarztl
Prax Ausg K Kleintiere Heimtiere 2015;43:373–380.
Bergh MS, Sullivan C, Ferrell CL, et al. Systematic
review of surgical treatments for cranial cruciate
ligament disease in dogs. J Am Anim Hosp Assoc
2014;50:315–321.
Duerr FM, Martin KW, Rishniw M, et al. Treatment
of canine cranial cruciate ligament disease. A survey of ACVS Diplomates and primary care veterinarians. Comp Orthop Traumatol 2014;27:478–
483.
Ferreira MP, Ferrigno CR, de Souza AN, et al. Shortterm comparison of tibial tuberosity advancement
and tibial plateau levelling osteotomy in dogs with
cranial cruciate ligament disease using kinetic analysis. Vet Comp Orthop Traumatol 2016;29:209–213.
Gordon-Evans WJ, Griffon DJ, Bubb C, et al. Comparison of lateral fabellar suture and tibial plateau leveling osteotomy techniques for treatment of dogs
with cranial cruciate ligament disease. J Am Vet
Med Assoc 2013;243:675–680.
Krotscheck U, Nelson SA, Todhunter RJ, et al.
Long term functional outcome of tibial tuberosity
advancement vs. tibial plateau leveling osteotomy
and extracapsular repair in a heterogeneous population of dogs. Vet Surg 2016;45:261–268.
Lafaver S, Miller NA, Stubbs WP, et al. Tibial tuberosity advancement for stabilization of the canine cranial cruciate ligament-deficient stifle joint: surgical
technique, early results, and complications in 101
dogs. Vet Surg 2007;36:573–586.
MacDonald TL, Allen DA, Monteith GJ. Clinical assessment following tibial tuberosity
advancement in 28 stifles at 6 months and 1
year after surgery. Can Vet J 2013;54:249–254.
Mölsä SH, Hyytiäinen HK, Hielm-Björkman AK, et al.
Long-term functional outcome after surgical repair
of cranial cruciate ligament disease in dogs. BMC
Vet Res 2014;10:266–276.
Nelson SA, Krotscheck U, Rawlinson J, et al. Longterm functional outcome of tibial plateau leveling
osteotomy versus extracapsular repair in a heterogeneous population of dogs. Vet Surg 2013;42:38–
50.
Pond MJ, Campbell JR. The canine stifle joint I.
Rupture of the anterior cruciate ligament: an
assessment of conservative and surgical treatment.
J Small Anim Pract 1972;13:1–10.
Pozzi A, Hildreth BE 3rd, Rajala-Schultz PJ. Comparison of arthroscopy and arthrotomy for diagnosis
of medial meniscal pathology: an ex vivo study. Vet
Surg 2008;37(8):749–755.
Romano LS, Cook JL. Safety and functional outcomes
associated with short-term rehabilitation therapy
in the post-operative management of tibial plateau
leveling osteotomy. Can Vet J 2015;56:942–946.
Slocum B, Slocum TD. Tibial plateau leveling
osteotomy for repair of cranial cruciate ligament
rupture in the canine. Vet Clin North Am Small
Anim Pract 1993;23:777–795.
Thieman KM, Tomlinson JL, Fox DB, et al. Effect of
meniscal release on rate of subsequent meniscal
tears and owner-assessed outcome in dogs with
cruciate disease treated with tibial plateau leveling
osteotomy. Vet Surg 2006;35:705–710.
Vasseur PB. Clinical results following nonoperative
management for rupture of the cranial cruciate ligament in dogs. Vet Surg 1984;13:243–246.
Voss K, Damur DM, Guerrero T, et al. Force plate
gait analysis to assess limb function after tibial
tuberosity advancement in dogs with cranial cruciate ligament disease. Vet Comp Orthop Traumatol
2008;21:243–249.
Wucherer KL, Conzemius MG, Evans R, et al. Shortterm and long-term outcomes for overweight dogs
with cranial cruciate ligament rupture treated surgically or nonsurgically. J Am Vet Med Assoc
2013;242:1364–1372.
VetBooks.ir
39
Success and Failure after Stifle
Stabilization Surgery
Michael G. Conzemius and Richard B. Evans
Introduction
Balanced and concurrent consideration of success and failure after stifle surgery should be
used to define and explain how ‘successful’
a procedure is. To accomplish this, investigators must: (i) understand how to calculate and
report the successes and failures; (ii) carefully
choose the outcome measure(s) used to measure success (e.g., owner survey, gait analysis)
and failure (e.g., second surgery); and (iii) evaluate and report data in a clinically meaningful
manner. All of this discussion is relative to time
after the intervention. Other factors, such as age,
breed, surgeon experience, owner’s input, can
also influence outcomes.
Balancing success and failure
Since surgery is a comparatively invasive intervention that has inherent risks to the patient,
it is most reasonable to consider the advantages and disadvantages concurrently when
discussing and reporting techniques. Although
there may be disagreement regarding the exact
mathematical method that should be used to
report advantages and disadvantages of an
intervention, the concept remains the same;
benefits and risks associated with an intervention need to be evaluated together. The Number
Needed to Treat (NNT) is the number of subjects
that need to be treated to prevent one additional
bad outcome (e.g., limping). If an intervention
has a NNT of 6, it means that six patients
must be treated with that intervention before
one additional bad outcome (e.g., lameness) is
prevented relative to the control group. A NNT
of 1 would suggest that every patient treated
with an intervention improves, and none in the
control group improve. A NNT of 10 would
suggest a high placebo effect. Absolute Risk
Reduction (ARR; arithmetic difference between
groups) is the change in the risk of an outcome,
and is the inverse of NNT (Hutton 2009).
Alternatively, the Relative Risk Reduction (RRR;
proportional difference between groups) can be
calculated.
The likelihood of an adverse event or treatment failure is just as important to the patient
and client as the probability of success. The
Number Needed to Harm (NNH) is the number of
patients that had an adverse event (e.g., implant
removal) because of the intervention that would
not have been exposed to the adverse event if
there were in the control group. A NNH of 1
suggests that 100% of treated patients had an
adverse event, and they would not have that
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
317
VetBooks.ir
318
Surgical Treatment
adverse event if they were in the control group.
Similarly, Absolute Risk Increase (ARI) can be
calculated.
To calculate NNT and NNH, it is necessary to choose a specific outcome measure at a
specific time point. For example, if success at
1 year after surgery is defined as at least a 25%
improvement from a validated owner survey
and no residual lameness via visual inspection
12 months after surgery, failure will be defined
as the need for a second surgery. For the control
group it can be conservatively estimated that
with non-surgical management of large-breed,
obese dogs with cruciate ligament rupture (CR),
50% of dogs will have a successful outcome
and 0% of dogs would require a second surgery
(Wucherer et al. 2013). For tibial plateau leveling
osteotomy (TPLO) it is estimated that 90% have
a successful outcome (owner reports improvement plus no visual lameness) and 10% have
failure (e.g., second surgery needed to remove
bone plate). The present authors used 10%
based on unpublished data from their hospital,
where it was found that over a 5-year period
9% of patients that had a TPLO plate applied
underwent a second surgery where the TPLO
plate was removed. For comparison, only 80%
of dogs that have an extracapsular suture placed
have a successful outcome, and 5% require a
second surgery. Using these estimates of success and failure, it can be learned that both procedures provide a good treatment advantage
over non-surgical management and TPLO provides greater benefits (Table 39.1). However, if
the relationship between NNT and NNH (a low
number is good) is reviewed, a conclusion that
TPLO is much better than a suture surgery after
examining only NNT is an incomplete interpretation, as the risks of TPLO are greater than for
a suture surgery.
Owner questionnaires
Establishing the owner’s perspective on outcome remains important since they spend
the most time with their pet. Historically,
manuscripts have documented that owners
reported that their pet had a ‘good or excellent’ outcome 88.5–93% of the time after surgery
(Hoffmann et al. 2006; Corr & Brown 2007;
Stein & Schmoekel 2008). These findings, however, must be interpreted with great caution
because of differences in the questions asked,
the method of questionnaire delivery (mail,
telephone, or personnel interview) and other
biases that significantly influence owner reporting. It is also important to note the duration
of follow-up after surgery, since it has been
reported that outcomes worsen with increased
time after surgery (Innes et al. 2000). To best
interpret and compare studies, the consistent
use of a validated owner questionnaire should
be considered. Several validated owner questionnaires addressing patient pain, function,
quality of life, and/or activity have been created. The Canine Brief Pain Inventory (CBPI)
for dogs with osteoarthritis (OA) provides reasonable evidence that owner questionnaires can
be effectively used in clinical research (Brown
et al. 2008). The Liverpool Osteoarthritis in Dogs
(LOAD) instrument has been critically evaluated and successfully used in several clinical
investigations (Walton et al. 2013; Lascelles et al.
2015). The Client-Specific Outcome Measures
(CSOM) has also been evaluated and used in
clinical research (Rialland et al. 2012).
While each of these questionnaires will
effectively standardize the questions and allow
for some comparison across studies, results in
studies with small to modest patient enrollment
numbers should be interpreted with caution
Table 39.1 An example of how NNT and NNH can be used for a balanced approach to compare different interventions.
Success
rate (%)
NNT
1/Tx-control
(control = 50%)
Major complication
(2nd surgery) (%)
NNH
1/%
complication
NNT/NNH
TPLO
90
2.5
10
10
0.25
Extracapsular suture
stabilization
80
3.33
5
20
0.167
NNT, Number Needed to Treat; NNH, Number Needed to Harm; TPLO, tibial plateau leveling osteotomy.
VetBooks.ir
Success and Failure after Stifle Stabilization Surgery
because of low statistical power. Inconsistencies
in delivery and interpretation of the questionnaire results in sizeable variabilities that can
only be overcome by employing large study
populations. In addition, it is necessary to be
cognizant of the caregiver placebo effect that
undoubtedly influences responses from owners
and other caregivers (Conzemius & Evans
2012).
Veterinary examination
Before surgery, a clinician may assign a subjective score to limb function based on assessment
of dog’s level of pain, lameness, and posture
while sitting. While each clinician differs to
some degree, observations when the patient
is walking and/or trotting may include a dip
in the patient’s hip or head, degree of limb
carriage, and stride length. During physical
examination the clinician may note the joint’s
range of motion, the amount of muscle mass,
and even if the leg is positioned ‘normally’
when sitting. All of these can contribute to a
determination of the patient’s quality of limb
function. Documentation of findings are generally recorded via a numeric rating score (NRS),
where numbers are assigned to each finding,
or via a visual analog scale (VAS) where limb
function is assigned by marking a line with one
end of the line representing ‘clinically normal’
(sound) and the other end representing ‘could
not be more lame’ (i.e., non weight-bearing)
(Waxman et al. 2008). The NRS is limited
because there are a restricted number of groups
(four or five) within a classification, and dogs
within a group can have appreciable differences
in their lameness severity (Waxman et al. 2008).
A VAS does not have this limitation because it
provides a continuous scale that may be easier
to handle statistically. Regardless, both schemes
provide only the opinion of the observer. Several manuscripts have tried to offset these
limitations by including multiple, trained
observers. Unfortunately, in one publication
which tried to validate clinician observation of
gait, neither trained nor untrained observers
could reliably identify lameness. There were
large disagreements between individuals.
Untrained observers (first-semester veterinary
students) had the same visual acuity for dog
319
lameness as boarded surgeons (Waxman et al.
2008). The only saving grace was a finding that
trained clinicians provided repeatable data;
that is, they consistently made the same mistake. This would allow a clinician to compare
groups over time, but not necessarily to comment on the success or failure of an individual
dog.
Pedometers and accelerometers
The greatest limitation to data collected at a veterinary hospital is that it measures a moment
in time, and not the day-to-day activity of the
dog at home. A pedometer or accelerometer can
measure patient activity level at home over an
extended period of time. In one study, pedometers were successfully used to measure physical
activity in dogs over a 14-day period (Chan et al.
2005). The pedometer accuracy varied depending on the patient’s size (it overestimated walking in large dogs and underestimated walking
in small dogs), but correlated well with overall reports of the dog’s activity level at home
and the dog’s condition body score. Accelerometers are more sophisticated in that some can
measure changes in acceleration in the x-, y-,
and z- axes. Thus, body movement in any direction is measured. In one study that determined
variability in accelerometer data in companion
dogs, large day-to-day, and even week-to-week,
variations occurred in dogs, but within dogs, a
full 7-day comparison of total activity counts
from one week to the next provided the least
variable estimate of the dogs’ activity (Dow et al.
2009). It was also reported that accelerometers
might be most useful for documenting changes
in the dog’s activity over time.
While pedometers and accelerometers estimate patient activity, to date, there is little information available as to whether such data can be
translated to something clinically relevant, such
as distance traveled and/or activity intensity.
For example, it may currently be found that a
patient had an increase in accelerometer counts
of 20%, but what exactly does that mean? In
the present authors’ opinion, if this meant that
the dog was willing to travel 20% more distance or performed 20% more intense activities
(e.g., stairs, jumping), it would much more
beneficial.
VetBooks.ir
320
Surgical Treatment
Force platform gait analysis
Force platform gait analysis provides an objective, sensitive method to measure gait. It has
been used extensively to compare forces before
and after surgical treatment of CR in clinical
patients (Budsberg et al. 1988; Dupuis et al. 1994;
DeCamp et al. 1996; Jevens et al. 1996; Marsolais
et al. 2003; Conzemius et al. 2005), and is recognized by many as the ‘gold standard’ outcome
measure for orthopaedic conditions such as CR.
However, computational gait analysis is useful
only if cases are carefully selected, the gait analysis is precisely performed, and the collected
data are correctly analyzed (Evans et al. 2003;
Evans et al. 2005).
Pressure platform gait analysis can also be
used and has specific advantages and disadvantages that are relevant to clinical research.
Tek-scan’s Industrial Sensing pressure measurement system has been compared to traditional force platform gait analysis, and the data
are comparable (Besancon et al. 2003). However,
the data are not interchangeable because pressure mats consistently underestimate vertical
forces; thus, studies should choose one method
or the other. This system has been used successfully to evaluate limb function in dogs after
surgical treatment of CR (Horstman et al. 2004).
A final alternative is to use the pressure-sensing
mat GAIT4Dog® . These mats do not report pad
pressures or ground reaction forces, which limits validation techniques, but rather report relationships between limbs, such as asymmetry.
Their long length allows for the rapid collection
of data and their integration into treadmills is
unique.
Reporting data in a clinically
meaningful manner
Many investigators including the present
authors have limited the usefulness of their
data by only reporting group means and pvalues. If it is reported that the peak vertical
force is 40.0 for group A and 38.0 for group
B, and the P-value is 0.04, then clearly group
A and B are different. If Group A and B have
undergone different surgical procedures, then
this result tells us very little clinically. What
owners and veterinarians need to know is
how a difference impacts the outcome for an
individual dog, what is the size of the difference, and is it clinically significant? Although
these topics extend beyond the scope of this
chapter, investigators should consider reporting probability, such as probability of normal
function (Conzemius et al. 2005), effect sizes of
group differences, and then consider clinical
significance from these results.
Additional considerations regarding
residual lameness
Three additional potential contributors to residual lameness in a dog after CR stifle stabilization surgery are the development of complications, the progression of OA, and instability.
While many complications are avoidable, their
exclusion is impossible. Complication rates
have been reported for many studies, and their
relative frequency between various stabilization techniques estimated by some authors. A
clear definition of the timing and severity of
a complication has been described and should
be used for consistency (Cook et al. 2010). As
discussed above, complications need to be considered with successes. For example, Voss et al.
(2008) used force platform gait analysis to determine outcome in dogs after tibial tuberosity
advancement, and reported that while most
dogs returned to a function that was 90% of the
normal dogs studied, 25% of the cases had a
complication and these dogs had ground reaction forces (GRFs) that were significantly lower
than when no complication occurred (Voss et al.
2008).
OA development and progression is
inevitable regardless of the surgical technique used. While the severity of stifle OA
is not correlated to the severity of lameness
(Gordon et al. 2003), it seems likely that dogs
with OA have a greater probability of lameness
as compared to their counterparts. Much of this
assertion could be related to the limitations of
plain radiographs. Magnetic resonance imaging (MRI), using dGEMRIC or T2 mapping, can
generate objective information regarding the
health of the cartilage, is related to OA progression and patient prognosis (Cunningham et al.
2006; Welsch et al. 2009), and has been described
in the dog (Wucherer et al. 2012). One aspect
of stifle surgery that some surgeons consider
routine is medial meniscus release, which aims
Figure 39.1 Graph showing vertical impulse
(VI; % body weight) of dogs before
arthroscopic surgery and at 2 and 6 months
after surgery. In a group of dogs with cruciate
ligament rupture and a medial meniscal tear,
dogs treated with only arthroscopic
debridement of the ruptured cranial cruciate
ligament and medial meniscus were
compared with dogs that received
arthroscopic debridement together with tibial
plateau leveling osteotomy (TPLO).
VI (% bw)
VetBooks.ir
Success and Failure after Stifle Stabilization Surgery
18
16
14
12
10
8
6
4
2
0
to reduce the risk of a medial meniscal tear after
surgery. One fact that surgeons should consider
is that release of the medial meniscal rapidly
causes OA and lameness within 12 weeks, even
in a stable stifle (Luther et al. 2009). In research
hounds, evidence of cartilage loss can be seen
grossly using India ink staining and via MRI T2
mapping. In addition, it should be accepted that
medial meniscal tears occur more commonly in
an unstable stifle as opposed to a stable stifle;
thus, if the stabilization procedure performed
requires a release of the medial meniscus than
it should be questioned as to how effective
it is at stabilizing the cruciate-deficient stifle
joint. Empirically, meniscal pathology and
OA are the greatest limits to outcome after
surgery for CR. This suggestion is supported
by a small study that evaluated dogs with
chronic lameness (>3 months) from surgical
treatment for CR, minimal instability, and a
medial meniscal tear (Conzemius 2007). In
this study, outcome was measured objectively
using GRFs in dogs that had either arthroscopic
debridement of the CrCL and medial meniscus
or arthroscopic debridement and TPLO stabilization; no differences were found between
groups (Figure 39.1).
For decades, veterinary surgeons have
debated which surgical procedure provides
the best outcome after treatment of CR. One
component of this is to establish that the procedure in question adequately stabilizes the
stifle. This is based on the assumption that the
degree of instability is related to the degree
of lameness. The term ‘assumption’ is used
because the evidence provided to date does not
state that instability is good, but does suggest
that it may not be all that bad. In one study
(Hill et al. 1999), dogs which had undergone
surgery more than 1 year previously were
321
TPLO + Scope
(n = 4)
Scope ( n = 4)
0
6
26
Time after Surgery (weeks)
allocated to groups based on owner interview,
as having either a satisfactory or unsatisfactory
outcome. Surprisingly, dogs in the satisfactory
outcome group had almost twice the amount of
instability and less than half the stifle pain on
physical examination.
Conclusions
Advances in understanding of how to interpret success and define outcome measures will
lead to continued improvement in clinical treatments. Whilst it appears that surgical management can improve lameness in most dogs with
CR, the unfortunate fact is that as yet no surgical procedure has been developed, whether
it includes stabilization or not, that eliminates
lameness.
References
Besancon MF, Conzemius MG, Derrick TR, et al. Comparison of vertical forces in normal dogs between
the AMTI Model OR6-5 force platform and the
Tekscan (industrial sensing pressure measurement
system) pressure walkway. Vet Comp Orthop Traumatol 2003;16:153–157.
Brown DC, Boston RC, Coyne JC, et al. Ability of the
canine brief pain inventory to detect response to
treatment in dogs with osteoarthritis. J Am Vet Med
Assoc 2008;233:1278–1283.
Budsberg SC, Verstraete MC, Soutas-Little RW, et al.
Force plate analyses before and after stabilization
of canine stifles for cruciate injury. Am J Vet Res
1988;49:1522–1524.
Chan CB, Spierenburg M, Ihle SL, et al. Use of
pedometers to measure physical activity in dogs.
J Am Vet Med Assoc 2005;226:2010–2015.
Cook JL, Evans R, Conzemius MG, et al. Proposed definitions and criteria for reporting time
frame, outcome, and complications for clinical
orthopaedic studies in veterinary medicine. Vet
Surg 2010;39:905–908.
VetBooks.ir
322
Surgical Treatment
Conzemius MG, Evans RB. Care giver placebo effect
in dogs with osteoarthritis. J Am Vet Med Assoc
2012;241:1314–1319.
Conzemius MG. RCCL Injury: The role of stabilization. Proceedings from the American College of
Veterinary Surgeons Annual Symposium, Chicago,
IL, 2007, p. 332.
Conzemius MG, Evans RJ, Besancon MF, et al. Effect
of surgical technique on limb function after surgery
for rupture of the cranial cruciate ligament in dogs.
J Am Vet Med Assoc 2005;226:232–239.
Corr SA, Brown C. A comparison of outcomes following tibial plateau leveling osteotomy and cranial tibial wedge osteotomy procedures. Vet Comp
Orthop Traumatol 2007;20:312–319.
Cunningham T, Jessel R, Zurakowski D, et al. Delayed
gadolinium-enhanced magnetic resonance imaging of cartilage to predict early failure of Bernese
periacetabular osteotomy for hip dysplasia. J Bone
Joint Surg 2006;88:1540–1548.
DeCamp CE, Riggs CM, Olivier NB, et al. Kinematic
evaluation of gait in dogs with cranial cruciate ligament rupture. Am J Vet Res 1996;57:120–126.
Dow C, Michel KE, Love M, et al. Evaluation of optimal sampling interval for activity monitoring in
companion dogs. Am J Vet Res 2009;70:444–448.
Dupuis J, Harari J, Papageorges M, et al. Evaluation of
fibular head transposition for repair of experimental cranial cruciate ligament injury in dogs. Vet Surg
1994;23:1–12.
Evans RB, Gordon W, Conzemius M. The effect of
velocity on ground reaction forces in dogs with
lameness attributable to tearing of the cranial cruciate ligament. Am J Vet Res 2003;64:1479–1481.
Evans R, Horstman C, Conzemius M. Accuracy and
optimization of force platform gait analysis in
Labradors with cranial cruciate disease evaluated
at the walking gait. Vet Surg 2005;34:445–449.
Gordon WJ, Conzemius MG, Riedesel E, et al.
The relationship between limb function and
radiographic osteoarthrosis in dogs with stifle
osteoarthrosis. Vet Surg 2003;32:451–454.
Hill CM, Conzemius MG, Smith GK, et al. Bacterial
culture of the canine stifle joint following surgical repair of ruptured cranial cruciate ligament. Vet
Comp Orthop Traumatol 1999;12:1–5.
Hoffmann DE, Miller JM, Ober CP, et al. Tibial
tuberosity advancement in 65 canine stifles. Vet
Comp Orthop Traumatol 2006;19:219–227.
Horstman CL, Conzemius MG, Evans R, et al. Assessing the efficacy of perioperative oral carprofen
after cranial cruciate surgery using noninvasive,
objective pressure platform gait analysis. Vet Surg
2004;33:286–289.
Hutton JL. Number needed to treat and number
needed to harm are not the best way to report and
assess the results of randomized clinical trials. Br J
Haematol 2009;146:27–30.
Innes JF, Bacon D, Lynch C, Pollard A. Long-term
outcome of surgery for dogs with cranial cruci-
ate ligament deficiency. Vet Record 2000;147:325–
328.
Jevens DJ, DeCamp CE, Hauptman J, et al. Use of
force-plate analysis of gait to compare two surgical techniques for treatment of cranial cruciate ligament rupture in dogs. Am J Vet Res 1996;57:389–
393.
Lascelles BD, Knazovicky D, Case B, et al. A caninespecific anti-nerve growth factor antibody alleviates pain and improves mobility and function
in dogs with degenerative joint disease-associated
pain. BMC Vet Res 2015;11:101.
Luther JK, Cook CR, Cook JL. Meniscal release in cruciate ligament intact stifles causes lameness and
medial compartment cartilage pathology in dogs
12 weeks postoperatively. Vet Surg 2009;38:520–
529.
Marsolais GS, McLean S, Derrick T, et al. Kinematic
analysis of the hind limb during swimming and
walking in healthy dogs and dogs with surgically
corrected cranial cruciate ligament rupture. J Am
Vet Med Assoc 2003;222:739–743.
Rialland P, Bichot S, Moreau M, et al. Clinical validity of outcome pain measures in naturally occurring canine osteoarthritis. BMC Vet Res 2012;8:162.
Stein S, Schmoekel H. Short-term and eight to 12
months results of a tibial tuberosity advancement
as treatment of canine cranial cruciate ligament
damage. J Small Anim Pract 2008;49:398–404.
Voss K, Damur DM, Guerrero T, et al. Force plate
gait analysis to assess limb function after tibial
tuberosity advancement in dogs with cranial cruciate ligament disease. Vet Comp Orthop Traumatol
2008;21:243–9.
Walton MB, Cowderoy E, Lascelles D, et al. Evaluation
of construct and criterion validity for the ‘Liverpool
Osteoarthritis in Dogs’ (LOAD) clinical metrology
instrument and comparison to two other instruments. PLoS One 2013;8:e58125.
Waxman AW, Robinson DA, Evans R, et al. Relationship between objective and subjective assessment
of limb function in normal dogs with an experimentally induced lameness. Vet Surg 2008;37:241–
246.
Welsch GH, Mamisch TC, Marlovits S, et al. Quantitiative T2 mapping during follow-up after matrixassociated autologous chondrocyte transplantation
(MCAT): Full-thickness and zonal evaluation to
visualize the maturation of cartilage repair tissue.
J Orthop Res 2009;27:957–963.
Wucherer KL, Ober C, Conzemius MG. The use of
delayed gadolinium enhanced magnetic resonance
imaging of cartilage and T2 mapping to evaluate
articular cartilage in the normal canine elbow. Vet
Rad Ultrasound 2012; 53:57–63.
Wucherer KL, Conzemius MG, Evans RB, et al. Shortterm and long-term outcomes for overweight dogs
with cranial cruciate ligament rupture treated surgically or nonsurgically. J Am Vet Med Assoc
2013:242:1364–1372.
VetBooks.ir
40
Diagnosis and Management
of Orthopaedic Infection
after Stifle Surgery
Noël M.M. Moens
Introduction
Since ancient times, surgical infections have
always been a challenge for surgeons. Although
significant discoveries have been made over
the past century, current understanding of surgical infections and widespread use of antibiotics have all but eliminated the risk of surgical site infection (Alexander 1985). Although
the risk of developing surgical infection and
the chances of dying from infection have substantially decreased, surgeons are now faced
with the increasing prevalence of multi-drugresistant bacteria (Cohen 1992). Infections that
are untreatable with the current range of antibiotics are becoming more frequent and cause a
significant burden on the patient’s well-being
and on the cost of healthcare.
The overall incidence of infection in human
surgery has been reported to be between 2% and
5%. However, incidence varies based on the specific surgery, specific risk factors, and wound
classification (Culver et al. 1991; Anderson 2011;
Eisenberg 2012). Clean elective orthopaedic
procedures have the lowest infection rates,
while contaminated or dirty procedures are
associated with higher rates. Although slightly
higher, the rate of surgical infection in veterinary surgery parallels the human surgery, with
infection rates for clean procedures reported
to be around 2.5% (Vasseur et al. 1992; Eugster et al. 2004). Over the past two decades,
several new procedures have been developed
for the treatment of various stifle conditions.
Although most are clean elective procedures,
higher infections rates than expected have often
been reported.
Definition
Surgical site infections (SSI) are infectious
complications that manifest at the incision site
of a surgical patient, and are the result of a combination of host, pathogen, and environmental
factors resulting in the establishment of infection (Mangram et al. 1999; Nelson 2011). In order
to standardize the definition of SSI, the United
States Centers for Disease Control and Prevention (CDC) has defined several categories of
SSI and has provided criteria for its diagnosis
(Table 40.1). It must be noted that although isolation and culture of the causal agent adds to the
validity of the diagnosis, a positive culture is not
required for the diagnosis of SSI. Some aspects
of the definition can still be open to interpretation and will continue to generate variability
in the results. For example, inflammation and
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
323
VetBooks.ir
324
Surgical Treatment
Table 40.1 Criteria for the definition of different categories of surgical site infection.
Category
Superficial SSI
Within 30 days of the operation. Involves only the skin and/or subcutaneous tissues.
Involves one or more of the following:
r Purulent discharge (with or without laboratory confirmation)
r Organism isolated from aseptically collected sample of fluid or tissue
r At least one of the following signs of infection: Pain or tenderness, localized swelling,
r
Deep SSI
redness or heat and superficial incision is deliberately opened by the surgeon unless
incision is culture-negative
Diagnosis of superficial incisional SSI made by a surgeon or attending clinician
Within 30 days of the operation if no implants or within 1 year if an implant is left in
place. Involves deep soft tissues (fascial or muscle layers).
Involves one or more of the following:
r Purulent discharge from deep incision but not from the organ/space component of the
surgical site
r A deep incision spontaneously dehisces or is deliberately opened by a surgeon when
r
r
r
Organ/Space SSI
the patient has at least one of the following clinical signs: Fever, localized pain or
tenderness, unless site is culture-negative
Organism isolated from aseptically collected sample of fluid or tissue.
An abscess or other evidence of infection involving the deep incision that is found on
direct examination, during reoperation, or by histopathologic or radiologic examination
Diagnosis of deep incisional SSI made by a surgeon or attending clinician
Within 30 days of the operation if no implants or within 1 year if an implant is left in
place. Involves any organ/space, other than the incision, that was opened or manipulated
during surgery.
Involves one or more of the following:
r Purulent drainage from a drain placed into the organ/space
r Organisms isolated from an aseptically obtained culture or fluid or tissue in the
organ/space
r An abscess or other evidence of infection involving the organ/space that is found on
direct examination, during reoperation, or by histopathologic or radiologic examination
r Diagnosis of organ/space SSI made by a surgeon or attending clinician
Note: Adapted from: CDC definitions for surgical site infections (Mangram et al. 1999).
incisional dehiscence has always been a diagnostic challenge. Whether the animal caused
the infection by opening the incision, or the
infection caused the animal to open the incision,
will always be a matter of debate and personal
interpretation.
Incidence of infection in stifle surgery
Because of the high prevalence of cruciate ligament rupture, and the popularity of tibial
plateau leveling osteotomy (TPLO), more studies have focused on this procedure than on
any other stifle procedure. Infection rates after
TPLO surgery vary greatly, and range between
2.5% and 15.8% (Pacchiana et al. 2003; Priddy
et al. 2003; Corr & Brown 2007; Fitzpatrick &
Solano 2010; Frey et al. 2010; Gatineau et al.
2011; Thompson et al. 2011; Gallagher & Mertens
2012; Dal-bó et al. 2013; Etter et al. 2013; Savicky et al. 2013; Nazarali et al. 2014). The actual
incidence is difficult to determine because few
studies use the standardized definition of infection, and even fewer are the result of active
surveillance. Most studies are retrospective in
nature and have not been designed to assess
infection rates. One prospective, multicenter
study with active surveillance for up to a year
reports an overall infection rate of 6.7% over 549
VetBooks.ir
Diagnosis and Management of Orthopaedic Infection after Stifle Surgery
procedures (Nazarali et al. 2015). These rates
seem to be fairly similar to most high tibial
osteotomy procedures.
Although much less has been published on
the other procedures, infection rates after tibial
tuberosity advancement (TTA) are very similar,
and rates between 2.6% and 12.5% have been
reported (Lafaver et al. 2007; Wolf et al. 2012;
Dal-bó et al. 2013; Proot & Corr 2013; Yap et al.
2015). Significantly higher infection rates have
been observed in a population of Boxer dogs
compared to non-Boxer dogs (22% versus 3.7%),
but the reasons remain unclear (de Lima Dantas
et al. 2015). Closing cranial wedge ostectomy has
published infection rates of between 8.3% and
16.6% (Corr & Brown 2007; Dal-bó et al. 2013).
Besides the treatment of cruciate ligament rupture, reported infection rates after patellar luxation repair range from 6.4% to 10% (Gibbons
et al. 2006; Clerfond et al. 2014; Kalff et al. 2014;
Shaver et al. 2014).
Extracapsular techniques for cruciate ligament stabilization have generally been associated with a lesser risk of infection. The largest
series of 363 cases of lateral fabellar suture
stabilization reports an infection rate of 3.9%
(Casale & McCarthy 2009). Only infections confirmed by a positive culture were counted.
Therefore, this number is likely an underestimation of the true infection rate. An additional 5%
of the cases were treated with empirical antibiotics without definitive diagnosis (Casale &
McCarthy 2009). This number is similar to the
infection rate of 4.2% in another study (Frey et al.
2010). Extracapsular techniques using braided
polyester sutures appear to have similar infection rates (Cook et al. 2010; Raske & Hulse
2013), though insufficient evidence has been
published to allow any conclusion at this time.
Pathogens
Coagulase-positive Staphylococcus spp. such as
S. pseudintermedius and S. aureus are responsible for the majority of infections, while other
bacteria such as Streptococcus spp., Enterococcus spp., Escherichia coli and Pseudomonas aeruginosa and others are encountered with less frequency (Fitzpatrick & Solano 2010; Thompson
et al. 2011; Gallagher & Mertens 2012; Dal-bó
et al. 2013; Etter et al. 2013; Savicky et al. 2013;
325
Nazarali et al. 2015; Yap et al. 2015). The
increased incidence of infection caused by
multi-drug-resistant (MDR) bacteria is of particular concern for both human and veterinary
surgery, as the treatment of these infections is
particularly challenging. In stifle surgery, the
proportion of infections caused by an MDR bacteria range between 10% and 58% (Fitzpatrick &
Solano 2010; Gallagher & Mertens 2012; Etter
et al. 2013; Savicky et al. 2013; Yap et al. 2015).
In a multi-center study, 38% of TPLO infections were caused by a MDR bacterium. Staphylococci were particularly prone to show drug
resistance, with up to 60% of S. pseudintermedius
and 50% of S. aureus being methicillin-resistant
(Nazarali et al. 2015).
Risk factors predisposing patients to infection after stifle surgery are multiple and, for
the most part, similar to the risk factors in
other surgeries: Wound classification, type of
procedure, American Society of Anesthesiologists (ASA) score, obesity, gender and neutering status, endocrinopathies, duration of anesthesia or surgery, number of people in the
operating theater, use of skin staples, timing
of clipping, and so forth have all been associated with an increased risk of infection (Beal
et al. 2000; Nicholson et al. 2002; Eugster et al.
2004; Fitzpatrick & Solano 2010; Frey et al. 2010;
Yap et al. 2015). Risks factors for methicillinresistant S. pseudintermedius (MRSP) infections
after TPLO surgery include being an MRSP carrier and being a Bulldog (Nazarelli et al. 2015).
The postoperative, prophylactic use of antibiotics is a highly debated subject in both human
and veterinary surgery. Routine postoperative
antibiotic treatment beyond 24 hours is not recommended in people undergoing clean surgical procedures as this practice has not been
shown to reduce SSI rates and may contribute
to the development of antimicrobial resistance
and additional morbidity (Mangram et al. 1999;
Bratzler & Houck 2005). However, several
recent veterinary studies do suggest a benefit
of administering postoperative antibiotics after
cruciate ligament rupture surgery, in particular
after TPLO (Fitzpatrick & Solano 2010; Frey et al.
2010; Gatineau et al. 2011; Nazarali et al. 2015). In
those studies, the administration of antibiotics
for 3 to 14 days had a significant protective effect
against infections. The duration of antibiotic
prophylaxis required is unknown, and none of
VetBooks.ir
326
Surgical Treatment
the studies was specifically designed to address
this question. Prospective studies are, therefore,
needed to validate these findings.
Diagnosis
Even though SSI can occur up to a year postoperatively, most infections are diagnosed within
the first couple of months after surgery. In a
study of 1000 TPLOs, the average time between
surgery and diagnosis of infection was 25 days
(range 7–60 days) if the dogs were treated with
antibiotics postoperatively, and 18 days (range
7–30 days) for dogs that did not receive postoperative antibiotics (Fitzpatrick & Solano 2010).
Similarly, for TTA, the average interval was 42
days, with 67% of infections diagnosed before
30 days (Yap et al. 2015).
The infection can be localized around the surgical implants and the osteotomy site or be
intra-articular, or both. Septic arthritis is relatively infrequent and is present in roughly 10–
16% of infections (Priddy et al. 2003; Yap et al.
2015). Clinical signs vary, but are typical for
infection: Localized heat, redness, pain, or tenderness are usually present. The swelling and
bruising may be localized around the implant
or involve the entire distal limb. Excessive
incisional discharge may develop soon after
surgery in acute cases, while chronic cases may
develop draining tracts. Dehiscence of the incision, often to the level of the bone plate, can
also be observed. In some cases, systemic signs
such as depression and fever may be detectable
(Marchevsky & Read 1999; Thompson et al.
2011). In most cases, increased lameness is evident. Animals affected with acute septic arthritis often present with a severe lameness. However, low-level, chronic septic arthritis cases
may be presented with a less severe but lingering lameness (Hill et al. 1999; Marchevsky &
Read 1999; Fitch et al. 2003).
Radiographic signs of infection are generally mild and non-specific unless the infection
is severe and chronic. Periosteal reaction and
radiolucency around surgical implants can be
observed in chronic cases, but are often absent
in the more acute cases (Trampuz & Zimmerli
2006; Yap et al. 2015). Joint effusion is often
detected in cases with septic arthritis (Fitch et al.
2003).
Arthrocentesis and analysis of synovial fluid
is a quick and reliable way to rule out joint
involvement. Care must be taken to avoid iatrogenic contamination of the joint when performing the arthrocentesis. Aseptic preparation of
the skin is carefully performed and a puncture
site away from the site of infection is selected, if
possible. Septic arthritis is often associated with
a markedly increased synovial cell count consisting primarily of neutrophils (Marchevsky &
Read 1999). In many cases, toxic changes to
synovial neutrophils are absent. Therefore, this
feature should not be used to rule out a septic process (Marchevsky & Read 1999). Aerobic
culture of the synovial fluid should be performed. However, only 50% of the cultures
are expected to yield positive results (Montgomery et al. 1989; Marchevsky & Read 1999;
Clements et al. 2005; Scharf et al. 2015). Enrichment in the blood culture medium as a way to
increased sensitivity of the cultures has been
recommended but has been met with mixed
results (Montgomery et al. 1989; Marchevsky &
Read 1999; Scharf et al. 2015).
Deep aspiration of the fluid around the surgical implant before surgery or intraoperative
tissue culture are the best ways of diagnosing
implant-associated infection (Trampuz & Zimmerli 2006). Similar to synovial fluid, culture of
fluid from around the implant can have a low
sensitivity. Therefore, a negative culture should
not, by itself, rule out infection (Darouiche
2004). If necessary, sonication of the implant can
be used to increase sensitivity of the cultures,
but is not routinely available (Trampuz & Zimmerli 2006). Because of the high incidence of
MDR bacteria (Nazarali et al. 2015) it is essential to obtain culture and sensitivity panels.
Extended sensitivity panels may be required for
MDR bacteria. In the absence of a positive culture but clinical evidence of infection, empirical antibiotics can be administered based on the
best evidence of bacterial flora and resistance
patterns prevalent in each hospital.
Treatment
Treatment will depend on the severity of the
infection, the location of infection, and the stage
of healing. Infections diagnosed early without
evidence of abscess formation are often initially
VetBooks.ir
Diagnosis and Management of Orthopaedic Infection after Stifle Surgery
treated by systemic administration of an appropriate antibiotic. If bone consolidation or joint
stabilization has not yet been achieved, the goal
of treatment is to control the infection to prevent the development of chronic osteomyelitis
until consolidation is achieved (Darouiche 2004;
Trampuz & Zimmerli 2006). More severe infections, those involving the stifle joint, or those
associated with the formation of an abscess
or wound dehiscence, require more aggressive
treatment.
Due to the devastating effect of untreated
septic arthritis, joint lavage, surgical drainage
and debridement have been recommended
over the administration of antibiotics alone for
the treatment of post-surgical septic arthritis
(Marchevsky & Read 1999). However, the
superiority of this treatment over the administration of antibiotics alone for cases that
do not involve intra-articular implants has
not been clearly demonstrated (Fitch et al.
2003; Clements et al. 2005). Lavage can be
performed using large ingress/egress needles
or through arthrotomy and joint exploration
(Marchevsky & Read 1999). The required
duration of antibiotic administration for septic
arthritis is unknown, but 4–6 weeks has been
recommended (Marchevsky & Read 1999;
Fitch et al. 2003; Clements et al. 2005). The
use of intra-articular gentamicin-impregnated
collagen sponges has been described for the
treatment of septic arthritis in the dog and
other species (Owen et al. 2004). However, this
method cannot be recommended due to the
short intra-articular elution times of the gentamicin and the persistent joint inflammation
caused by the collagen sponge (Hayes et al.
2016).
Similar to other orthopaedic infections, infections associated with abscess formation, dehiscence or chronic osteomyelitis should be treated
with wound exploration, debridement, and
drainage (Figure 40.1). Unstable implants are
removed and, if necessary, replaced. Open
wound management with delayed closure or
negative pressure wound therapy should be
considered for dehiscence or severe infections
(Budsberg 2012; Nolff et al. 2015). The use
of local antibiotic delivery systems does not
replace the need for long-term systemic antibiotic administration, but can be a useful addition
to treatment (Hayes et al. 2013). In severe cases
327
Figure 40.1 Intraoperative picture during debridement
of a deep incisional surgical site infection after tibial
plateau leveling osteotomy surgery. Although the skin
incision was opened by the surgeon, the caudal sartorius
muscle and fascial layer have dehisced, exposing the
plate.
that do not respond to traditional treatment,
intravenous regional perfusion of antibiotics
could be attempted. This procedure was first
described by Finsterbush et al. (1970) in rabbits with experimental septic arthritis and
osteomyelitis, and has been successfully used
in humans and horses (Finsterbush et al. 1970;
Finsterbush & Weinbergh 1972; Whithair et al.
1992; Rubio-Martı́nez & Cruz 2006). Regional
perfusion results in a higher synovial concentration of antibiotics than would result from intravenous administration alone (Whithair et al.
1992; Pille et al. 2005). It has been associated with
low morbidity, but has not been fully investigated in dogs.
Infections associated with the implant that
develop after bone consolidation are often
VetBooks.ir
328
Surgical Treatment
treated by implant removal, followed by a short
course of antibiotics. Gram-positive aerobic
bacteria have the capacity to produce polysaccharide biofilm, making eradication without
removing the implant difficult (Jacques et al.
2010; Singh et al. 2013). One study highlighted
the importance of implant removal by showing that implant removal alone was just as efficient as implant removal with antimicrobial use,
and more effective than antimicrobial administration without implant removal (Savicky et al.
2013). In some situations, implant removal
is not always easy or possible. Despite the
general recommendation to remove implants
after infection, a successful resolution of infection without implant removal or after partial
removal has been achieved in several studies
(Fitzpatrick & Solano 2010; Savicky et al. 2013;
Yap et al. 2015). Risk of long-term recurrence in
such cases is unknown.
Prognosis and economic impact
Despite the high incidence of infection and the
incidence of MDR bacteria, infections of the
stifle joint generally carry a favorable prognosis
if treated appropriately. Resolution of infection
has been achieved in 95% of cases, and lameness resolution can be observed around 38 days
(range 15–45 days) after initiation of treatment
(Fitzpatrick & Solano 2010; Savicky et al. 2013).
In many cases, treatment requires prolonged
antibiotic administration and results in additional client visits, hospitalization days, or
surgeries. The economic impact of SSI has been
evaluated after TPLO by Nicoll et al. (2014), and
can represent a significant burden on the owner.
In this Canadian study, the average postoperative cost for dogs that developed SSI was $1559,
compared to an average cost of $212 for dogs
that did not experience complications. Depending on the severity of the infection and treatments required, the postoperative costs varied
between $145 and $5022. Presumably, the cost of
treating a MDR bacterium could be higher than
the cost of treating a non-resistant SSI ($2294
versus $1674). However, the difference was not
significant in this publication (Nicoll et al. 2014).
In addition to the financial burden, postoperative complications are also likely to decrease
client satisfaction and confidence in the
procedure.
Conclusions
Despite all the medical advances and the discovery of antibiotics more than 60 years ago,
it is clear that surgical infections are here to
stay. Even though infections rates have drastically decreased, the proportion of infections
caused by MDR bacteria continues to increase.
If the trend continues, there will soon come a
post-antibiotic era in which all currently known
antibiotics would be ineffective. Resistance to
each and every one of the currently known
antibiotic classes has already been observed
(Alanis 2005). Inappropriate use of antibiotics,
complacence, and the lack of discovery of new
antibiotics have been largely blamed for this
alarming trend (Overbye & Barrett 2005). Veterinarians are not exempt from responsibility,
and the appropriate use of antibiotics is, more
than ever, of the upmost importance to reduce
or delay the development of bacterial resistance. It is clear that accurate data on infection
rates and evidence-based guidelines for the correct use of antibiotics in veterinary surgery are
lacking and must be developed. While there
is a renewed push for the discovery of new
antibiotics (Clardy et al. 2006; O’Connell et al.
2013), current research has been focused on
understanding the mechanism of drug resistance, its epidemiology, and the role of biofilm.
Understanding these may lead to new ways
of disrupting the bacterial defense systems to
increase the efficacy of the drugs currently
available. Meanwhile, another body of research
is already preparing for a post-antibiotic times,
evaluating novel strategies for fighting infections without the use of antibiotics (Kaufmann
2007; de Oca 2013). What the situation will be
in 5–10 years largely depends on the results of
these different research avenues.
References
Alanis AJ. Resistance to antibiotics: are we in the postantibiotic era? Arch Med Res 2005;36:697–705.
Alexander JW. The contributions of infection control to a century of surgical progress. Ann Surg
1985;201:423–428.
Anderson DJ. Surgical site infections. Infect Dis Clin
North Am 2011;25:135–153.
Beal MW, Brown DC, Shofer FS. The effects of
perioperative hypothermia and the duration of
anesthesia on postoperative wound infection rate
VetBooks.ir
Diagnosis and Management of Orthopaedic Infection after Stifle Surgery
in clean wounds: a retrospective study. Vet Surg
2000;29:123–127.
Bratzler DW, Houck PM. Antimicrobial prophylaxis for surgery: an advisory statement from the
National Surgical Infection Prevention Project. Am
J Surg 2005;189:395–404.
Budsberg SC. Osteomyelitis, In, Tobias KA, Johnston
SA (eds), Veterinary Surgery: Small Animal, 1st ed.,
St Louis, 2012, Saunders/Elsevier, pp. 669–675.
Casale SA, McCarthy RJ. Complications associated
with lateral fabellotibial suture surgery for cranial
cruciate ligament injury in dogs: 363 cases (1997–
2005). J Am Vet Med Assoc 2009;234:229–235.
Clardy J, Fischbach MA, Walsh CT. New antibiotics
from bacterial natural products. Nat Biotechnol
2006;24:1541–50.
Clements DN, Owen MR, Mosley JR, et al. Retrospective study of bacterial infective arthritis in 31 dogs.
J Small Anim Pract 2005;46:171–176.
Clerfond P, Huneault L, Dupuis J, et al. Unilateral
or single-session bilateral surgery for correction of
medial patellar luxation in small dogs: short and
long-term outcomes. Vet Comp Orthop Traumatol
2014;27:484–490.
Cohen ML. Epidemiology of drug resistance: implications for a post-antimicrobial era. Science 1992;
257:1050–1055.
Cook JL, Luther JK, Beetem J, et al. Clinical comparison of a novel extracapsular stabilization procedure and tibial plateau leveling osteotomy for
treatment of cranial cruciate ligament deficiency in
dogs. Vet Surg 2010;39:315–323.
Corr SA, Brown C. A comparison of outcomes following tibial plateau levelling osteotomy and cranial tibial wedge osteotomy procedures. Vet Comp
Orthop Traumatol 2007;20:312–319.
Culver DH, Horan TC, Gaynes RP, et al. Surgical
wound infection rates by wound class, operative
procedure, and patient risk index National Nosocomial Infections Surveillance System. Am J Med
1991;91:152S–157S.
Dal-bó Í, Ferrigno CRA, Ferreira MP, et al. Infecção
óssea após osteotomia para tratamento da ruptura
de ligamento cruzado em cães. Acta Sci Vet 2013;
41:1–7.
Darouiche RO. Treatment of infections associated
with surgical implants. N Engl J Med 2004;350:
1422–1429.
de Oca E. Antimicrobial peptide elicitors: new hope
for the post-antibiotic era. Innate Immun 2013;19:
227–241.
de Lima Dantas B, Sul R, Parkin T, et al. Incidence
of complications associated with tibial tuberosity
advancement in Boxer dogs. Vet Comp Orthop
Traumatol 2015;29:39–45.
Eisenberg D. Surgical site infections: Time to modify
the wound classification system? J Surg Res 2012;
175:54–55.
Etter SW, Ragetly GR, Bennett RA, et al. Effect of using
triclosan-impregnated suture for incisional closure
329
on surgical site infection and inflammation following tibial plateau leveling osteotomy in dogs. J Am
Vet Med Assoc 2013;242:355–358.
Eugster S, Schawalder P, Gaschen F, et al. A prospective study of postoperative surgical site infections
in dogs and cats. Vet Surg 2004;33:542–550.
Finsterbusch A, Argaman M, Sacks T. Bone and joint
perfusion with antibiotics in the treatment of experimental staphylococcal infection in rabbits. J Bone
Joint Surg Am 1970;52: 1424–32.
Finsterbush A, Weinberg H. Venous perfusion of the
limb with antibiotics for osteomyelitis and other
chronic infections. J Bone Joint Surg Am 1972;54:
1227–34.
Fitch RB, Hogan TC, Kudnig ST. Hematogenous septic arthritis in the dog: results of five patients
treated nonsurgically with antibiotics. J Am Anim
Hosp Assoc 2003;39:563–566.
Fitzpatrick N, Solano MG. Predictive variables for
complications after TPLO with stifle inspection
by arthrotomy in 1000 consecutive dogs. Vet Surg
2010;39:460–474.
Frey TN, Hoelzler MG, Scavelli TD, et al. Risk factors for surgical site infection-inflammation in dogs
undergoing surgery for rupture of the cranial cruciate ligament: 902 cases (2005-2006). J Am Vet Med
Assoc 2010;236:88–94.
Gallagher AD, Mertens WD. Implant removal
rate from infection after tibial plateau leveling
osteotomy in dogs. Vet Surg 2012;41:705–711.
Gatineau M, Dupuis J, Planté J, et al. Retrospective
study of 476 tibial plateau levelling osteotomy procedures: Rate of subsequent “pivot shift”, meniscal tear and other complications. Vet Comp Orthop
Traumatol 2011;24:333–341.
Gibbons SE, Macias C, Tonzing MA, et al. Patellar luxation in 70 large breed dogs. J Small Anim Pract
2006;47:3–9.
Hayes GM, Gibson TWG, Moens NMM, et al. Intraarticular implantation of gentamicin impregnated
collagen sponge causes joint inflammation and
impaired renal function in dogs. Vet Comp Orthop
Traumatol 2016;29:159–163.
Hayes GM, Moens NMM, Gibson TWG. A review of
local antibiotic implants and applications to veterinary orthopaedic surgery. Vet Comp Orthop Traumatol 2013;26:251–259.
Hill CM, Conzemius MG, Smith GK, et al. Bacterial
culture of the canine stifle joint following surgical repair of ruptured cranial cruciate ligament. Vet
Comp Orthop Traumatol 1999;12:1–5.
Jacques M, Aragon V, Tremblay YDN. Biofilm formation in bacterial pathogens of veterinary importance. Anim Heal Res Rev 2010;11:97–121.
Kalff S, Butterworth SJ, Miller A, et al. Lateral patellar
luxation in dogs: a retrospective study of 65 dogs.
Vet Comp Orthop Traumatol 2014;27:130–134.
Kaufmann SHE. The contribution of immunology to
the rational design of novel antibacterial vaccines,
Nat Rev Microbiol 2007;5:491–504.
VetBooks.ir
330
Surgical Treatment
Lafaver S, Miller NA, Stubbs WP, et al. Tibial tuberosity advancement for stabilization of the canine cranial cruciate ligament-deficient stifle joint: surgical
technique, early results, and complications in 101
dogs. Vet Surg 2007;36:573–586.
Mangram Al J, Horan TC, Pearson ML, et al. Guideline for Prevention of Surgical Site Infection,
1999 Centers for Disease Control and Prevention
(CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control 1999;27:97–
132.
Marchevsky AM, Read RA. Bacterial septic arthritis
in 19 dogs. Aust Vet J 1999;77:233–237.
Montgomery RD, Long IR, Milton JL, et al. Comparison of aerobic culturette, synovial membrane
biopsy, and blood culture medium in detection of
canine bacterial arthritis. Vet Surg 1989;18:300–303.
Nazarali A, Singh A, Moens NMM, et al. Association
between methicillin-resistant Staphylococcus pseudintermedius carriage and the development of surgical site infections following tibial plateau leveling osteotomy in dogs. J Am Vet Med Assoc
2015;247:909–916.
Nazarali A, Singh A, Weese JS. Perioperative administration of antimicrobials during tibial plateau leveling osteotomy. Vet Surg 2014;43:966–971.
Nelson LL. Surgical site infections in small animal
surgery. Vet Clin North Am - Small Anim Pract
2011;41:1041–1056.
Nicholson M, Beal M, Shofer F, et al. Epidemiologic
evaluation of postoperative wound infection in
clean-contaminated wounds: A retrospective study
of 239 dogs and cats. Vet Surg 2002;31:577–581.
Nicoll C, Singh A, Weese JS. Economic impact of tibial
plateau leveling osteotomy surgical site infection in
dogs. Vet Surg 2014;43:899–902.
Nolff MC, Fehr M, Bolling A, et al. Negative pressure
wound therapy, silver coated foam dressing and
conventional bandages in open wound treatment
in dogs. A retrospective comparison of 50 paired
cases. Vet Comp Orthop Traumatol 2015;28:30–38.
O’Connell KMG, Hodgkinson JT, Sore HF, et al.
Combating multidrug-resistant bacteria: current
strategies for the discovery of novel antibacterials.
Angew Chem Int Ed Engl 2013;52:10706–33.
Overbye KM, Barrett JF. Antibiotics: where did we go
wrong? Drug Discov Today 2005;10:45–52.
Owen MR, Moores AP, Coe RJ. Management of
MRSA septic arthritis in a dog using a gentamicinimpregnated collagen sponge. J Small Anim Pract
2004;45:609–612.
Pacchiana PD, Morris E, Gillings SL, et al. Surgical and
postoperative complications associated with tibial
plateau leveling osteotomy in dogs with cranial
cruciate ligament rupture: 397 cases (1998-2001).
J Am Vet Med Assoc 2003;222:184–193.
Pille F, De Baere S, Ceelen L, et al. Synovial fluid and
plasma concentrations of ceftiofur after regional
intravenous perfusion in the horse. Vet Surg
2005;34:610–7.
Priddy NH, Tomlinson JL, Dodam JR, et al. Complications with and owner assessment of the outcome
of tibial plateau leveling osteotomy for treatment of
cranial cruciate ligament rupture in dogs: 193 cases
(1997-2001). J Am Vet Med Assoc 2003;222:1726–
1732.
Proot JLJ, Corr SA. Clinical audit for the tibial
tuberosity advancement procedure: establishing
the learning curve and monitoring ongoing performance for the tibial tuberosity advancement
procedure using the cumulative summation technique. Vet Comp Orthop Traumatol 2013;26:280–
284.
Raske M, Hulse D. SwiveLock bone anchor stabilization of the cranial cruciate ligament deficient
stifle in dogs: Clinical Outcome. Open J Vet Med
2013;03:297–301.
Rubio-Martı́nez LM, Cruz AM. Antimicrobial
regional limb perfusion in horses, J Am Vet Med
Assoc 2006;228:706–12.
Savicky R, Beale B, Murtaugh R, et al. Outcome following removal of TPLO implants with surgical
site infection. Vet Comp Orthop Traumatol 2013;26:
260–265.
Scharf VF, Lewis ST, Wellehan JF, et al. Retrospective
evaluation of the efficacy of isolating bacteria from
synovial fluid in dogs with suspected septic arthritis. Aust Vet J 2015;93:200–203.
Shaver SL, Mayhew KN, Sutton JS, et al. Complications after corrective surgery for lateral patellar luxation in dogs: 36 cases (2000-2011). J Am Vet Med
Assoc 2014;244:444–448.
Singh A, Walker M, Rousseau J, et al. Characterization of the biofilm forming ability of Staphylococcus pseudintermedius from dogs. BMC Vet Res
2013;9:93.
Thompson AM, Bergh MS, Wang C, et al. Tibial
plateau levelling osteotomy implant removal: a retrospective analysis of 129 cases. Vet Comp Orthop
Traumatol 2011;24:450–456.
Trampuz A, Zimmerli W. Diagnosis and treatment of
infections associated with fracture-fixation devices.
Injury 2006;37:59–66.
Vasseur PB, Levy J, Dowd E, et al. Surgical wound
infection rates in dogs and cats Data from a teaching hospital. Vet Surg 1992;17:60–64.
Whithair KJ, Bowersock TL, Blevins WE, et al.
Regional limb perfusion for antibiotic treatment of
experimentally induced septic arthritis. Vet Surg
1992;21:367–73.
Wolf RE, Scavelli TD, Hoelzler MG, et al. Surgical and postoperative complications associated
with tibial tuberosity advancement for cranial
cruciate ligament rupture in dogs: 458 cases
(2007–2009). J Am Vet Med Assoc 2012;240:1481–
1487.
Yap FW, Calvo I, Smith KD, et al. Perioperative risk
factors for surgical site infection in tibial tuberosity
advancement: 224 stifles. Vet Comp Orthop Traumatol 2015;28:199–206.
VetBooks.ir
Section V
Medical Management of Cruciate
Ligament Rupture
Introduction
Although several new nonsteroidal antiinflammatory drugs have entered the veterinary market over the past several years, a
limited number of different types of drug are
available for the treatment of stifle osteoarthritis. In contrast, a plethora of nutritional
supplements are available, although evidence
of clinical efficacy for many nutritional sup-
plements is limited. Physical therapy has an
important role in the management of dogs
with cruciate ligament rupture. There is growing evidence that appropriate rehabilitation
after surgical treatment of the stifle can have
important benefits to patient mobility.
This section provides a detailed discussion of
current medical therapies commonly used for
the treatment of dogs with the cruciate ligament
rupture.
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell. 331
VetBooks.ir
VetBooks.ir
41
Medical Therapy for Stifle
Osteoarthritis
Steven C. Budsberg
Introduction
Osteoarthritis (OA) of the stifle joint is a progressive degenerative disease in dogs, which
can have a profound impact on quality of life
(Vasseur & Berry 1992; Lazar et al. 2005; HielmBjorkman et al. 2011). The clinical signs of stifle OA include discomfort, limited joint range
of motion, loss of muscle mass and muscle tone,
and decreased overall limb use. The pain can be
difficult to control. One of the primary reasons
hindering successful management may be the
presence of central nervous system plasticity
(Knazovicky et al. 2016). Additionally, while OA
is considered a chronic progressive disease, the
clinical picture may be quite dynamic with both
intermittent periods of acute signs, or ‘flareups,’ and periods of clinical quiescence. Given
all of these cofactors, it is not surprising that
there is variation in the clinical impact between
individual dogs.
The goals of medical management are to
minimize the clinical signs of OA, maintain
or improve limb use and, if possible, slow the
progression of the disease. Remember, OA
of the joint is an end-stage process; current
medical management protocols are directed at
ameliorating those clinical signs. It has been
proposed that multimodal therapy can yield a
better response in the treatment of OA through
the synergism of various therapies acting in
non-competing modes of action. This allows
for the administration of collectively lower
doses of medication, decreasing the potential
side effects of any one treatment prescribed
(Altman et al. 2000). In addition to nonsteroidal
anti-inflammatory drugs (NSAIDs), multimodal therapy for the treatment of OA also
incorporates weight loss, exercise modification, rehabilitation, and diet supplementation
(Argoff 2002; Budsberg & Bartges 2006; Aragon
et al. 2007; Johnston et al. 2008; Vandeweerd et al.
2012; Monterio-Steagall et al. 2013; Comblain
et al. 2016).
In the last few years, a plethora of new interventions have been introduced as adjunctive
therapies for OA. These include, but are not
limited to, non-NSAID analgesics, purposed
disease-modulating agents, biological products
(e.g., autologous protein products, stem cell
products, monoclonal antibodies), other oral
supplements, and physical modalities such
as acupuncture and light therapy. Most of
these therapies have been employed without
extensive clinical trials to assess efficacy. It is
important to remember the need for blinded,
randomized, clinical trials to assess efficacy
of new treatments. A care-giver placebo effect
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
333
VetBooks.ir
334
Medical Management of Cruciate Ligament Rupture
for veterinary medicine is defined when sham
medical intervention causes pet care-givers,
such as owners or veterinarians, to believe
that the provided treatment improved the
pet’s condition. A significant care-giver placebo
effect has been documented in dogs with OA
(Conzemius & Evans 2012). The care-giver
placebo effect for owners evaluating their dog’s
lameness occurred 56.9% of occasions. A caregiver placebo effect for veterinarians occurred
44.8% of the time when they examined dogs
for lameness at a walk or a trot, and 43.1% of
the time when veterinarians evaluated dogs for
signs of pain on palpation of the joint. In all of
these measurements, the owner and veterinarian, who was blinded to the treatment, believed
there were improvements while the dog was on
placebo treatment.
Weight management
The importance of weight management in the
prevention and treatment of OA cannot be overestimated. A substantial portion of the patient
population is obese, and it is recognized that
obesity is an important medical disease in
dogs (German 2006; Laflamme 2012; German
2016). Obesity, defined as exceeding ideal body
weight by 15–20%, places excessive forces on
joints and articular cartilage, and is exacerbated
by inactivity, propagating a vicious cycle of
muscle atrophy and decreased overall fitness
(Impellizeri et al. 2000; Kealy et al. 2000). While
there is not a clear cause and effect relationship between obesity and OA, fat is considered a metabolically active tissue promoting
inflammation (Greenburg & Obin 2006). There
is growing evidence that inflammatory mediators released from adipose tissue, including the
cytokines interleukin 6 (IL-6) and tumor necrosis factor alpha (TNF-α), and the adipokines leptin, visfatin, adiponectin, adipsin and resistin,
may have roles in the pathogenesis of OA (Frye
et al. 2016). Levels of adipsin and leptin are
associated with knee OA progression in human
beings (Martel-Pelletier et al. 2016). It has also
been proposed that leptin could play a role in
the development of cruciate ligament rupture
in dogs by the alteration of ligament fibroblast and collagenase activity. However, further
research is needed to substantiate this claim
(Comerford et al. 2005; Otero et al. 2006). Despite
these controversies about the cause and effect
of obesity and OA, weight reduction has been
shown clinically to ameliorate the signs associated with OA and to have preventive effects.
Burkholder et al. (2000) demonstrated, in a population of overweight dogs with clinical signs
of hip dysplasia, that appropriate weight loss
markedly improved ground reaction forces and
joint mobility. Additionally, more recently, Marshall et al. (2010) showed decreased lameness
and improved kinetic gait analysis with body
weight reduction in dogs with hip and elbow
OA. A series of studies have assessed the protective benefits of a calorically restricted diet for
the development of OA (Kealy et al. 2000; Impellizeri et al. 2000; Kealy et al. 2002; Mlacnik et al.
2006; Smith et al. 2006).
Nonsteroidal anti-inflammatory drugs
NSAIDs are the most commonly prescribed
class of medications to alleviate the clinical
signs of OA and are the mainstay in any medical management. These drugs are effective, with
relatively low adverse effects. NSAIDs reduce
the formation of inflammatory prostaglandins,
primarily PGE2, and thromboxane production
by inhibiting cyclooxygenase (COX) enzymes in
the arachadonic acid (AA) pathway. With the
inhibition of COX isoenzymes, NSAIDs have a
local effect at the site of injury as well as a central effect minimizing spinal nociception and
central sensitization. NSAIDs may also sensitize
mu receptors to the effects of opioids, explaining the synergism between these two medications. The benefit exerted by NSAIDs in the
treatment of OA is indisputable. Recently, specific receptor antagonists have been developed
to act on receptors activated by PGE2. Pharmacologically, these PGE2 receptors are subdivided into at least four subtypes (EP1–EP4).
The distribution of these receptors is considered
when explaining the multiple effects of PGE2 in
various tissues (Narumiya et al. 1999; Kawabata
2011; Kawahara et al. 2015). There is increasing
evidence that demonstrates the effectiveness of
selective EP4 receptor antagonists as analgesics
in a variety of inflammatory pain models in a
variety of species (Lin et al. 2006; Nakao et al.
2007; Murase et al. 2008; Colucci et al. 2010), as
well as in clinical trials in dogs (Rausch-Derra
et al. 2015; Rausch-Derra et al. 2016). NSAIDs are
VetBooks.ir
Medical Therapy for Stifle Osteoarthritis
not without adverse effects and must be used
judiciously, especially in dogs with pre-existing
conditions.
The primary selection of an NSAID is based
on individual analgesic and adverse responses.
Despite similar efficacies between different
NSAIDs, there can be a dramatic difference in
individual response. It may be necessary to try
different NSAIDs until an acceptable level of
analgesia is obtained or the patient experiences
an adverse response. Given that a patient may
need to be medicated with different NSAIDs,
there is extensive debate concerning the necessity or length of washout between the administration of sequential NSAIDs with little data
to support any particular dosing protocols (Lascelles et al. 2005; Ryan et al. 2007). However,
there is one situation in which a washout period
can strongly be considered, which is following
the use of aspirin. Aspirin use induces aspirintriggered lipoxins (ATL), which have protective
effects on the stomach lining. ATLs diminish
gastric mucosal injury from nitric oxide produced by traumatized vascular endothelium
(Souza et al. 2003). The concurrent or immediate
administration of other NSAIDs, particularly
COX-2 selective or COX-1 sparing drugs, will
completely block these lipoxins and their protective effects, thus increasing the risk of gastric
ulceration.
Additional analgesics
Although NSAIDs are traditionally the first
line of pharmaceuticals used to treat OA, they
incompletely suppress the inflammatory process through a limited mechanism of action
and, therefore, are not completely effective at
obviating the clinical signs of OA. A multimodal approach incorporating additional analgesics with differing mechanisms and sites of
action is often indicated for improved pain control while lowering the therapeutically effective
dose, thereby minimizing the adverse effects of
NSAIDs (Lascelles et al. 2008).
Amantadine
Amantadine, first recognized as an anti-viral
agent, has gained popularity for the treatment
of chronic pain disorders via the inhibition of
335
N-methyl-D-aspartate (NMDA) receptors.
NMDA receptor activation, secondary to
chronic stimulation of A delta and C fibers, is
believed to be the primary component leading to ‘spinal windup.’ A study by Lascelles
et al. (2008) compared the effects of adjunctive
amantadine with meloxicam in a population
of dogs with chronic OA refractory to NSAID
therapy alone. Dogs treated with meloxicam
in conjunction with amantadine had improved
client-specific outcome measure scores and
overall activity, compared with the administration of meloxicam alone.
Tramadol
Tramadol is an opioid analgesic acting at the mu
receptor while inhibiting serotonin uptake and
norepinephrine re-uptake (Raffa et al. 1992). Tramadol also inhibits central pro-inflammatory
cytokines and acts as an agonist of the transient
receptor potential vanilloid 1 (TRPV1) receptor, influencing various neuronal cation channels while locally decreasing IL-6 and substance
P (Marincsak et al. 2008). Only one investigation
has been conducted in dogs with OA to evaluate the effects of oral tramadol in a blinded
study using positive and negative controls. A
significant improvement was noted in the positive control group (carprofen, 2.2 mg kg–1
twice daily) and the tramadol (4 mg kg–1 three
times daily) group compared with the placebo
group (administered three times daily) using
the canine brief pain inventory questionnaire
(Malek et al. 2012). However, several other
outcome measures in this study showed no
improvement over placebo or baseline during
the administration of tramadol. Thus, the limited data from this study is difficult to assess in
terms of recommending tramadol use in dogs
with OA.
Gabapentin
Gabapentin is structurally similar to the
central inhibitory neurotransmitter gammaaminobutyric acid (GABA). The latter is
synthesized from glutamate, an excitatory
neurotransmitter. During periods of chronic
pain, there is an upregulation of glutamate and
subsequent NMDA receptor activation with a
VetBooks.ir
336
Medical Management of Cruciate Ligament Rupture
relative decrease in GABA concentration. This
results in the loss of an endogenous feedback
mechanism and an uninhibited nociceptive
pathway. Although gabapentin’s mechanism
of action was initially assumed to be through
GABAergic transmission, the therapeutic
effects are believed to be moderated through
the alpha2 subunit of voltage-gated calcium
channels, resulting in central analgesia (Davies
et al. 2007). To the present author’s knowledge,
there are no available clinical or experimental
studies evaluating the role of gabapentin in
treatment of OA in dogs.
Anti-nerve growth factor antibody
As a member of the neurotrophin family, nerve
growth factor (NGF) can bind the general neurotrophin receptor p75, as well as its highaffinity cognate receptor, tropomyosin-related
kinase (Trk)A (Mantyh et al. 2011). The NGFTrkA pathway in particular appears to be critical in driving acute and chronic pain. Recently,
canine and feline versions of anti-NGF antibodies have been developed. Two recent studies, where dogs with OA were treated with
anti-NGF antibodies, yielded promising results
(Webster et al. 2014; Lascelles et al. 2015).
stem cells (MSCs). MSCs have high proliferative and self-renewal capabilities, are adhesive
to plastic surfaces, demonstrate specific cellsurface proteins, and have the potential to differentiate in at least three lineages including
bone, cartilage, and adipose tissue. The second category is plasma-based products such
as platelet-rich plasma (PRP). PRP consists of
a pool of signaling proteins including growth
factors, cytokines, and other adhesive proteins
involved in healing mechanisms. The list is
not exhaustive. The final category is conditioned culture media, which contain biologically active molecules secreted by cells in vitro;
these molecules affect cell functions.
Autologous and, more recently, allogenic
stem cell therapies have shown some limited
positive results in clinical trials when given to
dogs with OA (Black et al. 2007; Black et al.
2008; Guercio et al. 2012; Vilar et al. 2013; Cuervo
et al. 2014; Vilar et al. 2014; Harman et al. 2016).
Additionally, studies of limited size and scope
have shown initial positive results for autologous plasma/platelet treatments in dogs with
OA (Fahie et al. 2013; Franklin & Cook 2013;
Wanstrath et al. 2016). At present, no clinical
data are available on conditioned culture media.
Chondromodulating agents
Botulinum toxin A
Botulinum toxin A is a potent neurotoxin produced by the bacterium Clostridium botulinum.
The toxin inhibits the release of neurotransmitters involved in direct pain perception. Thus,
intra-articular injection of this product may
have direct local anti-nociceptive properties in
painful osteoarthritic joints. Two small studies have been performed in dogs to evaluate
the intra-articular injection of botulinum toxin
with limited positive results (Hadley et al. 2010;
Heikkila et al. 2014).
Biological products
Current regenerative technologies for musculoskeletal injuries consist of three general categories. The first category is adult mesenchymal stromal cells, also known as mesenchymal
Recently, increased interest has been shown in
the alternative management of OA, not only to
alleviate clinical signs associated with the disease, but also to slow the process of cartilage
degradation and to promote cartilage synthesis.
Polysulfated glycosaminoglycan
Polysulfated glycosaminoglycan (PSGAG) is
a synthetic mixture of highly sulfated GAGs,
principally chondroitin sulfate, extracted from
bovine lung and tracheal cartilage (Todhunter &
Lust 1994). PSGAGs are beneficial in the treatment of OA by inhibiting cartilage-degradative
enzymes IL-1, matrix metalloproteinases
(MMPs), lysosomal elastase, cathepsin G,
PGE2, the formation of oxygen radicals, and
C3a and C5a complement fragments (Todhunter & Lust 1994; Sevalla et al. 2000; Mertens
et al. 2003; Fujiki et al. 2007). PSGAGs stimulate
VetBooks.ir
Medical Therapy for Stifle Osteoarthritis
cartilage repair processes by promoting protein
synthesis, collagen formation, and increasing
GAG and hyaluronan concentration (Glade
1990). PSGAGs also maintain chondrocyte
viability and stimulate chondrocyte division,
thereby slowing the process of extracellular
matrix degradation (Glade 1990; Sevalla et al.
2000). Since PSGAGs are a heparin analog, their
use in dogs with coagulopathies or concurrent
administration of NSAIDs, particularly those
with strong COX-1 (anti-thromboxane) activity,
is contraindicated. Limited clinical data that
supports the use of PSGAG in dogs with OA
are available (Lust et al. 1992; McNamara et al.
1997; Fujiki et al. 2007).
Hyaluronic acid
Hyaluronic acid (HA) is a linear, non-sulfated
GAG that is the primary constituent of synovial
fluid. HA interacts with aggrecan monomer
through non-covalent association to link
proteins to produce the large aggregating
polyglycosaminoglycans of articular cartilage
(McNamara et al. 1997). Administered HA is
speculated to increase synovial viscosity by
viscosupplementation. A variety of clinical and
experimental trials are available evaluating the
efficacy of HA for the treatment of cruciate ligament rupture. However, these studies yield conflicting data on HA’s ability to ameliorate the
progression of stifle OA (Schiavinato et al. 1989;
Marshall et al. 2000; Smith et al. 2001; Hellström
et al. 2003; Canapp et al. 2005; Smith et al. 2005;
Franklin & Cook 2013).
Dietary supplements
Omega-3 fatty acids
Nutritional supplementation with omega-3
(n-3) fatty acids has been proposed as an
adjunctive therapy for the management of OA.
The most prevalent of the polyunsaturated fatty
acids (PUFAs) comprising the cell membrane
are omega-6 (n-6) fatty acid and arachadonic
acid (AA). When the cell membrane, and therefore AA, is metabolized by the COX enzyme,
pro-inflammatory and vasoactive mediators of
2- and 4-series prostaglandins, thromboxanes,
337
and leukotrienes are produced. During the
process of OA, there is an increase in serum,
cartilage and synovial fluid concentrations of
n-6 PUFAs that propagate an inflammatory
reaction. The incorporation of n-3 PUFAs, eicosapentaenoic acid (EPA), into the cell membrane
will compete with AA for COX metabolism.
This results in the production of 3- and 5series prostaglandins, thromboxanes, and
leukotrienes that are significantly less inflammatory and vasoactive, curtailing the inflammatory response (Bauer 2007). There are several
n-3 fatty acids available, including EPA, docosahexainoid acid (DHA) and alpha-linolenic acid
(ALA), although EPA is the only n-3 PUFA with
selectivity for the chondrocyte cell membrane.
Several studies clinically support diet supplementation, including complete diets of high
dietary n-3 fatty acids, in the management of
OA (Miller 1992; Bartges et al. 2001; Roush et al.
2010; Hielm-Björkman et al. 2012; Moreau et al.
2013; Rialland et al. 2013; Mehler et al. 2016).
Glucosamine and chondroitin sulfate
Glucosamine and chondroitin sulfate formulations encompass the majority of nutritional supplements available on the current market for the
management of OA. Glucosamine is an aminomonosaccharide used in the synthesis of the disaccharide units of glycoasaminoglycan (McNamara et al. 1997; Neil et al. 2005). It can then
be incorporated into the large aggregating and
small-non-aggregating proteoglycans of articular cartilage, or as part of the disaccharide units
of hyaluronan. Chondroitin sulfate is a longchain polymer of repeating disaccharide units
of galactosamine sulfate and glucuronic acid
that constitutes the majority of glucosaminoglycans within articular cartilage (McNamara et al.
1997; Neil et al. 2005).
The mechanisms of action of chondroitin sulfate are synergistic with that of glucosamine,
and can stimulate the synthesis of endogenous
glycosaminoglycans and inhibit the synthesis of degradative enzymes, including MMPs.
Additionally, chondroitin sulfate inhibits both
IL-1-induced type II collagen degeneration,
histamine-induced inflammation, and has the
unique ability to improve synovial fluid viscosity by increasing hyaluronan concentration
VetBooks.ir
338
Medical Management of Cruciate Ligament Rupture
(McNamara et al. 1997; Kelly 1998; Canapp et al.
1999; Lippiello et al. 2000; Neil et al. 2005).
Notably, two studies evaluating the use of
glucosamine and chondroitin sulfate for the
amelioration of clinical signs associated with
OA yielded conflicting results. McCarthy et al.
(2007) demonstrated a positive effect on pain
score, weight-bearing, and severity of clinical
condition in dogs with hip and elbow OA, while
another study (Moreau et al. 2003) showed no
effect. Two small studies suggested positive
improvements when glucosamine and chondroitin sulfate are combined with glycosylated
undenatured type II collagen (D’Altilio et al.
2007; Gupta et al. 2012).
Avocado and soybean oil
unsaponifiables
Avocado and soybean oil unsaponifiables
(ASUs) are biologically active lipids believed to
have anti-inflammatory and anti-osteoarthritic
properties. ASUs decrease the expression of
inflammatory mediators and cartilage degradation (TNFα, IL-1β, COX-2, cytokine-inducible
nitric oxide synthase (iNOS), and MMPs)
and stimulate matrix synthesis by upregulating transforming growth factor beta (TGF-β)
expression by chondroblasts and osteoblasts
(Altinel et al. 2007; Au et al. 2007). A recent
experimental study reported the protective
effects of ASUs in a series of dogs with transected cranial cruciate ligaments (Boileau et al.
2009). Compared to the placebo group, dogs
treated with ASUs had smaller macroscopic
lesions on the tibial plateau. Histologically,
these dogs had decreased severity of tibial
and femoral cartilage lesions, synovitis, and
a decreased loss of subchondral bone and
calcified cartilage thickness compared with the
placebo group.
Conclusions
The goals of multimodal medical therapy are to
simultaneously maximize analgesia while minimizing the incidence and severity of adverse
effects and, if possible, to slow disease progression. This can be achieved by targeting multiple
sites along the nociceptive pathway, with the
inclusion of medications with varying mechanisms of action. It is important when creating,
maintaining, and adjusting multimodal regimens to remember that no individual responds
in the same manner, and no individual disease
progresses in the same way. It is imperative to
continually reassess the patient’s response and
adapt treatment as indicated.
References
Altinel L, Saritas ZK, Kose KC, et al. Treatment
with unsaponifiable extracts of avocado soybean
increases TGFB1 and TGFB2 levels in canine joint
fluid. Tohoku J Exp Med 2007;211:181–186.
Altman RD, Hochberg MC, Moskowitz RW, et al.
Recommendations for the medical management of
osteoarthritis of the hip and knee. Arthritis Rheum
2000;43:1905–1915.
Aragon CL, Hofmeister EH, Budsberg SC. Systematic review of clinical trials of treatments
for osteoarthritis in dogs. J Am Vet Med Assoc
2007;15;230:514–521.
Argoff CE. Pharmacologic management of chronic
pain. J Am Osteopath Assoc 2002;102:S21–S27.
Au RY, Al-Talib TK, Au AY, et al. Avocado soybean unsaponifiables (ASU) suppress TNFalpha, IL-1beta, COX-2, iNOS gene expression,
and prostaglandin E2 and nitric oxide production in articular chondrocytes and monocytes/
macrophages. Osteoarthritis Cartilage 2007;15:
1249–1255.
Bartges JW, Budsberg SC, Pazak HE, et al. Effects of
different n6:n3 fatty acid ratio diets on canine stifle
osteoarthritis. Proc Orthop Res Soc Annual Meeting 2001;47:462.
Bauer JE. Responses of dogs to dietary omega-3 fatty
acids. J Am Vet Med Assoc 2007;231:1657–1661.
Black L, Gaynor J, Gahring D, et al. Effect of adiposederived mesenchymal stem and regenerative cells
on lameness in dogs with chronic osteoarthritis
of the coxofemoral joints: a randomized, doubleblinded, multicenter, controlled trial. Vet Ther
2007;8:272–284.
Black L, Gaynor J, Adams C, et al. Effect of intraarticular injection of autologous adipose-derived mesenchymal stem and regenerative cells on clinical
signs of chronic osteoarthritis of the elbow joint in
dogs. Vet Ther 2008;9:192–200.
Boileau C, Martel-Pelletier J, Caron J, et al. Protective effects of total fraction of avocado/soybean
unsaponifiables on the structural changes in experimental dog osteoarthritis: inhibition of nitric oxide
synthase and matrix metalloproteinase-13. Arthritis Res Ther 2009;11:R41.
VetBooks.ir
Medical Therapy for Stifle Osteoarthritis
Budsberg SC, Bartges JW. Nutrition and osteoarthritis in dogs: does it help? Vet Clin North Am Small
Anim Pract 2006;36:1307–1323.
Burkholder WJ, Taylor L, Hulse DA. Weight loss to
optimal body condition increases ground reactive
force in dogs with osteoarthritis. Compend Cont
Educ Pract Vet 2000;23:74.
Canapp SO, McLaughlin RM, Hoskinson JJ, et al.
Scintigraphic evaluation of dogs with acute synovitis after treatment with glucosamine hydrochloride
and chondroitin sulfate. Am J Vet Res 1999;60:1552–
1557.
Canapp SO, Cross AR, Brown MP, et al. Examination of synovial fluid and serum following intravenous injections of hyaluronan for the treatment
of osteoarthritis in dogs. Vet Comp Orthop Traumatol 2005;18:169–174.
Colucci J, Boyd M, Berthelette C, et al. Discovery
of 4-{1-[({1-[4-(trifluoromethyl)benzyl]-1H-indol7-yl}carbonyl)amino]cyclopropyl}benzoic
acid
(MF-766), a highly potent and selective EP4 antagonist for treating inflammatory pain. Bioorg Med
Chem Lett 2010;20:3760–3763.
Comblain F, Serisier S, Barthelemy N, et al. Review
of dietary supplements for the management of
osteoarthritis in dogs in studies from 2004 to 2014.
J Vet Pharmacol Ther 2016;39:1–15.
Comerford EJ, Tarlton JF, Innes JF et al. Metabolism
and composition of the canine anterior cruciate ligament relate to difference in knee joint mechanics
and predisposition to ligament rupture. J Orthop
Res 2005;23:61–66.
Conzemius MG, Evans RB. Caregiver placebo effect
for dogs with lameness from osteoarthritis. J Am
Vet Med Assoc 2012;241:1314–1319.
Cuervo M, Rubio M, Sopena J, et al. Osteoarthritis
in dogs: a randomized study using mesenchymal
stem cells from adipose tissue and plasma rich in
growth factors. Int J Mol Sci 2014;15:13437–13460.
D’Altilio M, Peal A, Alvey M, et al. Therapeutic efficacy and safety of undenatured type II collagen
singly or in combination with glucosamine and
chondroitin in arthritic dogs. Toxicol Mech Methods 2007;17:189–196.
Davies A, Hendrich J, Van Minh AT, et al. Functional biology of the alpha(2)delta subunits of
voltage-gated calcium channels. Trends Pharmacol
Sci 2007;28:220–228.
Fahie MA, Ortolano GA, Guercio V, et al. A randomized controlled trial of the efficacy of autologous
platelet therapy for the treatment of osteoarthritis
in dogs. J Am Vet Med Assoc 2013;243:1291–1297.
Franklin SP, Cook JL. Prospective trial of autologous
conditioned plasma versus hyaluronan plus corticosteroid for elbow osteoarthritis in dogs. Can Vet
J 2013;54:881–884.
Frye CW, Shmalberg JW, Wakshlag JJ. Obesity, exercise and orthopedic disease. Vet Clin North Am
Small Anim Pract 2016;46:831–841
339
Fujiki M, Shineha J, Yamanokucki K, et al. Effects
of treatment of polysulfated glycosaominoglycan
on serum cartilage olgomeric matrix protein and
C-reactive protein concentrations, serum matrix
metalloproteinase-2 and -9 activities, and lameness in dogs with osteoarthritis. Am J Vet Res
2007;68:827–833.
German AJ. The growing problem of obesity in dogs
and cats. J Nutr 2006;136:1940S–1946S.
German AJ. Weight management in obese pets: the
tailoring concept and how it can improve results.
Acta Vet Scand. 2016;20:57.
Glade MJ. Polysulfated glycosaminoglycan accelerates net synthesis of collagen and glycosaminoglycans by arthritic equine cartilage tissues and chondrocytes. Am J Vet Res 1990;51:779–785.
Greenberg AS, Obin MS. Obesity and the role of adipose tissue in inflammation and metabolism. Am J
Clin Nutr 2006;83:S461–S465.
Guercio A, Di Marco P, Casella S, et al. Production
of canine mesenchymal stem cells from adipose
tissue and their application in dogs with chronic
osteoarthritis of the humeroradial joints. Cell Biol
Int 2012;36:189–194.
Gupta RC, Canerdy TD, Lindley J, et al. Comparative
therapeutic efficacy and safety of type-II collagen
(UC-II), glucosamine and chondroitin in arthritic
dogs: pain evaluation by ground force plate. J Anim
Physiol Anim Nutr (Berl) 2012;96:770–777.
Hadley HS, Wheeler JL, Petersen SW. Effects of intraarticular botulinum toxin type A (Botox) in dogs
with chronic osteoarthritis. Vet Comp Orthop Traumatol 2010;23:254–258.
Harman R, Carlson K, Gaynor J, et al. A prospective,
randomized, masked, and placebo-controlled efficacy study of intraarticular allogeneic adipose stem
cells for the treatment of osteoarthritis in dogs.
Front Vet Sci 2016;3:81.
Heikkila HM, Hielm-Björkman AK, Morelius M, et al.
Intra-articular botulinum toxin A for the treatment of osteoarthritic joint pain in dogs: a randomized, double-blinded, placebo-controlled clinical trial. Vet J 2014;200:162–169.
Hellström LE, Carlsson C, Boucher JF, et al. Intraarticular injections with high molecular weight
sodium hyaluronate as a therapy for canine arthritis. Vet Rec 2003;153:89–90.
Hielm-Björkman AK, Kapatkin AS, Rita HJ. Reliability and validity of a visual analogue scale used
by owners to measure chronic pain attributable
to osteoarthritis in their dogs. Am J Vet Res
2011;72:601–607.
Hielm-Björkman A, Roine J, Elo K, et al. An
un-commissioned randomized, placebo-controlled
double-blind study to test the effect of deep sea fish
oil as a pain reliever for dogs suffering from canine
OA. BMC Vet Res 2012;8:157.
Impellizeri JA, Tetrick MA, Muir P. Effect of weight
reduction on clinical signs of lameness in dogs
VetBooks.ir
340
Medical Management of Cruciate Ligament Rupture
with hip osteoarthritis. J Am Vet Med Assoc
2000;216:1089–1091.
Johnston SA, McLaughlin RM, Budsberg SC. Nonsurgical management of osteoarthritis in dogs. Vet
Clin North Am Small Anim Pract 2008;38:1449–
1470.
Kawabata A. Prostaglandin E2 and pain – an update.
Biol Pharm Bull 2011;34:1170–1073.
Kawahara K, Hohjoh H, Inazumi T, et al.
Prostaglandin E2-induced inflammation: Relevance of prostaglandin E receptors. Biochim
Biophys Acta 2015;1851:414–421.
Kealy RD, Lawler DF, Ballam JM, et al. Evaluation of
the effect of limited food consumption on radiographic evidence of osteoarthritis in dogs. J Am Vet
Med Assoc 2000;217:1678–1680.
Kealy RD, Lawler DF, Ballam JM, et al. Effects of diet
restriction on life span and age-related changes in
dogs. J Am Vet Med Assoc 2002;220:1315–1320.
Kelly GS. The role of glucosamine sulfate and chondroitin sulfates in the treatment of degenerative
joint disease. Altern Med Rev 1998;3:27–39.
Knazovicky D, Helgeson ES, Case B, et al. Widespread
somatosensory sensitivity in naturally occurring
canine model of osteoarthritis. Pain 2016;157:1325–
1332
Laflamme DP. Companion Animals Symposium:
Obesity in dogs and cats: What is wrong with being
fat? J Anim Sci 2012;90:1653–1662.
Lascelles BD, McFarland JM, Swann H. Guidelines for
safe and effective use of NSAIDs in dogs. Vet Ther
2005;6:237–251.
Lascelles BDX, Gaynor JS, Smith ES, et al. Amantidine
in a multimodal analgesic regimen for alleviation
of refractory osteoarthritis pain in dogs. J Vet Intern
Med 2008;22:53–59.
Lascelles BD, Knazovicky D, Case B, et al. A caninespecific anti-nerve growth factor antibody alleviates pain and improves mobility and function
in dogs with degenerative joint disease-associated
pain. BMC Vet Res 2015;11:101
Lazar TP, Berry CR, de Haan JJ, et al. Long-term
radiographic comparison of tibial plateau leveling osteotomy versus extracapsular stabilization
for cranial cruciate ligament rupture in the dog. Vet
Surg 2005;34:133–141.
Lin CR, Amaya F, Barrett L, et al. Prostaglandin
E2 receptor EP4 contributes to inflammatory
pain hypersensitivity. J Pharmacol Exp Ther
2006;319:1096–1103.
Lippiello L, Woodward J, Karpman R, et al. In vivo
chondroprotection and metabolic synergy of glucosamine and chondroitin sulfate. Clin Orthop Rel
Res 2000;381:229–240.
Lust G, Williams AJ, Burton-Wurster N, et al. Effects
of intramuscular administration of glycosaminoglycan polysulfates on signs of incipient hip dysplasia in growing pups. Am J Vet Res 1992;53:1836–
1843.
Malek S, Sample SJ, Schwartz Z, et al. Effect of
analgesic therapy on clinical outcome measures
in a randomized controlled trial using clientowned dogs with hip osteoarthirits. BMC Vet Res
2012;8:185.
Mantyh PW, Koltzenburg M, Mendell LM, et al.
Antagonism of nerve growth factor-TrkA signaling
and the relief of pain. Anesthesiology 2011;115:189–
204.
Marincsak R, Toth BI, Czifra G, et al. The analgesic
drug, tramadol, acts as an agonist of the transient receptor potential vanilloid-1. Anesth Analg
2008;106:1890–1896.
Marshall KW, Manolopoulos V, Mancer K, et al. Amelioration of disease severity by intraarticular hylan
therapy in bilateral canine osteoarthritis. J Orthop
Res 2000;18:416–425.
Marshall WG, Hazewinkel HA, Mullen D, et al. The
effect of weight loss on lameness in obese dogs with
osteoarthritis. Vet Res Commun 2010;34:241–253
Martel-Pelletier J, Raynauld JP, Dorais M, et al.
The levels of the adipokines adipsin and leptin are associated with knee osteoarthritis progression as assessed by MRI and incidence of
total knee replacement in symptomatic osteoarthritis patients: a post hoc analysis. Rheumatology
(Oxford) 2016;55:680–688.
McCarthy G, O’Donovan J, Jones B, et al. Randomised
double-blind, positive-controlled trial to assess the
efficacy of glucosamine/chondroitin sulfate for
the treatment of dogs with osteoarthritis. Vet J
2007;174:54–61.
McNamara PS, Johnston SA, Todhunter RJ. Slowacting disease-modifying osteoarthritis agents. Vet
Clin North Am Small Anim Pract 1997;27:863–
881.
Mehler SJ, May LR, King C, et al. A prospective, randomized, double blind, placebo-controlled
evaluation of the effects of eicosapentaenoic acid
and docosahexaenoic acid on the clinical signs
and erythrocyte membrane polyunsaturated fatty
acid concentrations in dogs with osteoarthritis. Prostaglandins Leukot Essent Fatty Acids
2016;109:1–7.
Mertens WD, MacLead JN, Fubini L, et al. Polysulphated glycosaminoglycans modulate transcription of interleukin-1B treated chondrocytes in
monolayer culture. Vet Comp Orthop Traumatol
2003;2:93–98.
Miller WH, Scott DW, Wellington JR. Treatment of
dogs with hip arthritis with a fatty acid supplement. Canine Pract 1992;17:6–8.
Mlacnik E, Bockstahler BA, Muller M, et al. Effects of
caloric restriction and a moderate or intense physiotherapy program for treatment of lameness in
overweight dogs with osteoarthritis. J Am Vet Med
Assoc 2006;229:1756–1760.
Monteiro-Steagall BP, Steagall PV, Lascelles BD. Systematic review of nonsteroidal anti-inflammatory
VetBooks.ir
Medical Therapy for Stifle Osteoarthritis
drug-induced adverse effects in dogs. J Vet Intern
Med 2013;27:1011–1019.
Moreau M, Dupuis J, Bonneau NH, et al. Clinical evaluation of a nutraceutical, carprofen and meloxicam
for the treatment of dogs with osteoarthritis. Vet
Rec 2003;152:323–329.
Moreau M, Troncy E, Del Castillo JR, et al. Effects of
feeding a high omega-3 fatty acids diet in dogs with
naturally occurring osteoarthritis. J Anim Physiol
Anim Nutr (Berl) 2013;97:830–837.
Murase A, Okumura T, Sakakibara A, et al. Effect of
prostanoid EP4 receptor antagonist, CJ-042,794, in
rat models of pain and inflammation. Eur J Pharmacol 2008;580:116–121.
Nakao K, Murase A, Ohshiro H, et al. CJ-023,423,
a novel, potent and selective prostaglandin EP4
receptor antagonist with antihyperalgesic properties. J Pharmacol Exp Ther 2007;322: 686–694.
Narumiya S, Sugimoto Y, Ushikubi F. Prostanoid
receptors: structure, properties and functions.
Physiol Rev 1999;79:1193–1226.
Neil KM, Caron JP, Orth MW. The role of glucosamine and chondroitin sulfate in treatment for
and prevention of osteoarthritis in animals. J Am
Vet Med Assoc 2005;226:1079–1088.
Otero M, Lago R, Gomez R, et al. Leptin: a metabolic
hormone that functions like a proinflammatory
adipokine. Drug News Perspect 2006;19:21–26.
Raffa RB, Friderichs E, Reimann W, et al. Opioid
and nonopioid components independently contribute to the mechanism of action of tramadol, an
‘atypical’ opioid analgesic. J Pharmacol Exp Ther
1992;260:275–285.
Rausch-Derra L, Huebner M, Wofford J, et al.
Prospective, randomized, masked, placebocontrolled multisite clinical study of grapiprant,
an EP4 prostaglandin receptor antagonist (PRA),
in dogs with osteoarthritis. J Vet Intern Med
2016;30:756–763.
Rausch-Derra LC, Huebner M, Rhodes L. Evaluation
of the safety of long-term, daily oral administration of grapiprant, a novel drug for treatment of
osteoarthritic pain and inflammation, in healthy
dogs. Am J Vet Res 2015;76:853–859.
Rialland P, Bichot S, Lussier B, et al. Effect of a
diet enriched with green-lipped mussel on pain
behavior and functioning in dogs with clinical
osteoarthritis. Can J Vet Res 2013;77:66–74.
Roush JK, Cross AR, Renberg WC, et al. Evaluation of
the effects of dietary supplementation with fish oil
omega-3 fatty acids on weight bearing in dogs with
osteoarthritis. J Am Vet Med Assoc 2010;236:67–73.
Ryan WG, Moldave K, Carithers D. Switching
NSAIDs in practice: insights from the Previcox
(firocoxib) experience trial. Vet Ther 2007;8:263–
271.
Schiavinato A, Lini E, Guidolin D, et al. Intraarticular sodium hyaluronate injections in the
341
Pond-Nuki experimental model of osteoarthritis
in dogs. II. Morphological findings. Clin Orthop
Relat Res 1989;241:286–299.
Sevalla K, Todhunter RJ, Verneir-Singer M, et al. Effect
of polysulfated glycosaminoglycan on DNA content and proteoglycan metabolism in normal and
osteoarthritic canine articular cartilage explants.
Vet Surg 2000;29:407–414.
Smith G, Jr, Myers SL, Brandt KD, et al. Effect
of intraarticular hyaluronan injection on vertical ground reaction force and progression of
osteoarthritis after anterior cruciate ligament transection. J Rheumatol 2005;32:325–334.
Smith GK, Paster ER, Powers MY, et al. Lifelong diet restriction and radiographic evidence of
osteoarthritis of the hip joint in dogs. J Am Vet Med
Assoc 2006;229:690–693.
Smith GN, Jr, Mickler EA, Myers SL, et al. Effect
of intraarticular hyaluronan injection on synovial
fluid hyaluronan in the early stage of canine posttraumatic osteoarthritis. J Rheumatol 2001;28:1341–
1346.
Souza MH, de Lima OM, Jr, Zamuner SR, et al. Gastritis increases resistance to aspirin-induced mucosal
injury via COX-2-mediated lipoxin synthesis. Am
J Physiol Gastrointest Liver Physiol 2003;285:54–
61.
Todhunter RJ, Lust G. Polysulfated glycosaminoglycan in the treatment of osteoarthritis. J Am Vet Med
Assoc 1994;8:1245–1251.
Vandeweerd JM, Coisnon C, Clegg P, et al. Systematic review of efficacy of nutraceuticals to alleviate clinical signs of osteoarthritis. J Vet Intern Med
2012;26:448–456.
Vasseur PB, Berry CR. Progression of stifle
osteoarthrosis following reconstruction of the
cranial cruciate ligament in 21 dogs. J Am Anim
Hosp Assoc 1992;28:129–136.
Vilar JM, Morales M, Santana A, et al. Controlled,
blinded force platform analysis of the effect
of intraarticular injection of autologous adiposederived mesenchymal stem cells associated to
PRGF-Endoret in osteoarthritic dogs. BMC Vet Res
2013;9:131.
Vilar JM, Batista M, Morales M, et al. Assessment
of the effect of intra-articular injection of autologous adipose-derived mesenchymal stem cells in
osteoarthritic dogs using a double blinded force
platform analysis. BMC Vet Res 2014;10:143.
Wanstrath AW, Hettlich BF, Su L, et al. Evaluation
of a single intra-articular injection of autologous
protein solution for treatment of osteoarthritis in a
canine population. Vet Surg 2016;45:764–774.
Webster RP, Anderson GI, Gearing DP. Canine Brief
Pain Inventory scores for dogs with osteoarthritis
before and after administration of a monoclonal
antibody against nerve growth factor. Am J Vet Res
2014;75:532–535.
VetBooks.ir
VetBooks.ir
42
Rehabilitation for Dogs with
Cruciate Ligament Rupture
Denis J. Marcellin-Little and Courtney J. Arnoldy
Introduction
Physical rehabilitation is routinely incorporated
into a plan for the care of dogs with cruciate ligament rupture (CR). Rehabilitation is
often performed during the early postoperative period after surgical stabilization, but is
also part of the conservative management of
dogs where surgery is not performed, or part
of the long-term management of dogs that fail
to thrive after surgery. The aim of this chapter
is to review rehabilitation goals and treatment
options for dogs with CR, to review the scientific evidence supporting rehabilitation, and to
discuss the selection of rehabilitation plans for
specific patients.
The goals of rehabilitation for dogs
with cruciate ligament rupture
The goals of rehabilitation for dogs recovering
from surgery to stabilize stifle joints with
CR include providing pain relief throughout
recovery, eliminating postoperative edema,
maintaining or recovering stifle joint motion,
promoting controlled limb use, preventing and
recovering from a loss of muscle mass and
from changes in posture resulting from chronic
pain and limb disuse, preventing abnormal
movement strategies, and preventing mechanical complications after surgery. The goals of
rehabilitation in dogs with CR before surgery
and in dogs with CR that are managed without
surgery are similar to the goals listed above,
with emphasis on providing pain management,
promoting controlled limb use, preventing
abnormal movement strategies, preventing and
recovering from a loss of muscle mass, and
from changes in posture resulting from chronic
pain and limb disuse. Re-evaluations during
recovery are used to monitor progress towards
rehabilitation goals and adjust rehabilitation
priorities.
Pain relief
Little is known about the pain resulting from
CR in dogs. While all agree that dogs with CR
experience pain, there is no specific information regarding the neuropathology associated
with cruciate ligament fiber damage or rupture.
In dogs with hip dysplasia, cyclooxygenase-1
(COX-1), COX-2, and lipooxygenase concentrations in the femoral head are increased, as is
the concentration of COX-2 in the hip joint capsule (Lascelles et al. 2009). Similar assessment in
Advances in the Canine Cranial Cruciate Ligament, Second Edition. Edited by Peter Muir. © 2018 ACVS Foundation.
This Work is a co-publication between the American College of Veterinary Surgeons Foundation and Wiley-Blackwell.
343
VetBooks.ir
344
Medical Management of Cruciate Ligament Rupture
the dog stifle and human knee is lacking. Clinically, the signs of CR vary widely in dogs. Subjectively, dogs that are affected bilaterally shift
their weight cranially more than dogs that are
unilaterally affected. While dogs with a large
amount of cranial tibial thrust during weightbearing are most often very lame, the presence
of dysfunction in dogs with CR does not correlate highly with the amount of stifle instability. Other than instability, the presence of a tear
or fold in the caudal horn of the meniscus, the
presence of severe synovitis, and the presence of
osteoarthritis may be other factors causing pain
and dysfunction. Dogs may also perceive acuteon-chronic pain after surgery. In one report, 30%
of dogs had chronic pain after surgical treatment of CR (Mölsa et al. 2013).
Eliminating postoperative edema
Limb edema is a source of postoperative pain
and a potential factor promoting limb disuse
during the early postoperative period. Edema
typically subsides within 10 days; simple strategies, such as cold therapy, minimize its severity
and accelerate its resolution. A decrease in the
invasiveness of surgery decreases the severity
of edema. Edema resorption is promoted by elevation of the limb extremity, gentle tissue massage, passive range of motion and stretching,
cold therapy, and by the use of electrical stimulation (Rexing et al. 2010; Drygas et al. 2011).
Maintaining or recovering stifle joint
motion
Stifle extension is more critical to correct limb
use than stifle flexion because the functional
range of motion of the stifle requires near full
extension but occurs far from full flexion. Stifle
joint extension may be negatively impacted by
capsular or periarticular fibrosis that developed
before surgery (Figure 42.1). Extension may be
further impacted by the suboptimal placement
of an extracapsular stabilization suture. Subjectively, the most common surgical error leading
to a loss of stifle extension is the excessively
distal placement of the tibial tunnel. This problem may subside over time due to loss of stiffness of the extracapsular stabilization suture
as a result of cyclic loading and the potential
Figure 42.1 This 4-year-old Great Dane had a cruciate
ligament rupture that was managed conservatively,
leading to joint fibrosis and a loss of stifle joint extension.
At the time of presentation, he was non weight-bearing
on his left pelvic limb and stifle extension was limited to
134◦ , corresponding to a ∼30◦ loss of extension. Therapy
initially focused on preheating the joint and stretching the
joint manually.
enlargement of bone tunnels. Surgical procedures that alter the tibial plateau slope or displace the tibial crest do not alter stifle joint
motion since they do not include a femorotibial tether (Jandi & Schulman 2007). Stifle joint
motion should be measured with a goniometer before surgery whenever possible, particularly before extracapsular stabilization to differentiate a chronic loss of joint motion from acute
loss of joint motion caused by the surgical procedure.
Promoting controlled limb use
Limb use after CR stabilization surgery ranges
from good (mild weight-bearing lameness)
to poor (non weight-bearing lameness; Figure 42.2). Factors that are likely to lead to a
decrease in limb use include chronicity of the
problem including osteoarthritis, limb weakness and quadriceps inhibition, neuropathological changes, surgical technique (residual
instability, medial meniscal injuries), and suboptimal pain management (peripheral sensitization, allodynia). Rehabilitation strategies to
facilitate limb use include pain management,
client education regarding controlled walking,
sling use (proximal stability to promote distal mobility), and active exercises to promote
weight shifting.
Rehabilitation for Dogs with Cruciate Ligament Rupture
345
VetBooks.ir
Marsolais et al. 2002; Jerre 2009). Strengthening
exercises and a focus on normalizing muscle
activation/control via proprioceptive retraining may assist in reducing abnormal gait strategies and optimize recovery in patients with CR
(Adrian et al. 2013).
Preventing and recovering from changes
in posture resulting from chronic pain
and limb disuse
Preventing and recovering from a loss of
muscle mass and motor control
Muscle mass and neuromuscular control are
impaired in patients with CR, leading to a loss
of strength and dynamic joint stability (Risberg
et al. 2007). Controlled exercises promote limb
use, prevent loss of muscle mass, and accelerate recovery of muscle mass after CR stabilization (Figures 42.3 and 42.4) (Johnson et al. 1997;
Limb function (PVF % BW)
43
Preventing mechanical complications
after surgery
Mechanical failure can occur after all forms of
CR stabilization, and its likelihood is increased
by falls and by owners’ unwillingness or inability to control physical activity (Langenbach &
Marcellin-Little 2010). Physical rehabilitation
*#
*#
41
14
13
39
*
37
12
*
35
11
33
10
31
29
9
27
Limb function (VI % BW)
Figure 42.2 A dog is standing with a non
weight-bearing stance on his operated pelvic limb
14 days after extracapsular stabilization of his cruciate
ligament-deficient stifle joint. A non weight-bearing
stance during the subacute postoperative period is
generally the consequence of chronic pain from a
biological or mechanical problem.
Dogs with CR develop changes in posture that
include moving their center of gravity cranially
so that the loads resisted by their pelvic limbs
decrease (Figure 42.5). With time, these changes
in posture become deeply rooted. Therapeutic
exercises promote strategies to increase pelvic
limb muscle recruitment, improve motor control and proximal strength to help improve
posture.
8
25
0
6
0
Time (months after surgery)
6
Figure 42.3 Peak vertical forces (PVF) and vertical impulse (VI) relative to body weight (BW) before and 6 months after
extracapsular stabilization of the stifle joint for dogs that were exercise-restricted (dotted lines) and dogs that underwent
rehabilitation (solid lines). PVF and VI were larger 6 months after surgery compared to before s